Key Takeaways
Iron deficiency anemia is the most common nutritional deficiency worldwide. It develops when the body lacks the iron necessary to produce adequate hemoglobin, causing red blood cells to become smaller, paler, and less capable of carrying oxygen to tissues.
- Iron deficiency symptoms & signs ▾: The most common presentations include fatigue, pale skin, shortness of breath upon exertion, and dizziness. Severe deficiency can trigger more distinct signs, such as brittle, koilonychia, pica, restless legs syndrome, and noticeable hair shedding.
- Causes ▾: Heavy menstrual bleeding, chronic gastrointestinal blood loss, pregnant women, young children consuming excess cow's milk, individuals on plant-based diets, and patients with malabsorption conditions.
- Laboratory Investigations & Diagnosis ▾: A complete blood count (CBC) typically reveals low hemoglobin with hypochromic microcytic red cells. Iron studies are necessary to confirm the diagnosis. However, treating it without addressing the underlying source of blood loss or malabsorption will inevitably lead to recurrence.
- Iron deficiency treatment and management ▾: Oral iron supplements (typically 60 to 120 mg of elemental iron) are the standard first-line treatment. Intravenous (IV) iron is the preferred choice when oral iron is poorly tolerated, when the gut cannot absorb it properly, or when rapid replacement is clinically necessary.
*Click ▾ for more information
What is Iron Deficiency Anemia?
Iron deficiency anemia is the most common nutritional deficiency in the world. It affects an estimated 1.2 billion people and accounts for the majority of all anemia cases globally [1,11].
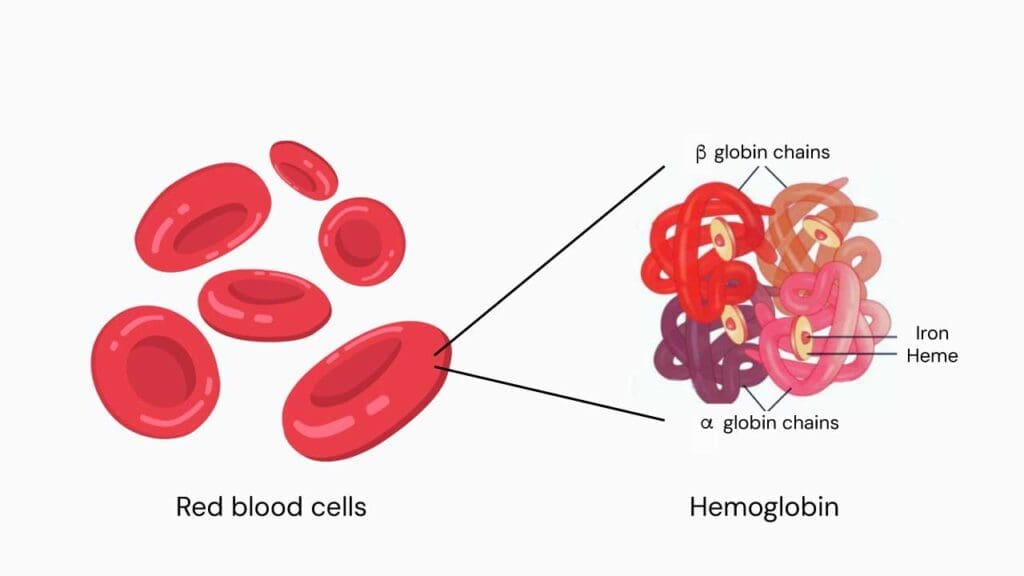
Iron deficiency anemia occurs when the body does not have enough iron to make adequate hemoglobin. Hemoglobin is the protein inside red blood cells that carries oxygen around the body. Without enough iron, hemoglobin production falls. Red blood cells become smaller and paler than normal, and the body's tissues receive less oxygen than they need [10,11].
Understanding iron deficiency anemia at this foundational level matters because it shapes every clinical decision that follows — from which tests to order to which treatments to choose.
The World Health Organization defines anemia using the following hemoglobin cutoffs [2]:
- Below 130 g/L in adult men
- Below 120 g/L in non-pregnant women
- Below 110 g/L during pregnancy
How Does the Body Regulate Iron?
Iron plays a vital role in oxygen transport, energy production, and DNA synthesis. But iron is also chemically dangerous. Free iron in the body generates harmful molecules called reactive oxygen species, which can damage cells. The body handles this by keeping nearly all of its iron tightly bound to proteins, and by regulating how much iron enters the bloodstream very precisely [13].
The hormone hepcidin is the master regulator of this entire process.
How the Body Absorbs Iron
Dietary iron comes in two forms. Heme iron is found in meat, fish, and poultry. Non-heme iron comes from plants, eggs, and dairy. Both forms are absorbed in the duodenum and the upper part of the small intestine (the jejunum), but they enter cells differently.
Non-heme iron must first be converted from an unusable form (Fe3+) into a usable form (Fe2+). This happens at the surface of the gut lining, with help from an enzyme called duodenal cytochrome b (DCYTB) and dietary vitamin C. Once converted, the iron crosses into the gut lining cell (called an enterocyte) through a transporter protein called DMT1 (divalent metal transporter 1).
Heme iron takes a simpler route. It binds to a receptor on the cell surface and enters directly, where enzymes release the iron from the heme molecule inside the cell.
Heme iron is absorbed two to three times more efficiently than non-heme iron [11,13]. This difference is why vegetarians and vegans are at higher risk of iron deficiency and need to consume more total iron through their diet.
The Hepcidin–Ferroportin Axis: Why This Matters for Treatment
Once inside the gut lining cell (or inside a recycling macrophage), iron exits into the bloodstream through the only iron export protein in the body:ferroportin [13].
Whether ferroportin stays open or gets shut down depends entirely on hepcidin. Here is how it works:
- When iron stores are low, hepcidin falls. Ferroportin stays open, and iron flows freely into the blood.
