Key Takeaways
Iron studies interpretation uses serum iron, ferritin, transferrin or TIBC, and transferrin saturation together to map the body's iron status — never read one number alone [1,2].
- Ferritin below 30 µg/L strongly suggests iron deficiency in a healthy adult; below 15 µg/L confirms it [1,3].
- Inflammation can mask iron deficiency by inflating ferritin. In a general inflammatory illness, the WHO recommends a higher cut-off of 70 µg/L [9]. In heart failure and chronic kidney disease specifically, guidelines raise this further: ferritin under 100 µg/L, or 100–299 µg/L with TSAT under 20%, still counts as iron deficient [16,17].
- Soluble transferrin receptor (sTfR) rises with true tissue iron starvation and stays normal in pure inflammation, making it a reliable tie-breaker when ferritin is ambiguous [8].
- TSAT below 20% is the universal signal that the bone marrow is not getting enough iron, regardless of whether the cause is true deficiency or inflammation [1,6].
- Treatment depends on the cause: oral iron for simple deficiency, intravenous iron when the gut is bypassed or unreliable, phlebotomy for genetic overload, and chelation for transfusional overload.
*Click ▾ for more information
Introduction
Few blood tests are ordered more often than the iron panel, and few are misread more often. Think of an iron profile as a functional map of the body's iron logistics network rather than a list of disconnected numbers. Serum iron is the cargo moving right now. Transferrin and TIBC are the delivery fleet. Ferritin is the warehouse. A problem with any one part of this system, including something unrelated to iron itself, such as inflammation, can throw off the whole picture [2].
This guide walks through iron studies interpretation the way an experienced clinician does it: starting with what each marker means, then layering on the patterns that separate true iron deficiency from its look-alikes, especially anemia of chronic disease.

Why one number is rarely enough
Because systemic conditions like inflammation can distort single test results, clinicians must learn to read these markers as an interconnected pattern, not isolated values [1,2]. Serum iron fluctuates throughout the day, ferritin rises during infection, and transferrin falls when the liver redirects its resources toward inflammation. The whole panel, read in clinical context, is what gives the answer.
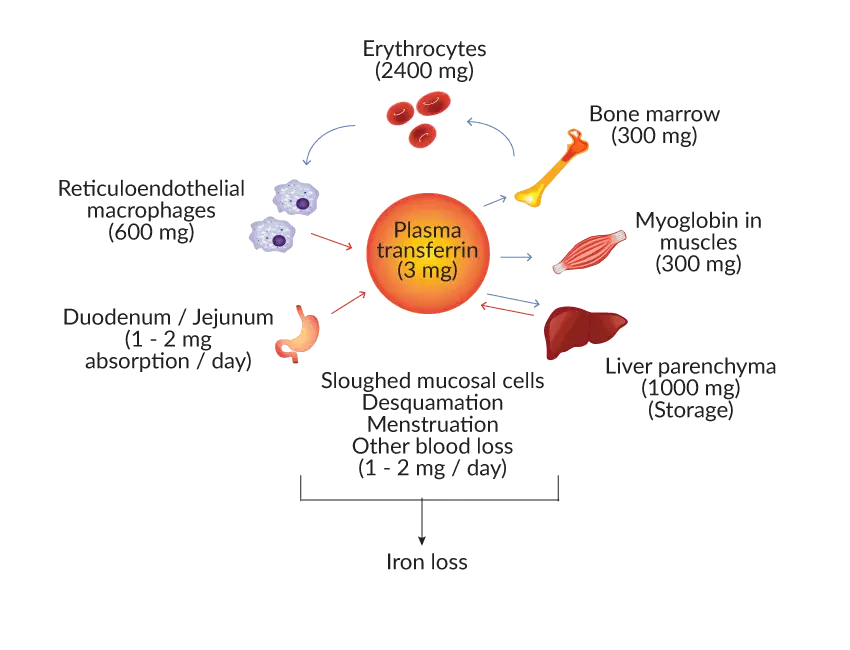
Iron Cycle and Metabolism in the Body
Iron enters the body through the gut, gets carried in blood bound to transferrin (the iron transport protein), and is either used in the bone marrow to make hemoglobin or stored as ferritin in the liver, spleen, and macrophages. When old red blood cells break down after their 120-day lifespan, macrophages recycle their iron back into circulation.
