Key Takeaways
Anemia is a reduction in red blood cells or hemoglobin that lowers the blood's oxygen-carrying capacity. It is a sign of an underlying problem, not a disease in itself [1,3].
- Anemia Symptoms and Factors Affecting Them ▾: Symptoms vary based on the rate of anemia development (acute vs. chronic) and individual characteristics (age, gender, health status). General symptoms include fatigue, weakness, pale skin, and shortness of breath. Specific disorders can present with additional signs like splenomegaly, jaundice, neurological symptoms (in B12 deficiency), or skin ulcers (in sickle cell anemia).
- Major Causes of Anemia ▾: The four major mechanisms of anemia are blood loss, reduced production (nutritional deficiency, marrow failure, or chronic disease), increased destruction (hemolysis), and abnormal red cell production [3].
- Diagnosis ▾: Diagnosis follows a stepwise approach: complete blood count and reticulocyte count first, then classification by red cell size (microcytic, normocytic, macrocytic), then targeted tests such as iron studies, B12/folate, or hemoglobin electrophoresis [3,4].
- Treatment ▾: Treatment depends on the cause. Iron-deficiency anemia responds to oral iron, often given on alternate days for better tolerance [8]. Severe sickle cell disease now has two FDA-approved gene therapies, Casgevy and Lyfgenia, both approved in December 2023 [9,10].
*Click ▾ for more information
Introduction
Anemia is the most common blood disorder worldwide [1]. In simple terms, anemia is a state in which the blood cannot carry enough oxygen to meet the body's needs. This happens when red blood cells or hemoglobin levels fall below normal for a person's age, sex, and physiological state [2]. The Global Burden of Disease 2021 study estimates that around 1.92 billion people live with anemia, and the prevalence has fallen only modestly since 1990, mainly in men [1].
This guide walks through how red cells are made, why anemia produces the symptoms it does, how clinicians classify it, and how each major type is investigated and treated.
Erythropoiesis
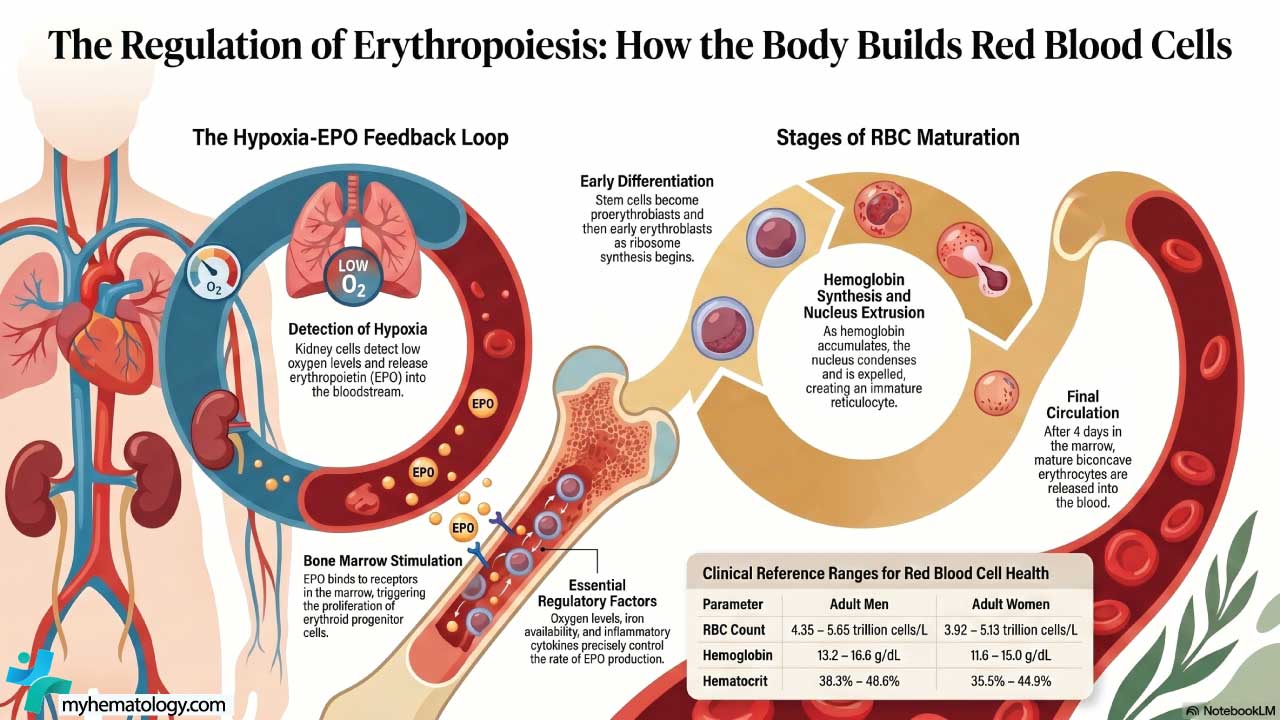
Red blood cells are produced in the bone marrow through a process called erythropoiesis (the formation of red blood cells). It starts with hematopoietic stem cells, which can either renew themselves or commit to becoming a specific blood cell type. Cells that commit to the red cell lineage divide rapidly, build hemoglobin, and finally lose their nucleus to become reticulocytes (young red cells) released into the bloodstream.
Two things drive this process:
- Erythropoietin (EPO), a hormone made by the kidneys when they sense low oxygen. EPO tells the marrow to make more red cells.
- Building blocks: iron, vitamin B12, folate, and amino acids. Without any of these, production stalls.
A new insight that older textbooks often skip is the role of hepcidin, a liver hormone that controls iron availability [7]. When hepcidin is high (as in inflammation or chronic disease), iron is locked away in stores and the marrow cannot use it, even if total body iron is normal. This is why anemia of inflammation behaves so differently from simple iron deficiency [6].