- When iron stores are high, or when the body is fighting inflammation, hepcidin rises. It binds to ferroportin, triggers its breakdown, and locks iron inside cells where it cannot be used [13].
This one mechanism explains three clinically important facts:
- Why daily oral iron is often poorly absorbed. Each iron dose raises hepcidin levels for approximately 24 hours, which blocks absorption of the next day's dose [4,5,6].
- Why chronic inflammation causes anemia. Conditions like rheumatoid arthritis, cancer, and chronic kidney disease keep hepcidin high, trapping iron inside cells even when stores are technically adequate [3,13].
- Why intravenous iron works when oral iron does not. IV iron bypasses the gut entirely, so hepcidin cannot block it.
Once in the bloodstream, iron attaches to a carrier protein called transferrin, which transports it to the bone marrow and other tissues.
How Iron Is Stored
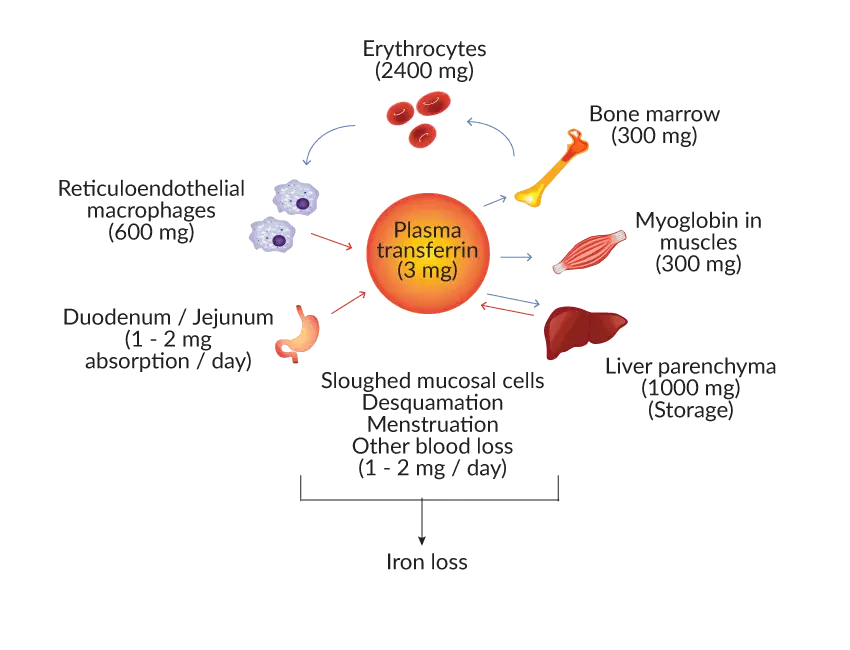
About 70 to 80% of the body's iron is functional, meaning it is actively working — mostly inside hemoglobin, but also in muscle protein (myoglobin) and in enzymes involved in energy production.
The rest is stored for later use. The main storage protein is ferritin, found in the liver, spleen, and bone marrow. A smaller amount is stored as hemosiderin, an insoluble breakdown product of ferritin [11,13].
When red blood cells reach the end of their roughly 120-day lifespan, macrophages in the spleen and liver break them down and recycle their iron. This recycling loop provides most of the iron the bone marrow needs each day. Only 1 to 2 mg per day comes from newly absorbed dietary iron.
Why the Body Cannot Simply Excrete Excess Iron
The body has no regulated pathway to remove iron once absorbed. About 1 to 2 mg is lost passively each day through shed gut and skin cells. Menstruation, pregnancy, lactation, and blood loss add to this. Because iron cannot be excreted on demand, the body must control it at the point of absorption and that control is driven entirely by hepcidin.
The Three Stages of Iron Deficiency
Iron deficiency does not appear suddenly. It develops in three overlapping stages, each representing a deeper level of iron depletion [10,11].
Stage 1 — Iron depletion. Iron stores begin to fall. The serum ferritin (a blood test that reflects stored iron) drops, typically below 30 μg/L. Hemoglobin is still normal, and red blood cell production continues unaffected. Some people feel fatigue, notice hair shedding, or experience restless legs at this stage, even before anemia develops. This stage is also called iron deficiency without anemia (IDWA) and is at least twice as common as full iron deficiency anemia [1].
Stage 2 — Iron-deficient erythropoiesis. Erythropoiesis is the process of making new red blood cells. When iron stores run out, the bone marrow starts producing red blood cells that are under-filled with hemoglobin. Ferritin remains low. Transferrin saturation (TSAT) — the proportion of the body's iron-carrier protein that is actually loaded with iron — falls below 20%. A newer lab marker called reticulocyte hemoglobin content (Ret-He or CHr), which reflects the hemoglobin content of the youngest red blood cells, also declines at this stage [12]. Hemoglobin may still sit at the lower end of the normal range.
Stage 3 — Iron deficiency anemia. This is the stage most people recognize. Hemoglobin finally drops below the normal threshold for age and sex. Red blood cells become smaller than normal (microcytic, with MCV below 80 fL) and paler than normal (hypochromic, with MCH below 27 pg). The red cell distribution width (RDW) — a measure of how variable red blood cell size is — rises. Symptoms become obvious.
Signs and Symptoms of Iron Deficiency Anemia (IDA)
Symptoms of iron deficiency anemia develop gradually. Many people adapt to declining hemoglobin over time, which means they may not realize how unwell they feel until treatment begins and they notice the difference.