A liver hormone called hepcidin is the master switch. During inflammation, the liver releases hepcidin in response to inflammatory signals such as interleukin-6. Hepcidin acts like a padlock: it binds to ferroportin, the only doorway iron can use to leave a cell, and triggers its destruction. With the doorway gone, iron stays trapped inside macrophages and liver cells, and serum iron falls. This is a major part of why people with chronic inflammatory disease become anemic even when their iron stores are full [5,7].
Transferrin behaves differently. It is a negative acute-phase reactant, made by the liver. During chronic inflammation or malnutrition, the liver scales back transferrin gene transcription to redirect resources toward inflammatory proteins instead. This is an upstream production shutdown, not a cell-level defense response, and it explains why transferrin and TIBC drop in chronic illness even though iron transport would otherwise be needed [2,7].
Reference Ranges vs. Diagnostic Cut-offs
Two ideas are easy to confuse and worth separating early:
- Reference range = the spread of values found in a healthy population. Useful for flagging "abnormal."
- Diagnostic threshold = the value at which evidence supports a clinical decision, such as starting iron treatment.
These are not the same. A ferritin of 20 µg/L might fall inside the lab's "normal" range for a woman, yet fall below the diagnostic cut-off for iron deficiency [1,3]. Always check both, and never rule out iron deficiency in an inflammatory state just because ferritin isn't low [8,11].
The Five Core Markers
1. Ferritin — The Warehouse Reading
Ferritin is a protein that stores iron inside cells. Blood levels of ferritin mirror, indirectly, how much iron the body has in reserve. It is the single best test for iron stores [1,2].
Reference range (lab-derived):
- Men: 30–300 µg/L
- Women: 15–300 µg/L
Practical diagnostic cut-offs in a healthy adult:
- <15 µg/L: absolute iron deficiency [1]
- <30 µg/L: sensitive marker of iron deficiency, also used in pregnancy and pre-op screening [1,6]
With concurrent inflammation (such as rheumatoid arthritis, infection, or chronic kidney disease), ferritin no longer reflects stores reliably, because it is an acute-phase reactant:
- General inflammatory illness: the WHO recommends raising the diagnostic cut-off to ferritin <70 µg/L [9].
- Heart failure or chronic kidney disease specifically: established cardiology and nephrology guidelines define iron deficiency as ferritin <100 µg/L (absolute), or ferritin 100–299 µg/L combined with TSAT <20% (functional) [11,12]. This means a ferritin reading that looks comfortably "normal" can still represent clinically meaningful iron deficiency in these patients.
What else raises ferritin? Iron overload (hemochromatosis or repeated transfusions), liver disease, some cancers, autoimmune disease, and chronic alcohol use [1,2].
What lowers ferritin? Iron deficiency from any cause — poor intake, blood loss, malabsorption, or increased demand in pregnancy.
The big caveat
Ferritin is an acute-phase reactant. It rises during any inflammatory illness. A "normal" or even high ferritin in an inflamed patient does not rule out iron deficiency [1,7,8].
2. Serum Iron — The Cargo in Transit
Serum iron measures iron currently circulating in the blood, bound to transferrin. It is the most volatile number on the panel.
Reference range:
- Men: 60–170 µg/dL (11–32 µmol/L)
- Women: 40–150 µg/dL (7–27 µmol/L)
Serum iron looks straightforward but is the least reliable marker on its own. Levels can swing by up to 70% over the course of a single day [1]. To minimize the impact of this extreme diurnal variation and post-prandial spikes, blood for an iron panel should ideally be drawn in the morning after an overnight fast, avoiding any iron supplements for at least 24 hours prior [18]. Recent meals, iron tablets, blood loss, or any inflammatory illness can all move it sharply.