Physiology of Hemoglobin
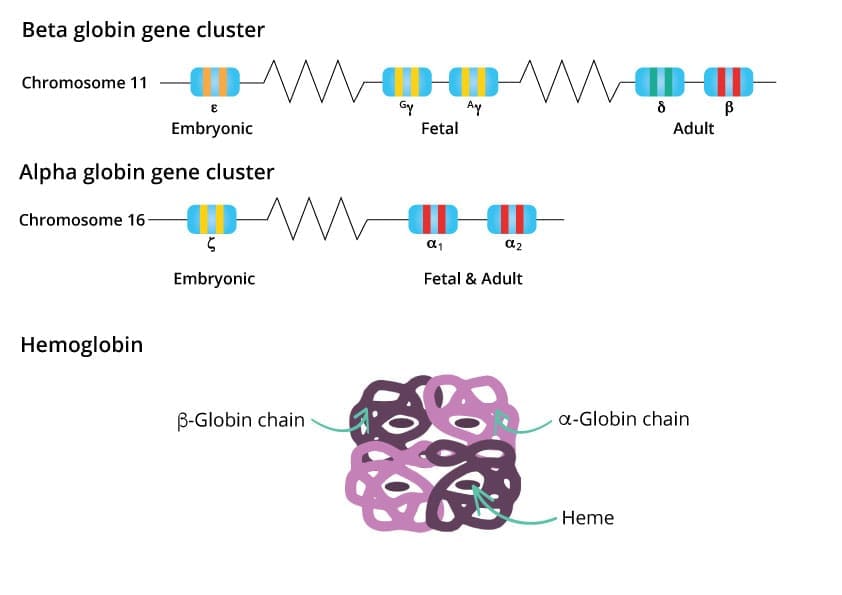
Hemoglobin is a tetramer — a protein made of four subunits. Each adult hemoglobin (HbA) molecule has two alpha and two beta globin chains, and each chain holds a heme group with one iron atom at its center [3]. The iron binds oxygen reversibly, picking it up in the lungs and releasing it in the tissues.
Normal hemoglobin levels differ slightly between sexes, mainly because of testosterone's stimulating effect on red cell production:
- Adult men: roughly 13.0–17.0 g/dL
- Non-pregnant adult women: roughly 12.0–15.5 g/dL
The 2024 WHO guideline kept most adult cutoffs but updated thresholds for children aged 6–23 months and pregnant women in the second trimester, and added formal adjustments for altitude and smoking [2]. These adjustments matter for population-level diagnosis, especially in high-altitude regions.
How the Body Compensates for Anemia
When oxygen delivery falls, the body adapts in several ways:
- The heart beats faster and pumps harder, raising cardiac output.
- Breathing rate rises, increasing oxygen uptake.
- Tissues extract more oxygen from each unit of blood than they normally would.
- Red cells produce more 2,3-DPG (2,3-diphosphoglycerate), a small molecule that lowers hemoglobin's affinity for oxygen so it releases oxygen more readily in tissues.
These adaptations explain why a slowly developing chronic anemia may produce surprisingly few symptoms, while a sudden drop in hemoglobin can cause severe distress at a much higher Hb level.
Anemia Symptoms
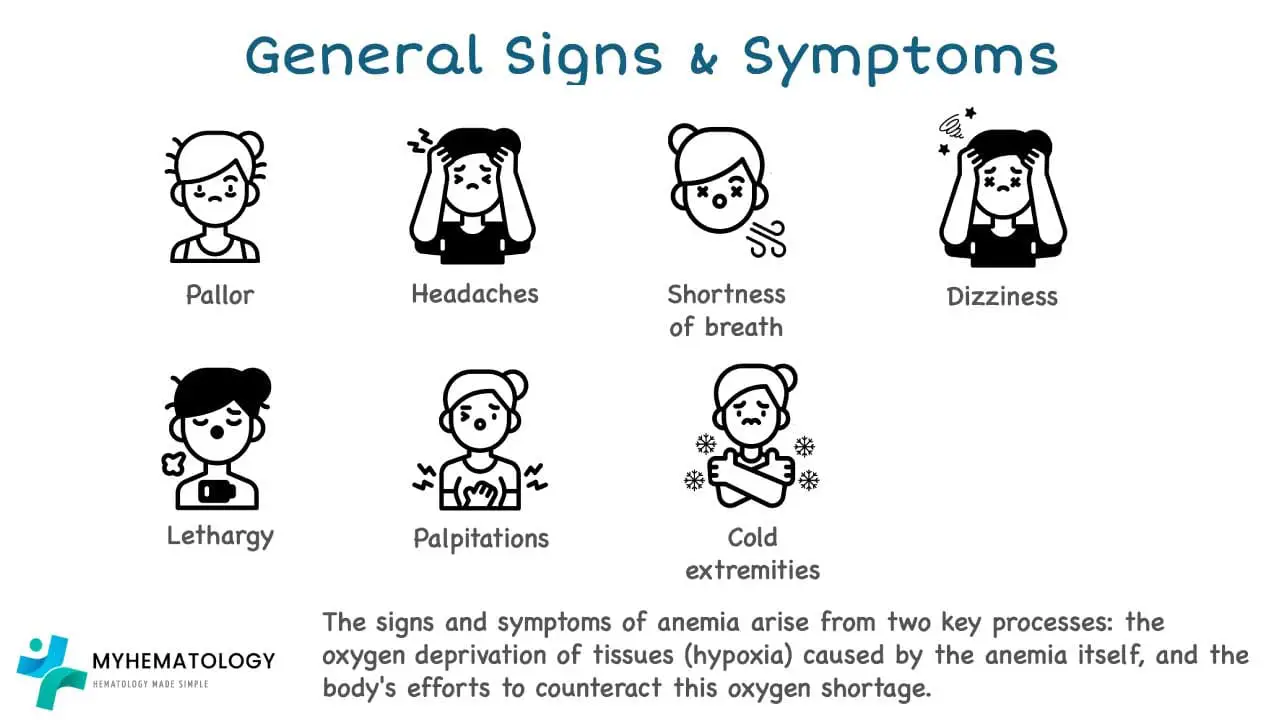
General symptoms
The most common symptoms are fatigue, pale skin and mucous membranes, breathlessness on exertion, palpitations, dizziness, and headache. Severity depends less on the absolute hemoglobin and more on how fast it dropped, how active the person is, and whether they have heart or lung disease [3].