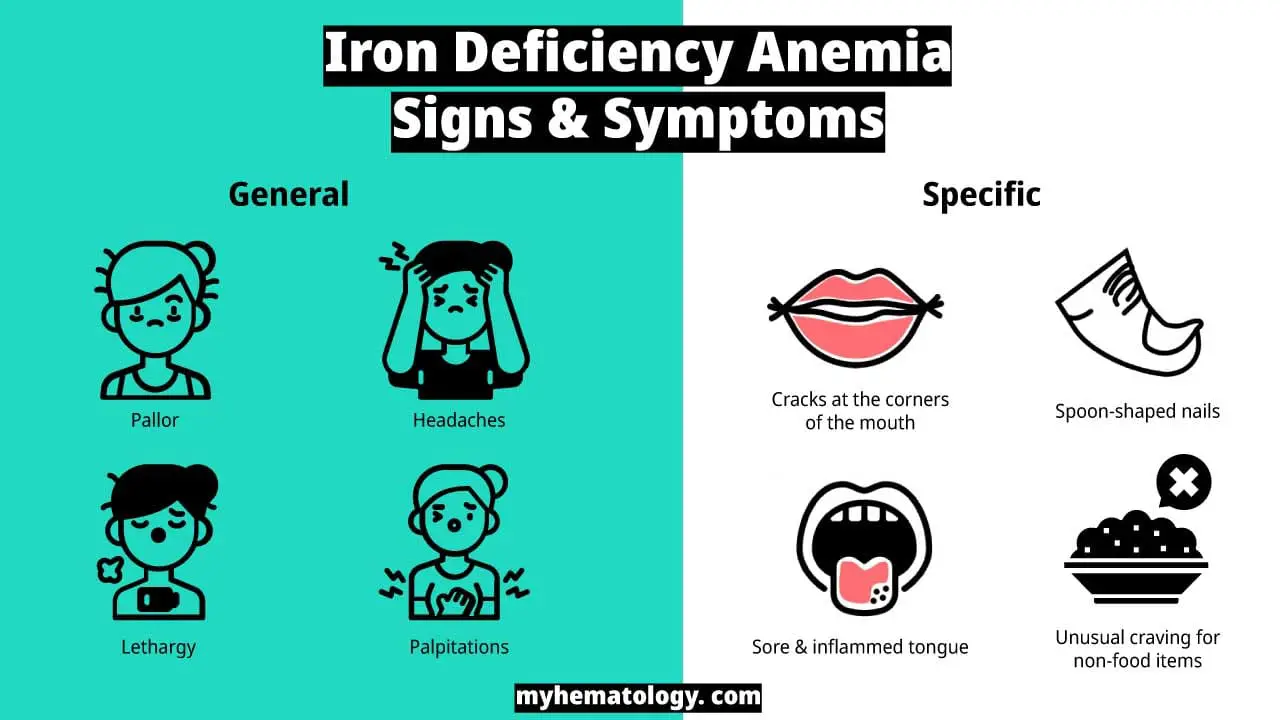
Common Symptoms
- Fatigue and reduced ability to exercise
- Pale skin, most visibly in the inner eyelids (conjunctivae), palms, and nail beds
- Shortness of breath with activity
- Dizziness or light-headedness
- Headaches
- Rapid or irregular heartbeat (palpitations or tachycardia)
- Cold hands and feet
- Difficulty concentrating
Signs of Longer-Standing or Severe Deficiency
These signs point to iron deficiency that has been present for months or longer:
- Koilonychia — thin, brittle, spoon-shaped nails
- Glossitis — a sore, smooth, pale tongue
- Angular cheilitis — painful cracks at the corners of the mouth
- Pica — an unusual craving for non-food items such as ice (a form of pica called pagophagia), clay, or paper
- Restless legs syndrome — an uncomfortable urge to move the legs, often worse at night
- Hair shedding (telogen effluvium) — noticeable increase in hair loss
- Plummer-Vinson syndrome (also called Paterson-Brown-Kelly syndrome) — a rare combination of long-standing iron deficiency anemia, difficulty swallowing, and a thin web of tissue in the upper esophagus.
It is worth noting that fatigue, hair loss, and restless legs can all appear in iron deficiency without anemia (IDWA) and respond to iron treatment [1,7]. A normal hemoglobin does not rule out clinically significant iron deficiency.
Who Is at Risk of Iron Deficiency Anemia?
Certain groups are at much higher risk than others. Understanding these risk factors helps with early identification and prevention.
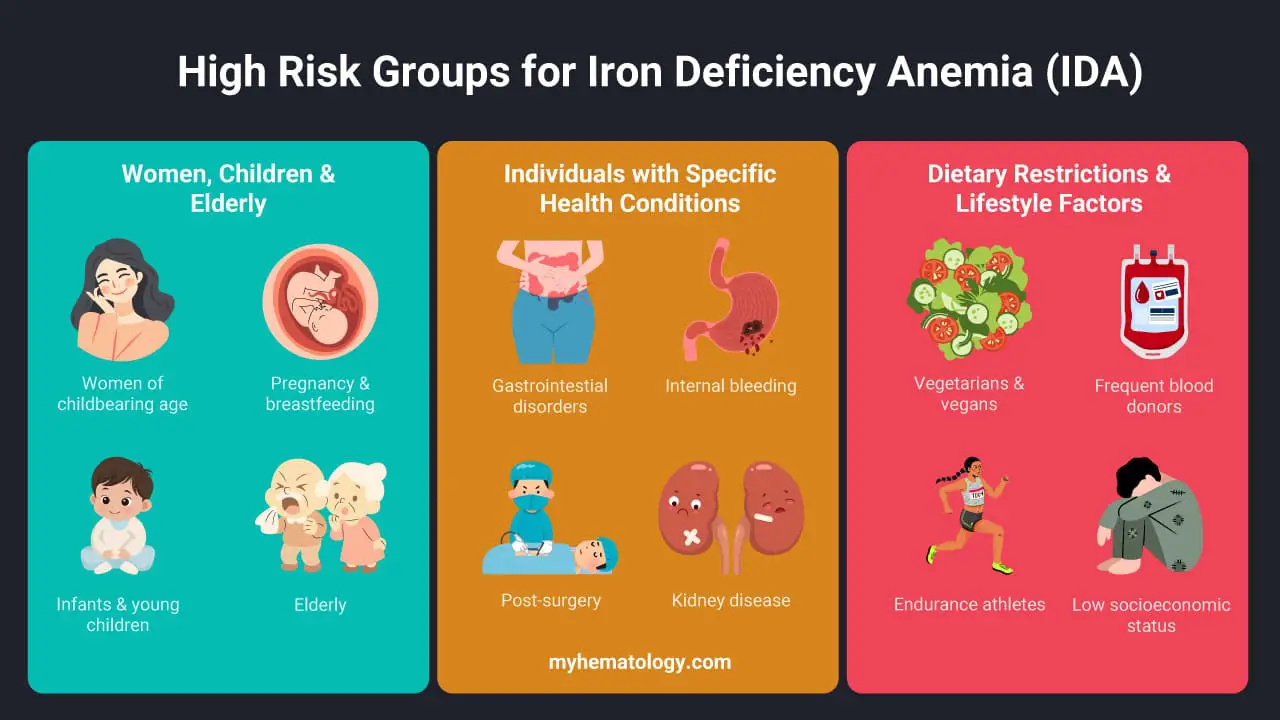
Women of Reproductive Age
Heavy menstrual bleeding is the single biggest preventable cause of iron deficiency in women in high-income countries. Bleeding that lasts more than seven days, requires changing protection more often than every two hours, or noticeably disrupts daily life should prompt iron studies. This group should be on every clinician's radar for iron deficiency anemia screening.