Hemolysis is another trap. If red blood cells rupture during a difficult blood draw, the iron stored inside them floods into the serum sample. This artificially spikes both serum iron and transferrin saturation and can ruin the accuracy of the whole panel. Labs should reject visibly hemolyzed samples for iron studies.
Because of this volatility, the 2021 British Society for Haematology Good Practice Paper goes as far as to say that measuring serum iron in isolation is not clinically useful on its own [1]. Its real value comes from feeding into the transferrin saturation calculation.
3. Transferrin — The Delivery Fleet
Transferrin is the main protein that ferries iron through the bloodstream. Each transferrin molecule can carry two iron atoms.
Reference range: 250–370 mg/dL (28–42 µmol/L)
High transferrin typically reflects iron deficiency. The body responds to empty stores by making more transferrin, hoping to grab any available iron. Pregnancy and oral contraceptive use also raise it.
Low transferrin points to either reduced production (inflammation, liver disease, malnutrition, nephrotic syndrome) or genuine iron overload, where the body needs less carrying capacity.
Transferrin is a negative acute-phase reactant, meaning inflammation drops it [2,7]. This matters because it can blunt the rise you would otherwise expect in iron deficiency complicated by chronic illness.
4. Total Iron-Binding Capacity (TIBC) — The Fleet's Total Capacity
TIBC reflects the maximum amount of iron the blood can carry if every transferrin binding site were occupied. In most modern labs, it tracks closely with transferrin and is often used interchangeably.
Reference range: 250–450 µg/dL (45–81 µmol/L)
High TIBC → usually iron deficiency (more empty seats on the bus).
Low TIBC → inflammation, liver disease, malnutrition, or iron overload.
TIBC's real job is feeding into the transferrin saturation.
5. Transferrin Saturation (TSAT) — Is the Fleet Actually Loaded?
TSAT = (serum iron ÷ TIBC) × 100. It tells you what percentage of the delivery fleet's capacity is currently in use.
Reference range: 20–50%
Diagnostic cut-off: TSAT below 20% is now widely recognized as the primary indicator of a restricted iron supply to the bone marrow, regardless of whether the underlying cause is true deficiency or chronic inflammation [1,6,11]. This is one of the most clinically reliable single thresholds on the entire panel.
- Low TSAT → iron deficiency anemia, anemia of chronic disease, IRIDA (iron-refractory iron deficiency anemia).
- High TSAT (>45% in women, >50% in men, persistently) → suspect hemochromatosis or other iron overload [4].
Absolute vs. Functional Iron Deficiency
This distinction is one of the most important concepts in iron studies interpretation, and it is easy to miss if you only look at reference ranges.
| Diagnostic Type | Ferritin | TSAT | Clinical Meaning |
|---|---|---|---|
| Absolute Deficiency | Low (<30 µg/L) | Low (<20%) | Total body iron stores are genuinely empty. |
| Functional Deficiency | Normal or high (often >100 µg/L in HF/CKD) | Low (<20%) | Iron is present but trapped by inflammation; the marrow can't access it fast enough. |
| Iron Overload | High (>200–300 µg/L) | High (>45–50%) | The system is overflowing with iron. |
In absolute iron deficiency, the warehouse is empty. In functional iron deficiency, the warehouse still has iron, but the hepcidin padlock is stuck, and the bone marrow cannot draw on it fast enough to keep up with red cell production [18]. This concept, formalized in the BSH's dedicated functional iron deficiency guideline, was originally developed for patients on erythropoiesis-stimulating agents in chronic kidney disease and has since become central to heart failure and CKD anemia management [18].
Reading the Panel Together: Classic Patterns
This is where iron studies interpretation gets clinically useful.
| Pattern | Serum Iron | Ferritin | Transferrin / TIBC | TSAT |
|---|---|---|---|---|
| Iron deficiency anemia | Low | Low | High | Low (<20%) |
| Anemia of chronic disease | Low | Normal or High | Low | Low or Normal |
| Iron deficiency + chronic disease | Low | Variable (often "normal") | Variable | Low |
| Iron overload (hemochromatosis) | High | High | Low | High (>45–50%) |
| Sideroblastic anemia | High | High | Low/Normal | High |
The trickiest scenario in clinical practice is the third row: someone with both iron deficiency and an inflammatory illness. Ferritin can look reassuring even when stores are gone [7,8].