In older adults, anemia symptoms are often blamed on aging or other illnesses, which delays diagnosis. Persistent unexplained fatigue in any adult is worth a blood count.
Symptoms that hint at the cause
Some signs point toward a specific mechanism rather than anemia in general:
- Iron deficiency: koilonychia (spoon-shaped nails), pica (craving non-food substances such as ice or clay), glossitis (smooth, sore tongue), and angular cheilitis.
- Vitamin B12 deficiency: numbness or tingling in the hands and feet, balance problems, memory difficulty, and mood changes. These reflect damage to the myelin sheath around nerves and can be irreversible if treatment is delayed [3].
- Hemolytic anemia: jaundice (yellow skin and eyes), dark urine, gallstones from chronic bilirubin overload, and an enlarged spleen.
- Sickle cell disease: episodes of severe pain (vaso-occlusive crises), leg ulcers, and a heightened risk of stroke and infection.
- Thalassemia major: bony changes including maxillary prominence ("chipmunk facies") and frontal bossing in untreated children, due to marrow expansion under the strain of ineffective erythropoiesis.
- Bone marrow failure (e.g., aplastic anemia): not just anemia, but also easy bruising, bleeding, and frequent infections, because all three blood cell lines fall together.
Classifying Anemia
Two classifications are used in practice, and both are useful.
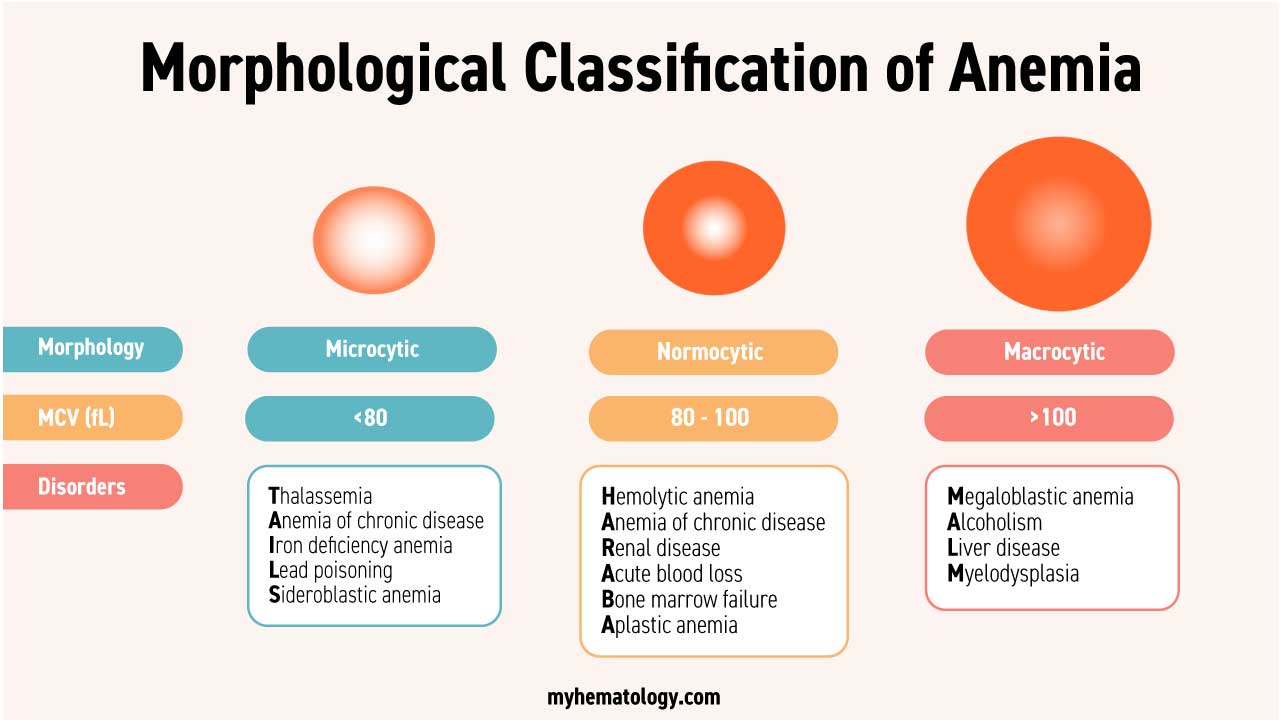
By red cell size (morphological classification)
This is the most common starting point because the mean corpuscular volume (MCV) comes free with every CBC.
- Microcytic (small cells, MCV < 80 fL): most often iron-deficiency anemia, thalassemia, anemia of chronic disease, and rarely sideroblastic anemia.
- Normocytic (normal-sized cells, MCV 80–100 fL): acute blood loss, anemia of chronic disease, early iron deficiency, hemolysis, marrow failure, and chronic kidney disease.
- Macrocytic (large cells, MCV > 100 fL): vitamin B12 or folate deficiency, alcohol use, liver disease, hypothyroidism, and some marrow disorders like myelodysplastic syndromes.
A peripheral blood smear adds detail like anisocytosis (variable size), poikilocytosis (variable shape), polychromasia (young cells), spherocytes, sickle cells, and target cells each narrow the differential.
By severity (current WHO classification for non-pregnant adults)
- Mild: 11.0–11.9 g/dL (women) or 11.0–12.9 g/dL (men)
- Moderate: 8.0–10.9 g/dL
- Severe: below 8.0 g/dL
Different cutoffs apply to children and pregnant women, and the 2024 update also added altitude and smoking adjustments [2]. Severity guides urgency, not cause.
Red Cell Balance Sheet
Red cells live about 120 days. The marrow continuously replaces them, and reticulocytes are the marker of that replacement. A normal reticulocyte percentage is about 0.5–2.0%.