Pregnant and Breastfeeding Women
Iron requirements roughly double during pregnancy. The American Society of Hematology and current obstetric guidelines now recommend universal screening for iron deficiency in pregnancy. When oral iron is failing or time is limited, guidelines support earlier use of IV iron in the second and third trimesters [8].
Infants and Children
Premature and low-birthweight infants are born with reduced iron stores and face the highest early risk. Toddlers who drink large volumes of cow's milk are also vulnerable. Cow's milk is low in bioavailable iron and can cause small amounts of blood loss in the gut, worsening iron balance [14].
Older Adults
In older adults, iron deficiency anemia should be treated as a potential sign of gastrointestinal blood loss until proven otherwise. The most common causes include slow bleeding from peptic ulcers, polyps, angiodysplasia, or colorectal cancer. Regular use of NSAIDs or aspirin, atrophic gastritis (thinning of the stomach lining), and Helicobacter pylori infection also contribute. In this age group, iron deficiency often coexists with anemia of inflammation, which can complicate diagnosis [3, 9].
People with Specific Medical Conditions
- Gastrointestinal diseases such as celiac disease, Crohn's disease, ulcerative colitis, H. pylori gastritis, and prior gastric bypass or bariatric surgery all reduce the gut's ability to absorb iron [9].
- Chronic kidney disease (CKD). Anemia in CKD results from a combination of reduced erythropoietin production, blood losses during dialysis, and high hepcidin from inflammation [16]. While historically managed with Erythropoiesis-Stimulating Agents (ESAs), the 2026 KDIGO guidelines recognize Hypoxia-Inducible Factor–Prolyl Hydroxylase Inhibitors (HIF-PHIs), such as vadadustat, as an alternative to ESAs [16,18]. These novel agents are particularly relevant for dialysis patients and alter how collateral iron supplementation is managed, though ESAs remain the preferred first-line therapy due to ongoing cardiovascular safety considerations [16].
- Heart failure. Iron deficiency, even without anemia, is now recognized as a treatable cardiovascular risk factor. IV iron has been shown to improve symptoms and exercise capacity in this group.
Diet and Lifestyle
Vegetarians and vegans need to consume roughly 1.8 times the iron of meat-eaters to absorb the same amount. Frequent blood donors, endurance athletes (who experience hepcidin rises from exercise-induced inflammation and some red cell damage in the feet), and people experiencing food insecurity are also at elevated risk [11]. All of these groups should be considered for routine iron deficiency anemia screening where possible.
How is Iron Deficiency Anemia Diagnosed?
Diagnosing iron deficiency anemia involves a complete blood count, iron studies, and once IDA is confirmed, targeted investigation for its underlying cause.
Complete Blood Count (CBC)
The CBC gives a broad picture of all blood cell types. In iron deficiency anemia, the typical findings are:
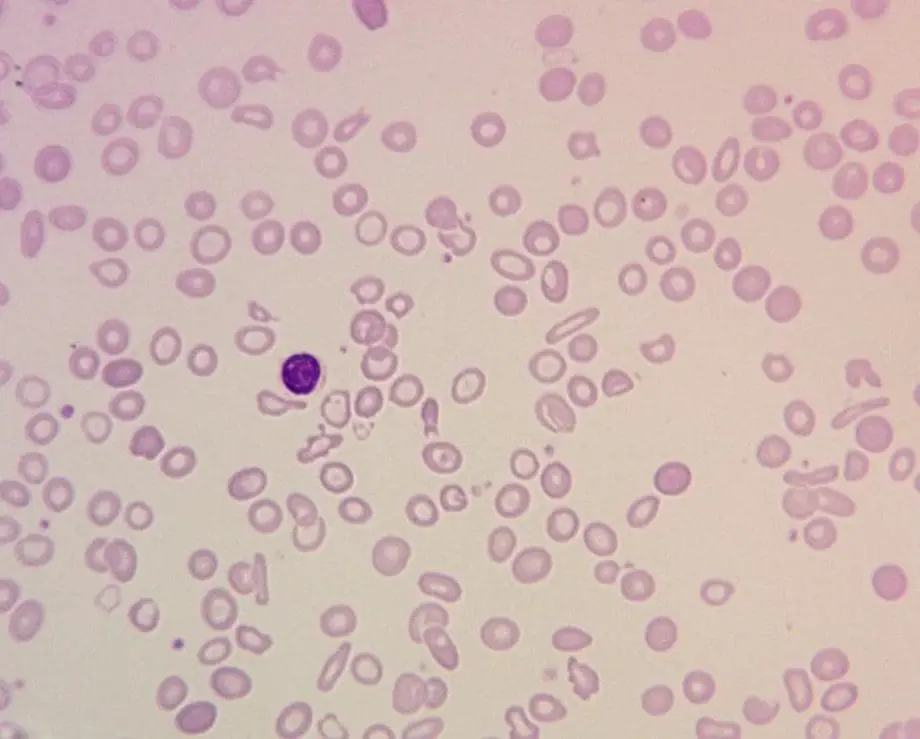
A peripheral blood film (a microscope slide of a blood sample) typically shows small, pale (microcytic, hypochromic) red blood cells of varying size and shape. Pencil-shaped red blood cells (pencil cells) are a characteristic finding.