Adjunct Tests When the Panel Is Ambiguous
When ferritin sits in the "grey zone" of roughly 30–100 µg/L and inflammation is present, the standard panel often cannot give a clean answer. Several additional tests can help [1,8].
Soluble Transferrin Receptor (sTfR)
sTfR is a fragment of the cellular receptor that takes up iron.Unlike ferritin, it is completely unaffected by inflammation, because it rises only in response to true tissue iron starvation. That makes it valuable when ferritin is unreliable [8].
sTfR/log ferritin index
A high sTfR paired with a high sTfR/log ferritin index points strongly toward true iron deficiency hidden beneath chronic inflammation. When the panel is ambiguous, ordering this combination can bypass the inflammatory noise and evaluate the bone marrow's actual functional iron status [8].
Reticulocyte Hemoglobin Content (Ret-He or CHr)
This modern complete blood count metric measures the hemoglobin inside newly made red cells (reticulocytes). Because reticulocytes only live one to two days, CHr reflects whether the bone marrow has enough iron available right now, not days or weeks ago. It is unaffected by inflammation, making it a fast, practical tool for detecting functional iron deficiency [1].
CRP (C-Reactive Protein)
Not an iron test itself, but ordering it alongside iron studies is now standard, since it tells you whether inflammation might be distorting ferritin and transferrin readings [1,8].
Hepcidin
The master regulator hormone. Routine clinical assays are not yet standardized, so hepcidin remains mostly a research tool. Still, understanding its behavior explains why someone with anemia of chronic disease can have low serum iron despite plentiful stores [5,7].
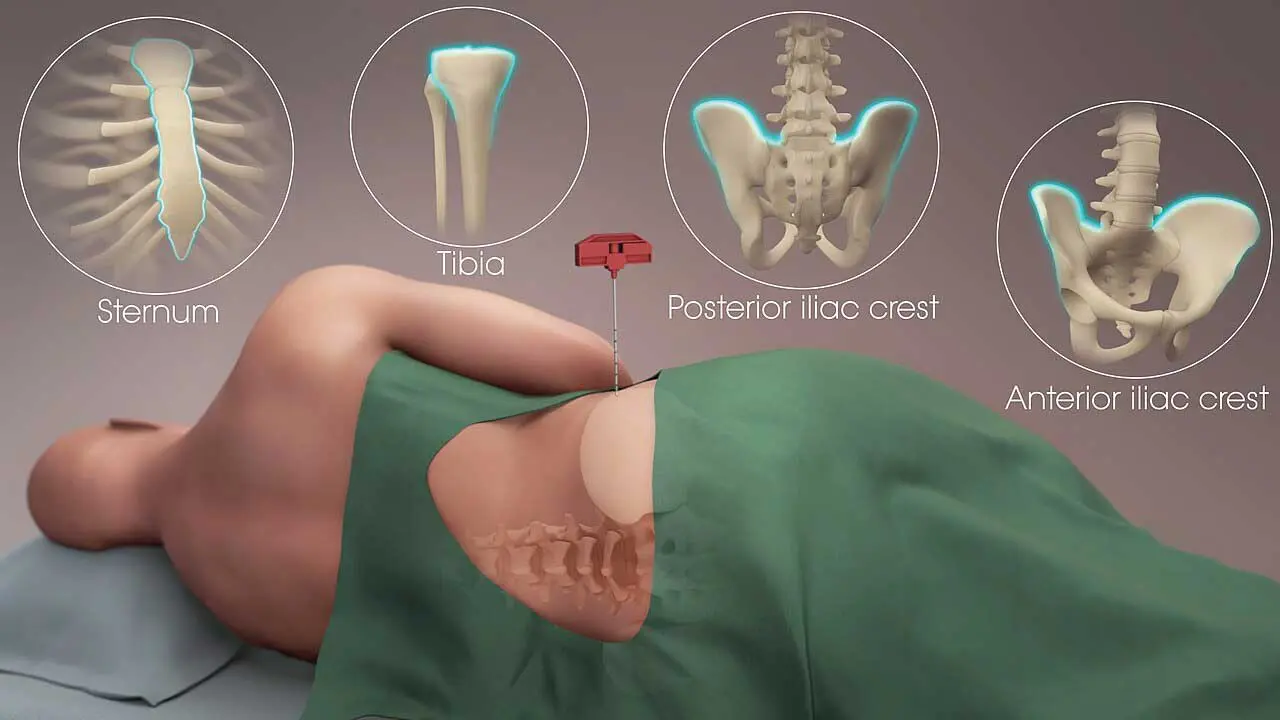
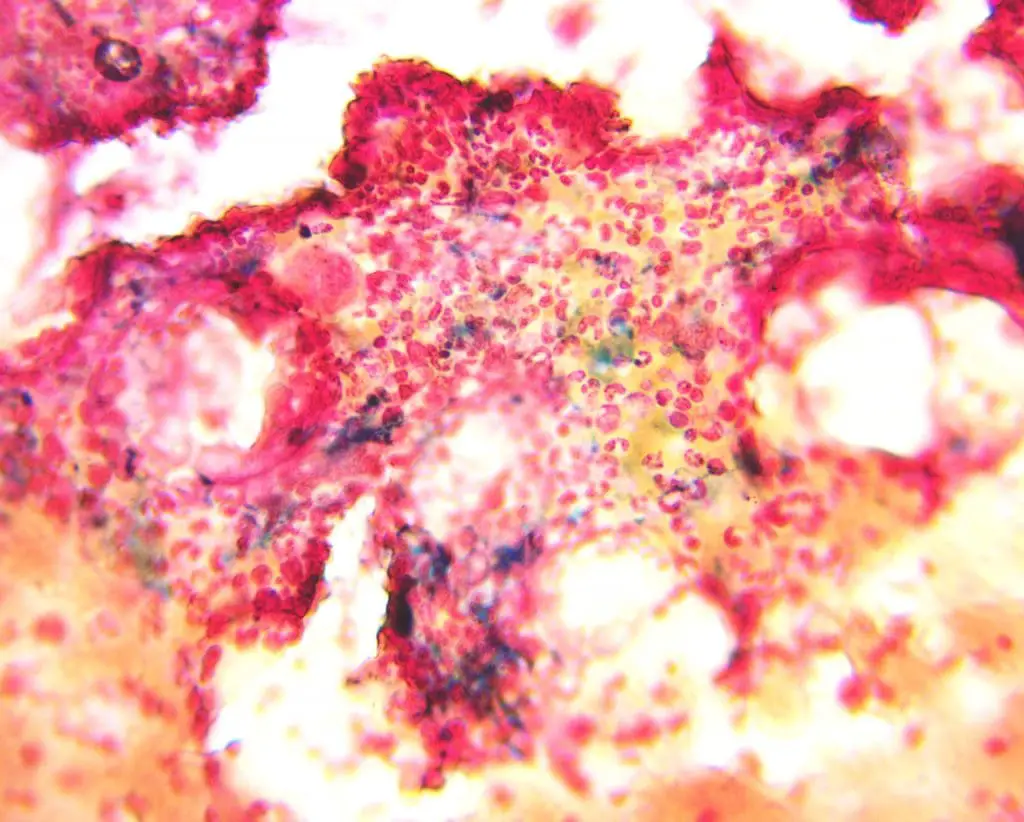
Bone Marrow Iron Staining: Still the "Gold Standard"?
A bone marrow aspirate stained with Perls' Prussian Blue directly shows stored iron. Historically this was the reference standard for assessing body iron [2].t is limited by its invasive nature, cost, and need for specialist expertise, so in modern practice it is rarely needed. Most cases are clear from blood tests, CRP, and clinical context. Bone marrow examination is now reserved for complicated cases, especially suspected sideroblastic anemia, myelodysplastic syndromes, or when blood tests give contradictory results in a critically ill patient.