In anemia, the raw percentage is misleading because the denominator (total red cells) is low. Corrected reticulocyte count should be used:
Corrected reticulocyte count = Reticulocyte % × (Patient's Hct ÷ Normal Hct)
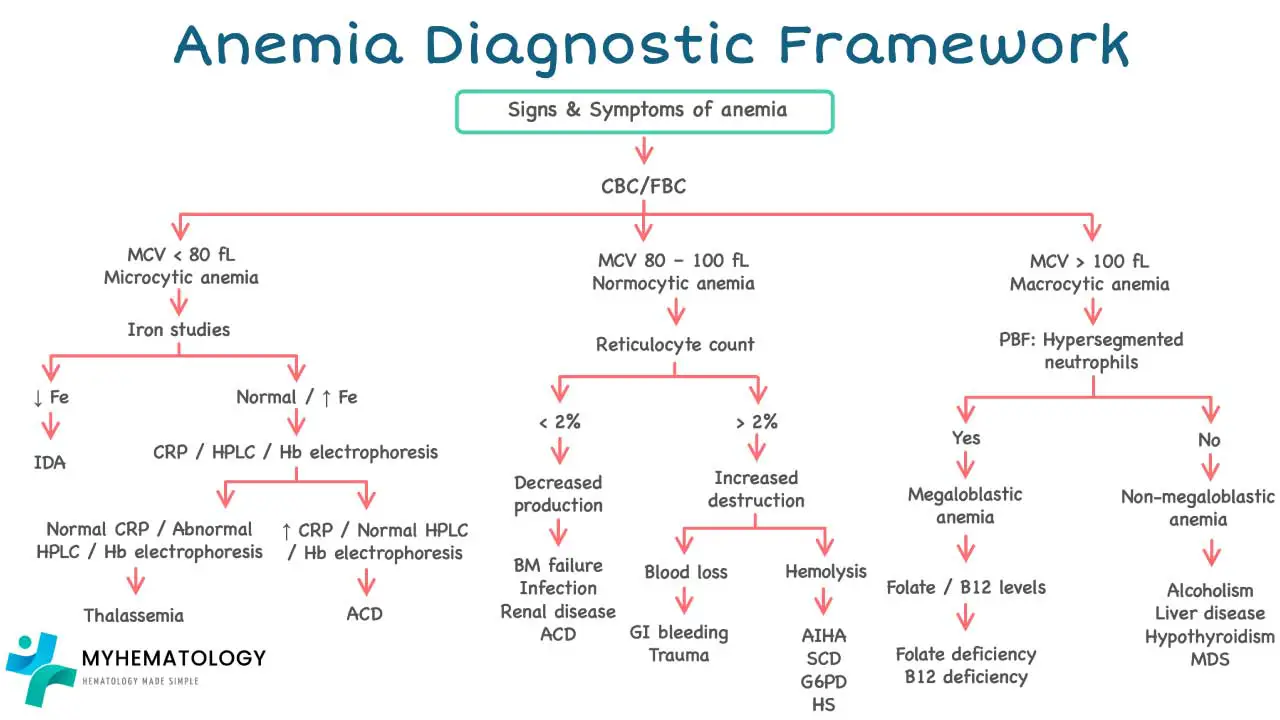
A corrected count above ~2% suggests the marrow is responding (think hemolysis or recent blood loss). A corrected count below 2% suggests the marrow is the problem (think nutritional deficiency, chronic disease, or marrow failure) [3]. This single calculation reorganizes the entire differential diagnosis and is one of the most exam-relevant points in the topic.
The Four Main Causes of Anemia
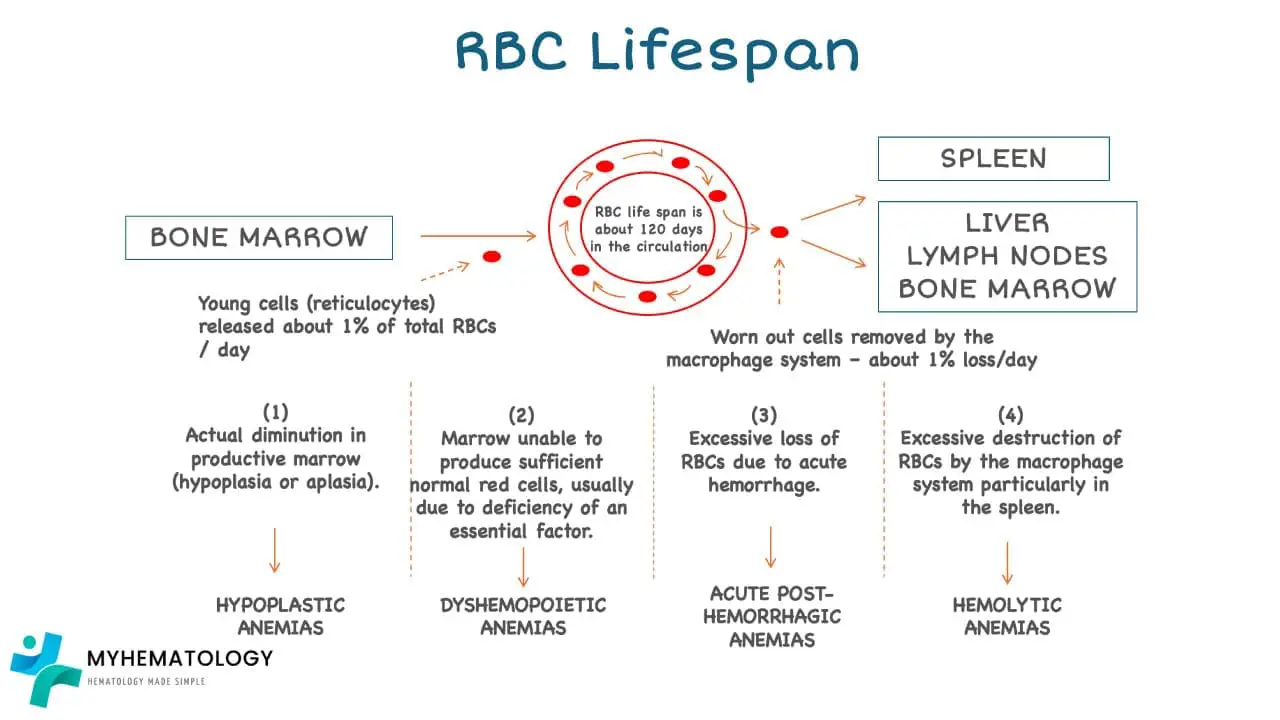
1. Blood loss
Acute blood loss from trauma, surgery, ruptured ectopic pregnancy, or severe gastrointestinal bleeding drops hemoglobin quickly and may need transfusion before iron stores are even tested. Chronic, low-volume blood loss is sneakier: heavy menstrual periods, slow ulcer bleeding, hemorrhoids, colon polyps, hookworm, or long-term NSAID use can quietly drain iron stores until iron-deficiency anemia develops [4].