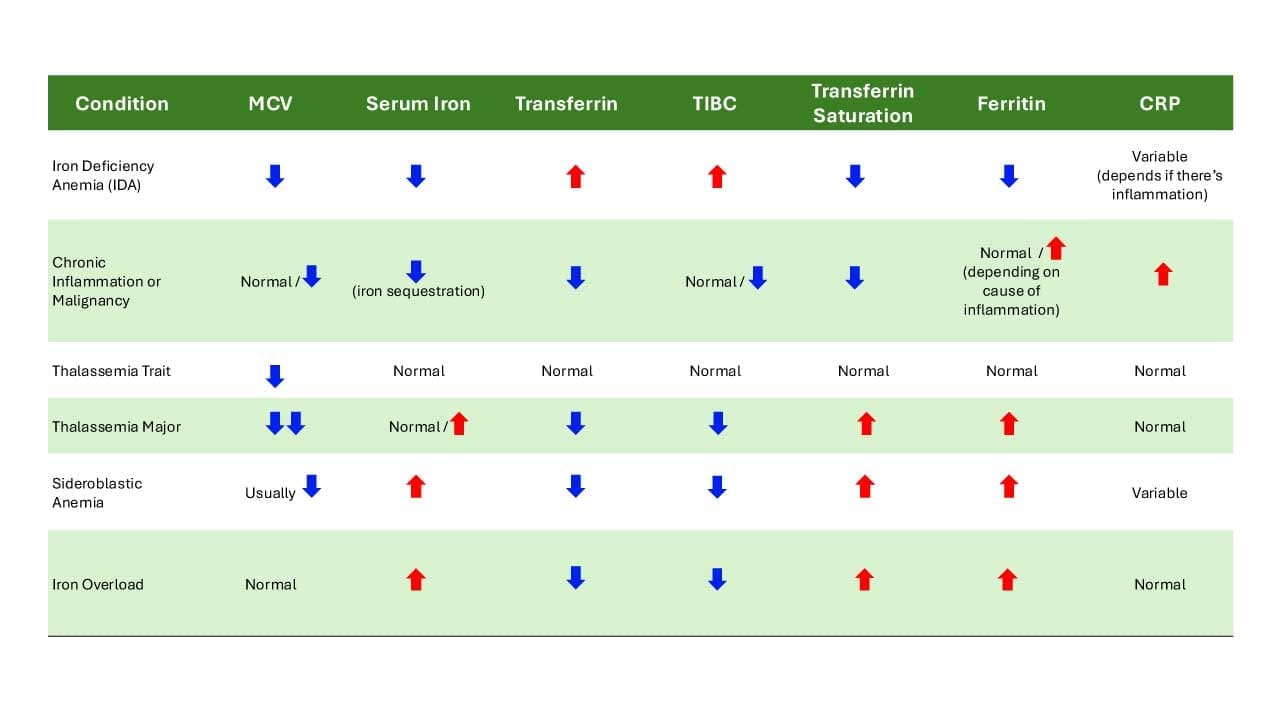
Iron Studies
Ferritin is what clinicians call an "acute phase reactant." This means it rises during infection, inflammation, liver disease, or cancer — even when iron stores are genuinely low. A ferritin level that looks normal may mask real iron deficiency. When inflammation is present, many guidelines accept ferritin up to 70–100 μg/L combined with a TSAT below 20% as consistent with iron deficiency.
Furthermore, modern nephrology guidelines, such as the 2026 Kidney Disease: Improving Global Outcomes (KDIGO) update, have shifted terminology from "functional iron deficiency" to "iron-restricted erythropoiesis" to more accurately reflect the pathophysiology of iron limitation during red blood cell production [16]. For patients with chronic kidney disease (CKD), particularly those on dialysis, diagnostic thresholds are significantly expanded. In these populations, guidelines advise withholding iron therapy only if ferritin exceeds 700 µg/L or TSAT is 40% or greater [16].
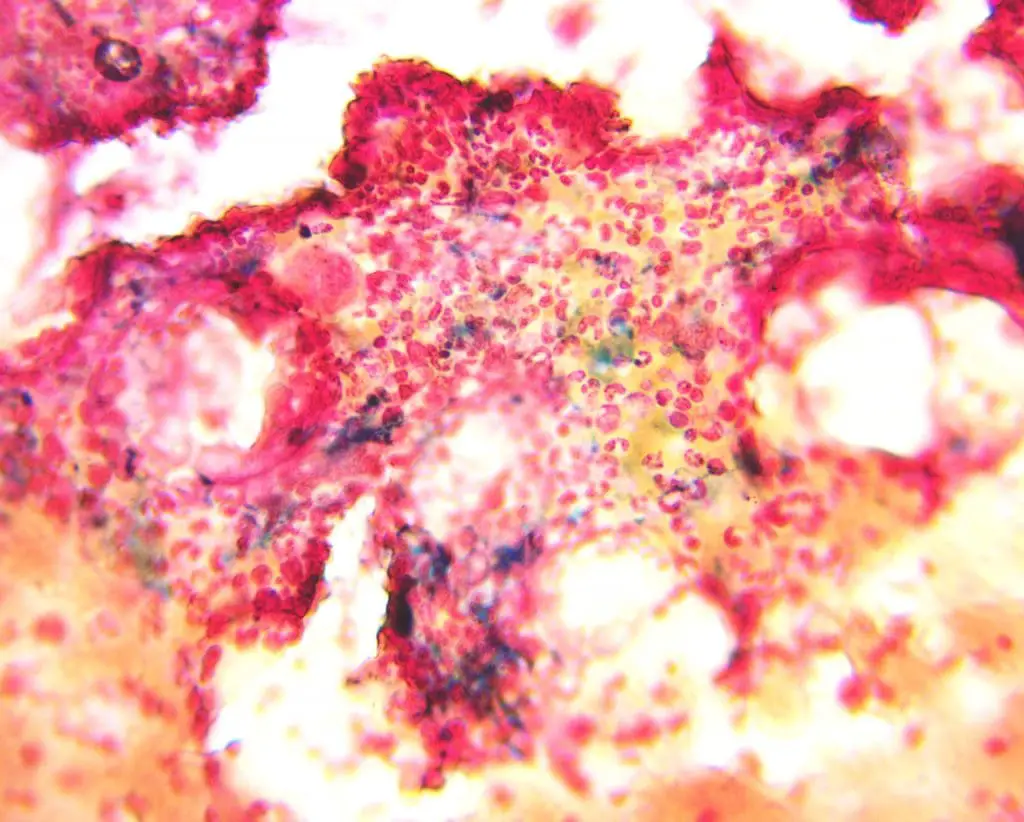
Bone Marrow Biopsy
A bone marrow aspirate stained with Perls' Prussian blue stain (which turns iron deposits blue) has historically been considered the gold standard test for iron deficiency. In iron deficiency anemia, iron stores are completely absent, and no blue color is seen. In modern practice, this test is rarely needed. Blood-based tests — ferritin, TSAT, and sTfR — are sufficient for the vast majority of cases [11].
Finding the Cause
Confirming the diagnosis is only the first step. The underlying cause must always be identified and addressed. The 2024 American Gastroenterological Association (AGA) Clinical Practice Update provides clear guidance [9]:
- Adult men and post-menopausal women should undergo bidirectional endoscopy (a gastroscopy to look at the upper gut and a colonoscopy for the lower gut) in essentially all cases. Testing for celiac disease and H. pylori infection is also recommended. If both scopes are negative, capsule endoscopy can examine the small bowel.
- Pre-menopausal women need a thorough menstrual and pregnancy history. GI evaluation is warranted if the menstrual history is insufficient or if symptoms suggest GI disease [9].
- Children require a dietary history (with particular attention to excess cow's milk intake), growth assessment, and celiac disease evaluation where appropriate [14].
Iron Deficiency Anemia Treatment & Management
Effective treatment of iron deficiency anemia has three equally important components: replace the iron, treat the underlying cause, and monitor the response. Treating the anemia without addressing the cause is never enough as the deficiency will return.
Oral Iron: The First-Line Treatment
For most non-pregnant adults with iron deficiency anemia, oral iron supplements are the first treatment choice. They are effective, inexpensive, and widely available.
Current evidence has reshaped the standard recommendation. The older approach of taking iron every day is now known to work less well than taking it every other day.
- Dose: A single morning dose of 60 to 120 mg of elemental iron. As a guide: one tablet of ferrous sulfate 200 mg contains approximately 60 mg of elemental iron; one tablet of ferrous fumarate 200 mg also provides around 60 mg; ferrous gluconate 325 mg provides approximately 65 mg.
- Frequency: Alternate-day dosing is heavily recommended for tolerability, though daily dosing remains acceptable [17]. While early stable isotope studies suggested alternate-day dosing produces more total absorbed iron by allowing hepcidin to reset [4,5,6], recent reviews clarify that both regimens significantly improve hemoglobin [17]. Alternate-day administration is an excellent strategy to minimize gastrointestinal side effects and improve adherence if daily oral iron is poorly tolerated, but daily single dosing achieves comparable clinical and hematologic outcomes in many patients [17].
- With vitamin C: Taking the supplement with orange juice or another vitamin C source improves absorption. Separate it from coffee, tea, dairy, calcium supplements, and antacids by at least one hour.
- Duration: Continue until hemoglobin returns to normal, then keep going for a further three months to fully refill iron stores. The target is a ferritin above 50 to 100 μg/L, depending on the clinical context.
Common side effects include nausea, stomach pain, constipation, and dark stools. Dark stools are harmless and expected. Most intolerance resolves by switching to alternate-day dosing, choosing a different formulation, or taking the supplement with a small amount of food.
Intravenous Iron: When Oral Iron Is Not Enough
IV iron delivers iron directly into the bloodstream, bypassing the gut entirely. It is the preferred choice when:
- Oral iron is not tolerated or has not worked
- Absorption is impaired (for example, in celiac disease, inflammatory bowel disease, or after bariatric surgery)
- Rapid replacement is needed (late pregnancy, before major surgery, or during significant ongoing blood loss)
- The patient has chronic kidney disease on dialysis. For hemodialysis patients, the 2026 KDIGO guidelines strongly endorse a proactive, high-dose IV iron strategy over a reactive, low-dose approach [16,18]. Based on evidence from the PIVOTAL trial, administering maintenance IV iron proactively reduces the need for erythropoiesis-stimulating agents (ESAs) without increasing the risk of infection [18].
- The patient has heart failure with iron deficiency [7,9]
Modern IV iron preparations carry a very low risk of serious allergic reactions. All IV iron infusions should be given in a clinical setting equipped to recognize and manage infusion reactions if they occur.
Blood Transfusion
Blood transfusion is reserved for patients with severe symptomatic anemia, hemodynamic instability, or active uncontrolled bleeding. It is a short-term stabilizing measure. It does not treat the iron deficiency itself, and IV iron should follow once the patient is stable.
Monitoring the Response
Regular follow-up is essential when treating iron deficiency anemia. The goal is to confirm that hemoglobin is rising and that iron stores are being rebuilt:
- At 4 weeks: Check hemoglobin. A rise of 10 g/L or more indicates a good response to treatment.
- At 3 months: Check ferritin and TSAT to confirm stores have been refilled.