In any adult with new iron deficiency and no obvious source, gastrointestinal evaluation is the standard of care to rule out occult malignancy.
2. Nutritional deficiency
Iron deficiency is the most common nutritional cause of anemia worldwide [4]. Risk factors include low dietary iron (especially from plant-only diets without fortification), heavy menstruation, pregnancy, infancy and adolescence, and malabsorption (celiac disease, post-bariatric surgery, H. pylori gastritis). The classic blood picture is microcytic, hypochromic red cells with low ferritin and high transferrin [5].
Vitamin B12 deficiency classically produces a macrocytic anemia with neurological signs. The most common cause is impaired absorption due to pernicious anemia (autoimmune loss of intrinsic factor), atrophic gastritis, ileal disease, long-term metformin or proton-pump inhibitor use, and strict vegan diets without supplementation.
Folate deficiency also produces macrocytic anemia but without the neurological signs. Causes include poor diet, alcohol use, malabsorption, pregnancy, and certain drugs (methotrexate, phenytoin).
3. Reduced or abnormal marrow production
This category includes anemia of chronic disease (also called anemia of inflammation), bone marrow failure syndromes, and renal anemia.
Anemia of chronic disease is the second most common anemia globally and is driven largely by hepcidin [6,7]. Inflammation raises hepcidin, which traps iron inside macrophages and intestinal cells, starving the marrow of usable iron despite normal or high stores. It commonly accompanies infections, autoimmune disease, cancer, and chronic kidney disease.
Bone marrow failure includes aplastic anemia (immune-mediated destruction of stem cells in most cases), myelodysplastic syndromes (clonal disorders producing dysfunctional cells), and inherited syndromes such as Fanconi anemia and Diamond-Blackfan anemia. These typically affect more than one cell line.
Renal anemia results from low erythropoietin production by failing kidneys and is treated with erythropoiesis-stimulating agents and IV iron.
4. Increased destruction (hemolysis)
In hemolytic anemia, red cells are destroyed faster than the marrow can replace them. Causes split into:
- Inherited intrinsic defects: sickle cell disease, thalassemia, hereditary spherocytosis (most cases autosomal dominant), and G6PD deficiency (X-linked, more common in males).
- Acquired causes: autoimmune hemolytic anemia (warm or cold antibody type), drug-induced hemolysis, microangiopathic hemolysis (TTP, HUS, DIC), paroxysmal nocturnal hemoglobinuria, and infections such as malaria.
The hallmark laboratory pattern is anemia plus a high reticulocyte count, raised LDH, raised unconjugated bilirubin, and low haptoglobin. The direct antiglobulin test (Coombs test) separates immune from non-immune causes [3].
How Anemia is Investigated
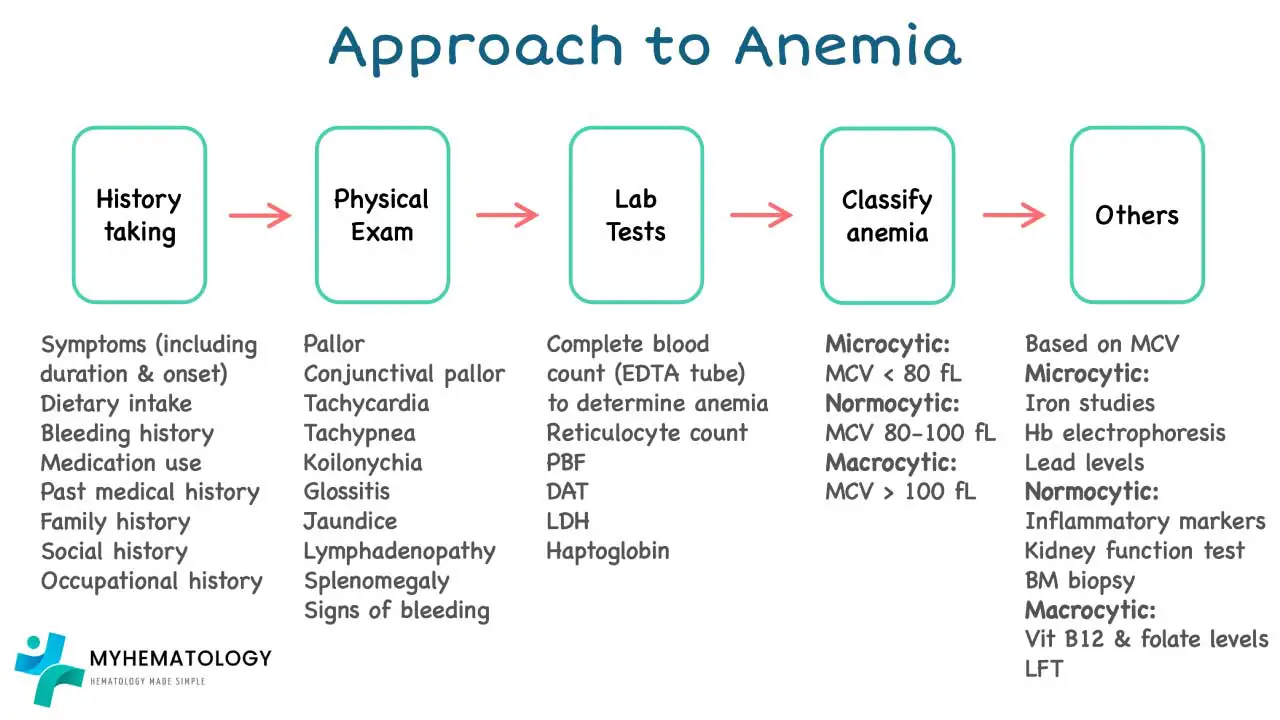
A clean, stepwise approach helps both diagnosis and exam questions:
- Confirm anemia and grade severity with a CBC and hemoglobin level.