- If there is no response: Consider three possibilities — ongoing blood loss, a malabsorption problem, or poor adherence to the supplement regimen. Each requires a different approach.
Iron in Food: Diet and Iron Deficiency Anemia
Diet plays a supporting role in both preventing and managing iron deficiency anemia. Knowing which foods are richest in iron and which foods interfere with absorption is practical knowledge for all.
Heme Iron Sources (Best Absorbed)
These are animal-derived and absorbed most efficiently by the body:
- Liver and organ meats (beef liver is particularly rich)
- Shellfish: clams, oysters, mussels
- Red meat: beef, lamb
- Poultry: especially dark meat
- Oily fish: sardines, tuna
Non-Heme Iron Sources
These are plant-derived and less efficiently absorbed, but they make a meaningful contribution when consumed regularly and paired with vitamin C:
- Iron-fortified breakfast cereals
- Lentils, chickpeas, kidney beans, soybeans
- Tofu and tempeh
- Pumpkin seeds and sesame seeds (tahini)
- Dark leafy greens: spinach, Swiss chard, kale
- Dried fruits: apricots, raisins
Because non-heme iron absorption is lower, vegetarians and vegans are advised to consume roughly 1.8 times the recommended daily iron intake compared with meat-eaters.
Foods and Drinks That Help Absorption
Vitamin C, eaten alongside iron-rich foods or supplements, significantly boosts non-heme iron absorption. Good sources include citrus fruits, bell peppers, tomatoes, and strawberries.
Foods and Drinks That Reduce Absorption
The following reduce iron absorption when consumed at the same time as iron-rich foods or supplements. Separating them by about an hour is enough to minimize the effect:
- Coffee and tea (which contain tannins that bind iron)
- Milk and dairy products
- Calcium-fortified foods and antacids
Frequently Asked Questions (FAQs)
What is the main cause of iron deficiency anemia (IDA)?
The answer depends on age and sex. In pre-menopausal women, heavy menstrual bleeding is the leading cause. In men and post-menopausal women, chronic gastrointestinal blood loss must be assumed until ruled out — common sources include peptic ulcers, polyps, and colorectal cancer. In infants and toddlers, inadequate dietary iron and excess cow's milk are the main contributors. In parts of the world where parasitic infection is common, hookworm is a significant cause [9,11].
What are the 4 common symptoms of iron deficiency anemia?
Fatigue, pallor (pale skin), shortness of breath on exertion, and dizziness or light-headedness are the most frequently reported symptoms. Restless legs, hair shedding, brittle nails, and pica are also characteristic but occur less often.
How long does treatment take to work?
Hemoglobin usually begins rising within two to four weeks of effective oral iron therapy and returns to normal by six to eight weeks. Refilling iron stores takes a further three months or so. With IV iron, hemoglobin typically rises within a few weeks and stores can be replaced in one or two infusions, depending on the preparation used.
When is the best time to take iron supplements?
A single morning dose on an empty stomach gives the best absorption. Taking iron every other day produces higher total absorption and fewer side effects compared to daily [4,5,6]. Pair it with orange juice or another source of vitamin C, and keep it away from coffee, tea, dairy, calcium supplements, and antacids for at least one hour.
Can you have iron deficiency without anemia, and does it matter?
Yes, and it does matter. Iron stores can become depleted before hemoglobin falls below the normal range. In this state, called iron deficiency without anemia (IDWA), fatigue, hair shedding, restless legs, and reduced exercise tolerance can all occur — and all respond to iron replacement [1,7]. A ferritin below 30 μg/L in an adult (or below 20 μg/L in a child) supports the diagnosis even when hemoglobin looks normal.
Are there test kits available to test for iron deficiency at home?
Yes, there are at-home iron test kits available. Most at-home kits measure ferritin from a finger-prick blood sample and can be a useful first screen. However, they should not replace a clinician-ordered iron panel if symptoms persist or results are abnormal. Ferritin can be misleadingly raised by inflammation, making the result harder to interpret without additional tests like TSAT.
Glossary of Related Medical Terms
- Anemia — Hemoglobin below the normal range for age and sex.
- Anisopoikilocytosis — Variation in red blood cell size and shape, seen on a blood smear.
- Bioavailability — The proportion of a nutrient that the body actually absorbs and uses.
- Ferritin — The main iron-storage protein in the body; a serum ferritin blood test reflects total iron stores.
- Ferroportin — The only protein that exports iron out of cells into the bloodstream; controlled by hepcidin.
- Hepcidin — A liver hormone that regulates iron absorption and release by causing ferroportin to break down.
- Heme iron — Iron found in animal foods, bound within the heme molecule; absorbed efficiently.
- Non-heme iron — Iron found in plant foods, eggs, and dairy; absorbed less efficiently.
- Hemoglobin (Hb) — The iron-containing protein in red blood cells that binds and transports oxygen.
- MCV (mean corpuscular volume) — The average size of a red blood cell. Low in iron deficiency anemia (microcytic).
- MCH (mean corpuscular hemoglobin) — The average amount of hemoglobin in a single red blood cell. Low in iron deficiency anemia (hypochromic).
- Microcytic / hypochromic — Red blood cells that are smaller and paler than normal.
- Reticulocyte — A young red blood cell freshly released from the bone marrow.
- Ret-He / CHr (reticulocyte hemoglobin content) — Reflects how much hemoglobin is in newly made red blood cells; an early sign of iron-restricted production.
- TIBC (total iron-binding capacity) — An indirect measure of how much transferrin is available to carry iron; rises when iron is low.
- TSAT (transferrin saturation) — The percentage of transferrin that is actually bound to iron; falls below 20% in iron deficiency.
- sTfR (soluble transferrin receptor) — Rises when cells need more iron; useful when ferritin is unreliable due to inflammation.
- Koilonychia — Spoon-shaped, brittle nails seen in chronic iron deficiency anemia.
- Glossitis — An inflamed, sore, smooth tongue.