- Look at the MCV to classify as microcytic, normocytic, or macrocytic.
- Check the reticulocyte count (corrected) to decide whether the marrow is responding or not.
- Order targeted tests based on those results:
- Microcytic, low retics → iron studies (ferritin, transferrin saturation), and consider thalassemia screen if iron studies are normal.
- Macrocytic, low retics → vitamin B12 and folate, thyroid function, liver tests, blood film for megaloblastic features.
- Normocytic, low retics → renal function, inflammatory markers, and consider bone marrow examination if unexplained.
- High retics → hemolysis screen (LDH, bilirubin, haptoglobin, blood film, direct antiglobulin test), hemoglobin electrophoresis if a hemoglobinopathy is suspected.
- When interpreting iron studies, specific diagnostic thresholds are crucial. A serum ferritin level below 30 ng/mL is universally diagnostic of absolute iron deficiency. However, because ferritin is an acute-phase reactant, patients with concurrent inflammation or chronic disease may be severely iron deficient even with a ferritin level up to 100 ng/mL [15]. To navigate these diagnostic gray areas, clinicians use the soluble transferrin receptor (sTfR) assay. The bone marrow sheds more sTfR when it is starved for iron; therefore, sTfR is significantly elevated in true iron deficiency but remains normal in the anemia of chronic disease [17]. Furthermore, measuring the reticulocyte hemoglobin equivalent (Ret-He) provides a real-time snapshot of the bone marrow's iron availability over the preceding 48 hours, offering a much faster diagnostic reflection than traditional indices like the mean corpuscular volume [13].
- Look for blood loss in any unexplained iron deficiency, especially in adults.
A peripheral blood film remains a high-yield, low-cost test that often points directly at the cause.

How Anemia Is Treated
Treatment always targets the cause. A few principles cover most clinical situations:
Iron-deficiency anemia. Oral iron remains first line. Recent guidelines from the American College of Gastroenterology and the European Hematology Association recommend alternate-day dosing because it improves absorption (by avoiding hepcidin spikes) and reduces gastrointestinal side effects compared to daily dosing [8]. Historically, intravenous (IV) iron like such as ferric carboxymaltose or ferric derisomaltose was reserved as a fallback when oral iron failed or was poorly tolerated. However, in contemporary practice, upfront single-dose IV iron is increasingly recognized as a first-line therapy for specific high-risk populations. This includes patients with inflammatory bowel disease, those requiring rapid optimization prior to major surgery, and patients with symptomatic heart failure with reduced ejection fraction, where IV iron has been shown to significantly improve functional capacity and reduce the risk of heart failure-related hospitalizations [16,18].
B12 and folate deficiency. Replace the deficient vitamin. B12 is given as injections in malabsorption and orally otherwise. Folate is replaced orally, but importantly, never give folate alone if B12 deficiency has not been excluded as it can mask the anemia while neurological damage progresses.
Anemia of chronic disease. Treat the underlying condition. In selected cases (chronic kidney disease, some cancers), erythropoiesis-stimulating agents combined with IV iron are used [6]. For patients with chronic kidney disease (CKD), a major pharmacological breakthrough is the recent introduction of oral hypoxia-inducible factor prolyl hydroxylase (HIF-PH) inhibitors, such as daprodustat. These agents trick the body into mimicking a high-altitude hypoxia response, which stabilizes the HIF protein. This stimulates the patient's own kidneys and liver to produce endogenous erythropoietin while simultaneously suppressing hepcidin levels to mobilize trapped iron stores [19].
Hemolytic anemia. Autoimmune hemolytic anemia is treated with corticosteroids, rituximab, or other immunosuppressants; splenectomy is reserved for refractory cases. Hereditary spherocytosis may also be helped by splenectomy. Folate supplementation is usually added because rapid red cell turnover increases demand.
Sickle cell disease. Hydroxyurea remains the workhorse, supported by L-glutamine, transfusion programs, and pain management. Since December 2023, two FDA-approved gene therapies have changed the landscape for severe sickle cell disease in patients aged 12 and older: Casgevy (exagamglogene autotemcel), the first CRISPR-Cas9 therapy ever approved, which boosts fetal hemoglobin by editing the BCL11A gene, and Lyfgenia (lovotibeglogene autotemcel), a lentiviral gene therapy that adds an anti-sickling β-globin gene [9,10]. Both require myeloablative conditioning and specialized centers, and access remains a major issue. Beyond gene therapy and hydroxyurea, daily medical management for sickle cell disease has expanded with the use of voxelotor, a first-in-class oral hemoglobin oxygen-affinity modulator. Voxelotor physically prevents deoxygenated hemoglobin S from polymerizing and sickling, which significantly raises hemoglobin levels and reduces markers of chronic hemolysis [20].
Transfusion-dependent thalassemia and lower-risk MDS. Luspatercept is an erythroid maturation agent that has reduced transfusion burden in both conditions [12].
Pyruvate kinase (PK) deficiency. For this rare inherited hemolytic anemia, mitapivat (a first-in-class oral PK activator) directly addresses the underlying enzymatic deficit. It improves the metabolic health of erythrocytes, significantly decreasing hemolysis and reducing the need for regular red-cell transfusions [14].
Severe or symptomatic anemia. Red cell transfusion may be needed regardless of cause. Modern practice favors restrictive transfusion thresholds (typically Hb < 7 g/dL in stable adults, higher in cardiac disease) rather than treating a number.
Anemia in Pregnancy and Childhood
Anemia in pregnancy raises the risk of preterm birth, low birth weight, and maternal complications, and routine antenatal screening with iron and folate supplementation is standard [11]. The 2024 WHO update revised the second-trimester hemoglobin cutoff to better reflect physiological hemodilution [2].
In children under five, iron-deficiency anemia is linked to impaired cognitive and motor development that may not fully reverse, even after iron is replaced [1]. This is why iron supplementation programs and food fortification are public-health priorities in many countries.
Why This Matters for Caregivers
If you are caring for someone with anemia, a few practical points help:
- Take symptoms seriously, especially in older adults and pregnant women.
- Iron tablets work best on an empty stomach but are gentler with food. Vitamin C improves absorption; tea, coffee, and calcium supplements reduce it.
- Most iron-deficiency anemia takes weeks to correct and several months more to refill stores. Stopping iron at the first normal hemoglobin is the most common cause of relapse.
- Seek urgent care for chest pain, fainting, severe shortness of breath, dark or red urine, or sudden severe pain in someone with sickle cell disease.
Glossary of Related Medical Terms
- Anemia — A reduction in the number of red blood cells or in the amount of hemoglobin, which lowers how much oxygen the blood can carry.
- Hemoglobin (Hb) — The iron-containing protein inside red blood cells that binds and carries oxygen.
- Erythropoiesis — The process by which the bone marrow makes new red blood cells.
- Erythropoietin (EPO) — A hormone made by the kidneys that signals the bone marrow to produce more red cells when oxygen is low.
- Hepcidin — A liver hormone that controls how much iron is absorbed from food and released from body stores; high hepcidin lowers available iron.
- Reticulocyte — A young red blood cell just released from the marrow; the count tells you whether the marrow is producing new cells well.
- Mean corpuscular volume (MCV) — The average size of a red blood cell, used to classify anemia as microcytic (small), normocytic (normal), or macrocytic (large).
- Microcytic / macrocytic / normocytic — Refers to red cells that are smaller than, larger than, or the same size as normal.
- Hemolysis — The breakdown of red blood cells; can happen inside vessels (intravascular) or in the spleen and liver (extravascular).
- Bilirubin — A yellow pigment released when red blood cells break down; high levels cause jaundice.
- Pancytopenia — A drop in all three blood cell types: red cells, white cells, and platelets.
- Hydroxyurea — A medication used in sickle cell disease that increases fetal hemoglobin and reduces painful crises.
- Vaso-occlusive crisis — Episodes of severe pain in sickle cell disease caused by sickled red cells blocking small blood vessels.
- Thrombocytopenia — A low platelet count.
- Splenomegaly / hepatomegaly — Enlargement of the spleen or liver.
Frequently Asked Questions (FAQs)
Is anemia dangerous?
Mild anemia is rarely dangerous on its own, but moderate to severe anemia strains the heart, impairs concentration and exercise tolerance, and can be life-threatening if it develops suddenly. Anemia is also frequently a clue to another illness like a bleeding ulcer, a malignancy, kidney disease so the underlying cause matters as much as the hemoglobin number itself.
Can anemia cause hair loss?
Yes. Iron-deficiency anemia is associated with diffuse hair shedding (telogen effluvium) and brittle hair. Hair growth typically recovers once iron stores are replenished, which can take several months.
Can anemia cause pain?
Anemia itself often causes headaches from reduced oxygen delivery to the brain. In sickle cell disease, severe pain crises occur when sickled cells block small vessels. In thalassemia, expansion of the marrow can cause bone pain. Anemia of chronic disease may also produce joint or muscle pain through the underlying inflammation rather than the anemia directly.
How long does it take to recover from anemia?
Iron-deficiency anemia usually shows a measurable hemoglobin rise within 2–4 weeks of starting iron, but full repletion of body iron stores takes another 3–6 months. B12 and folate replacement work faster on the blood count but neurological recovery from B12 deficiency may be slower or incomplete. Inherited anemias such as sickle cell and thalassemia are managed long-term rather than cured, except where curative options like stem cell transplant or gene therapy are appropriate.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- GBD 2021 Anaemia Collaborators (2023). Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990-2021: findings from the Global Burden of Disease Study 2021. The Lancet. Haematology, 10(9), e713–e734. https://doi.org/10.1016/S2352-3026(23)00160-6
- Guideline on haemoglobin cutoffs to define anaemia in individuals and populations [Internet]. Geneva: World Health Organization; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK602198/
- Turner J, Parsi M, Badireddy M. Anemia. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499994/