- Angular cheilitis — Painful cracks at the corners of the mouth.
- Pica — A craving for non-food substances such as ice, clay, or paper.
- Plummer-Vinson syndrome — A rare combination of chronic iron deficiency anemia, difficulty swallowing, and an esophageal web.
- IDWA (iron deficiency without anemia) — Low iron stores with a still-normal hemoglobin level.
- Anemia of inflammation (anemia of chronic disease) — Anemia caused by high hepcidin trapping iron inside cells; can coexist with true iron deficiency anemia.
- Erythropoiesis — The process of producing red blood cells in the bone marrow.
- Perls' Prussian blue stain — A bone marrow stain that turns iron deposits blue; the stain is absent in iron deficiency anemia.
- Ferric carboxymaltose /ferric derisomaltose /ferumoxytol / iron sucrose — Modern intravenous iron preparations used when oral iron is unsuitable.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cancado, R. D., Leite, L. A. C., & Muñoz, M. (2025). Defining Global Thresholds for Serum Ferritin: A Challenging Mission in Establishing the Iron Deficiency Diagnosis in This Era of Striving for Health Equity. Diagnostics (Basel, Switzerland), 15(3), 289. https://doi.org/10.3390/diagnostics15030289
- Sholzberg, M., Hillis, C., Crowther, M., & Selby, R. (2025). Diagnosis and management of iron deficiency in females. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 197(24), E680–E687. https://doi.org/10.1503/cmaj.240570
- American Society of Hematology. (2025). ASH draft guideline: Diagnosis of iron deficiency. https://www.hematology.org/-/media/hematology/files/education/clinicians/guideline
s-quality/ida-dx-public-comment.pdf - Stoffel, N. U., Cercamondi, C. I., Brittenham, G., Zeder, C., Geurts-Moespot, A. J., Swinkels, D. W., Moretti, D., & Zimmermann, M. B. (2017). Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials. The Lancet. Haematology, 4(11), e524–e533. https://doi.org/10.1016/S2352-3026(17)30182-5
- Stoffel, N. U., Zeder, C., Brittenham, G. M., Moretti, D., & Zimmermann, M. B. (2020). Iron absorption from supplements is greater with alternate day than with consecutive day dosing in iron-deficient anemic women. Haematologica, 105(5), 1232–1239. https://doi.org/10.3324/haematol.2019.220830
- von Siebenthal, H. K., Gessler, S., Vallelian, F., Steinwendner, J., Kuenzi, U. M., Moretti, D., Zimmermann, M. B., & Stoffel, N. U. (2023). Alternate day versus consecutive day oral iron supplementation in iron-depleted women: a randomized double-blind placebo-controlled study. EClinicalMedicine, 65, 102286. https://doi.org/10.1016/j.eclinm.2023.102286
- Cappellini, M. D., Musallam, K. M., & Taher, A. T. (2020). Iron deficiency anaemia revisited. Journal of internal medicine, 287(2), 153–170. https://doi.org/10.1111/joim.13004
- Lewkowitz, A. K., & Tuuli, M. G. (2023). Identifying and treating iron deficiency anemia in pregnancy. Hematology. American Society of Hematology. Education Program, 2023(1), 223–228. https://doi.org/10.1182/hematology.2023000474
- DeLoughery, T. G., Jackson, C. S., Ko, C. W., & Rockey, D. C. (2024). AGA Clinical Practice Update on Management of Iron Deficiency Anemia: Expert Review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association, 22(8), 1575–1583. https://doi.org/10.1016/j.cgh.2024.03.046
- Camaschella C. (2019). Iron deficiency. Blood, 133(1), 30–39. https://doi.org/10.1182/blood-2018-05-815944
- Pasricha, S. R., Tye-Din, J., Muckenthaler, M. U., & Swinkels, D. W. (2021). Iron deficiency. Lancet (London, England), 397(10270), 233–248. https://doi.org/10.1016/S0140-6736(20)32594-0
- Auerbach, M., & Adamson, J. W. (2016). How we diagnose and treat iron deficiency anemia. American journal of hematology, 91(1), 31–38. https://doi.org/10.1002/ajh.24201
- Ganz T. (2013). Systemic iron homeostasis. Physiological reviews, 93(4), 1721–1741. https://doi.org/10.1152/physrev.00008.2013
- Leung, A. K. C., Lam, J. M., Wong, A. H. C., Hon, K. L., & Li, X. (2024). Iron Deficiency Anemia: An Updated Review. Current pediatric reviews, 20(3), 339–356. https://doi.org/10.2174/1573396320666230727102042
- Wolf, M., Rubin, J., Achebe, M., Econs, M. J., Peacock, M., Imel, E. A., Thomsen, L. L., Carpenter, T. O., Weber, T., Brandenburg, V., & Zoller, H. (2020). Effects of Iron Isomaltoside vs Ferric Carboxymaltose on Hypophosphatemia in Iron-Deficiency Anemia: Two Randomized Clinical Trials. JAMA, 323(5), 432–443. https://doi.org/10.1001/jama.2019.22450
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. (2026). KDIGO 2026 Clinical Practice Guideline for the Management of Anemia in Chronic Kidney Disease. Kidney International, 109(1), S1-S99.
- Kamath, S., Parveen, R. S., Hegde, S., Mathias, E. G., Nayak, V., & Boloor, A. (2024). Daily versus alternate day oral iron therapy in iron deficiency anemia: a systematic review. Naunyn-Schmiedeberg's archives of pharmacology, 397(5), 2701–2714. https://doi.org/10.1007/s00210-023-02817-7
- Lucia Del Vecchio, Aleix Cases, Michele F Eisenga, Jolanta Małyszko, Jonathan Barratt, Davide Bolignano, KDIGO 2026 Clinical Practice Guideline for Anemia in Chronic Kidney Disease (CKD): a commentary from the European Renal Best Practice (ERBP), Nephrology Dialysis Transplantation, 2026; gfag014, https://doi.org/10.1093/ndt/gfag014