- Jogu P, Kamran MT. Iron-Deficiency Anemia(Archived) [Updated 2026 Feb 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448065
- Camaschella C. (2019). Iron deficiency. Blood, 133(1), 30–39. https://doi.org/10.1182/blood-2018-05-815944
- Weiss, G., Ganz, T., & Goodnough, L. T. (2019). Anemia of inflammation. Blood, 133(1), 40–50. https://doi.org/10.1182/blood-2018-06-856500
- Ganz T. (2013). Systemic iron homeostasis. Physiological reviews, 93(4), 1721–1741. https://doi.org/10.1152/physrev.00008.2013
- Stoffel, N. U., Cercamondi, C. I., Brittenham, G., Zeder, C., Geurts-Moespot, A. J., Swinkels, D. W., Moretti, D., & Zimmermann, M. B. (2017). Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. The Lancet. Haematology, 4(11), e524–e533. https://doi.org/10.1016/S2352-3026(17)30182-5
- Frangoul, H., Altshuler, D., Cappellini, M. D., Chen, Y. S., Domm, J., Eustace, B. K., Foell, J., de la Fuente, J., Grupp, S., Handgretinger, R., Ho, T. W., Kattamis, A., Kernytsky, A., Lekstrom-Himes, J., Li, A. M., Locatelli, F., Mapara, M. Y., de Montalembert, M., Rondelli, D., Sharma, A., … Corbacioglu, S. (2021). CRISPR-Cas9 Gene Editing for Sickle Cell Disease and β-Thalassemia. The New England journal of medicine, 384(3), 252–260. https://doi.org/10.1056/NEJMoa2031054
- Kanter, J., Walters, M. C., Krishnamurti, L., Mapara, M. Y., Kwiatkowski, J. L., Rifkin-Zenenberg, S., Aygun, B., Kasow, K. A., Pierciey, F. J., Jr, Bonner, M., Miller, A., Zhang, X., Lynch, J., Kim, D., Ribeil, J. A., Asmal, M., Goyal, S., Thompson, A. A., & Tisdale, J. F. (2022). Biologic and Clinical Efficacy of LentiGlobin for Sickle Cell Disease. The New England journal of medicine, 386(7), 617–628. https://doi.org/10.1056/NEJMoa2117175
- Anemia in Pregnancy: ACOG Practice Bulletin, Number 233. (2021). Obstetrics and gynecology, 138(2), e55–e64. https://doi.org/10.1097/AOG.0000000000004477
- Cappellini, M. D., Viprakasit, V., Taher, A. T., Georgiev, P., Kuo, K. H. M., Coates, T., Voskaridou, E., Liew, H. K., Pazgal-Kobrowski, I., Forni, G. L., Perrotta, S., Khelif, A., Lal, A., Kattamis, A., Vlachaki, E., Origa, R., Aydinok, Y., Bejaoui, M., Ho, P. J., Chew, L. P., … BELIEVE Investigators (2020). A Phase 3 Trial of Luspatercept in Patients with Transfusion-Dependent β-Thalassemia. The New England journal of medicine, 382(13), 1219–1231. https://doi.org/10.1056/NEJMoa1910182
- Almashjary, M. N., Barefah, A. S., Bahashwan, S., Ashankyty, I., ElFayoumi, R., Alzahrani, M., Assaqaf, D. M., Aljabri, R. S., Aljohani, A. Y., Muslim, R., Baawad, S. A., Bawazir, W. M., & Alharthy, S. A. (2022). Reticulocyte Hemoglobin-Equivalent Potentially Detects, Diagnoses and Discriminates between Stages of Iron Deficiency with High Sensitivity and Specificity. Journal of clinical medicine, 11(19), 5675. https://doi.org/10.3390/jcm11195675
- Al-Samkari, H., Galactéros, F., Glenthøj, A., Rothman, J. A., Andres, O., Grace, R. F., Morado-Arias, M., Layton, D. M., Onodera, K., Verhovsek, M., Barcellini, W., Chonat, S., Judge, M. P., Zagadailov, E., Xu, R., Hawkins, P., Beynon, V., Gheuens, S., van Beers, E. J., & ACTIVATE Investigators (2022). Mitapivat versus Placebo for Pyruvate Kinase Deficiency. The New England journal of medicine, 386(15), 1432–1442. https://doi.org/10.1056/NEJMoa2116634
- DeLoughery, T. G., Jackson, C. S., Ko, C. W., & Rockey, D. C. (2024). AGA Clinical Practice Update on Management of Iron Deficiency Anemia: Expert Review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association, 22(8), 1575–1583. https://doi.org/10.1016/j.cgh.2024.03.046
- Graham, F. J., Guha, K., Cleland, J. G., & Kalra, P. R. (2024). Treating iron deficiency in patients with heart failure: what, why, when, how, where and who. Heart (British Cardiac Society), 110(20), 1201–1207. https://doi.org/10.1136/heartjnl-2022-322030
- Kılıç, M., Özpınar, A., Serteser, M., Kilercik, M., & Serdar, M. (2022). The effect of reticulocyte hemoglobin content on the diagnosis of iron deficiency anemia: A meta-analysis study. Journal of medical biochemistry, 41(1), 1–13. https://doi.org/10.5937/jomb0-31435
- Ponikowski, P., van Veldhuisen, D. J., Comin-Colet, J., Ertl, G., Komajda, M., Mareev, V., McDonagh, T., Parkhomenko, A., Tavazzi, L., Levesque, V., Mori, C., Roubert, B., Filippatos, G., Ruschitzka, F., Anker, S. D., & CONFIRM-HF Investigators (2015). Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency†. European heart journal, 36(11), 657–668. https://doi.org/10.1093/eurheartj/ehu385
- Singh, A. K., Carroll, K., McMurray, J. J. V., Solomon, S., Jha, V., Johansen, K. L., Lopes, R. D., Macdougall, I. C., Obrador, G. T., Waikar, S. S., Wanner, C., Wheeler, D. C., Więcek, A., Blackorby, A., Cizman, B., Cobitz, A. R., Davies, R., DiMino, T. L., Kler, L., Meadowcroft, A. M., … ASCEND-ND Study Group (2021). Daprodustat for the Treatment of Anemia in Patients Not Undergoing Dialysis. The New England journal of medicine, 385(25), 2313–2324. https://doi.org/10.1056/NEJMoa2113380
- Vichinsky, E., Hoppe, C. C., Ataga, K. I., Ware, R. E., Nduba, V., El-Beshlawy, A., Hassab, H., Achebe, M. M., Alkindi, S., Brown, R. C., Diuguid, D. L., Telfer, P., Tsitsikas, D. A., Elghandour, A., Gordeuk, V. R., Kanter, J., Abboud, M. R., Lehrer-Graiwer, J., Tonda, M., Intondi, A., … HOPE Trial Investigators (2019). A Phase 3 Randomized Trial of Voxelotor in Sickle Cell Disease. The New England journal of medicine, 381(6), 509–519. https://doi.org/10.1056/NEJMoa1903212