Other Helpful Numbers
Mean Corpuscular Volume (MCV)
Average red blood cell size, reported on every full blood count. MCV <80 fL (microcytosis) is the classic clue for iron deficiency anemia, but thalassemia and anemia of chronic disease can also produce small cells [2]. A normal MCV does not rule out iron deficiency, especially early on.
Red Cell Distribution Width (RDW)
Often raised in iron deficiency anemia before MCV drops, because new small cells mix with older normal-sized ones. A high RDW alongside low ferritin is a strong combination [2].
From Lab Result to Treatment
Lab interpretation matters because it drives the next decision. In otherwise healthy adults with iron deficiency, oral iron is first-line. Modern guidelines increasingly recommend alternate-day (every other day) dosing for oral iron rather than daily administration. Oral iron temporarily spikes hepcidin for up to 48 hours, blocking subsequent absorption; alternate-day dosing maximizes fractional absorption and significantly reduces gastrointestinal side effects [14,15].
Ferritin and hemoglobin usually start to rise within weeks, but full stores take roughly three months to rebuild [3]. Intravenous iron formulations such as ferric carboxymaltose and ferric derisomaltose are now widely used when oral iron is poorly tolerated, ineffective, or too slow — for example before surgery, in pregnancy, in inflammatory bowel disease, and in chronic kidney disease [3,6,10]. Iron overload is managed with phlebotomy or chelation depending on the cause.
The lab is the starting point, not the destination.
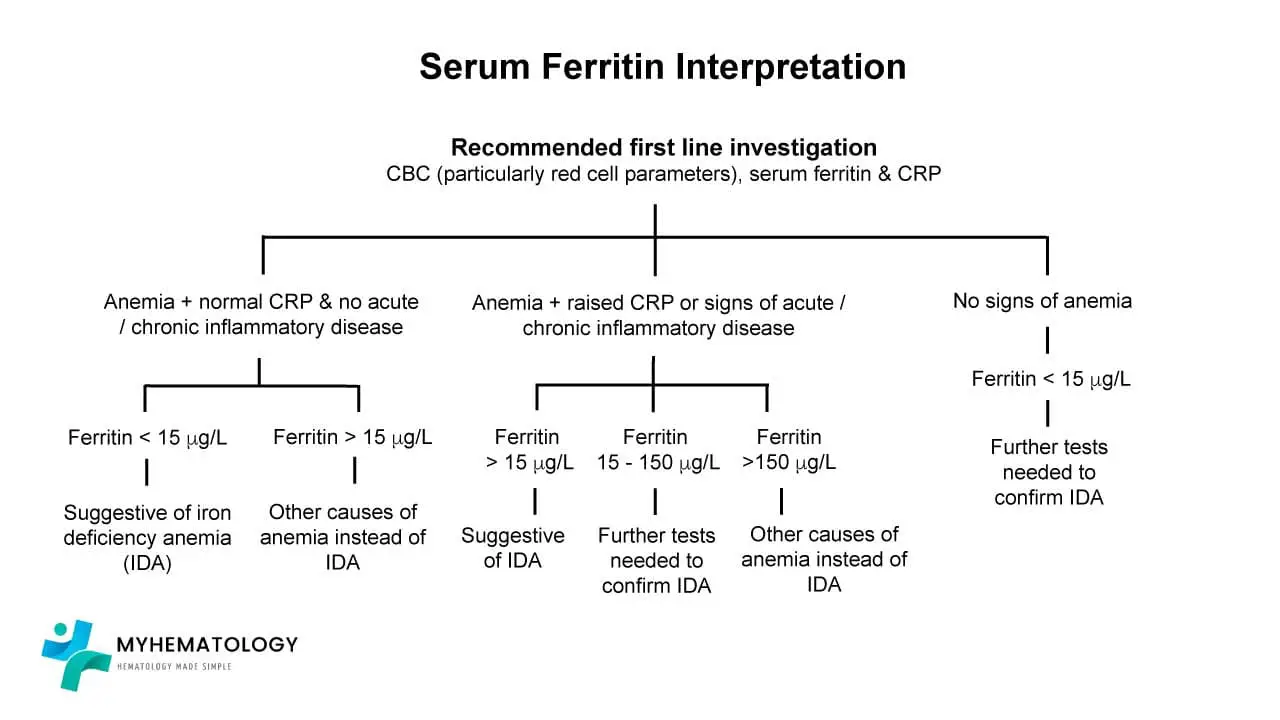
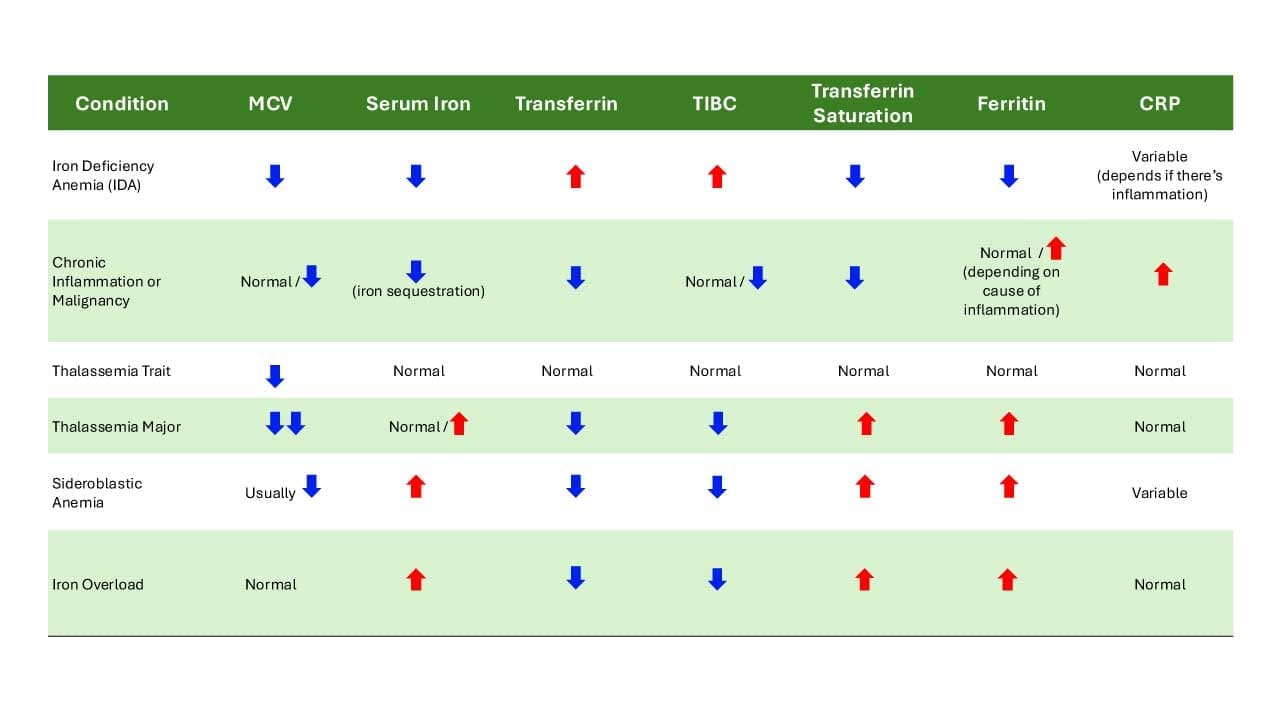
Iron Studies Interpretation Chart
Iron studies interpretation assess various markers to evaluate iron status and diagnose potential iron-related conditions.
Frequently Asked Questions (FAQs)
What do iron studies actually measure?
Iron studies are a panel of blood tests that look at iron status from several angles at once. The core tests are serum iron (iron circulating in the blood right now), ferritin (iron stored in tissues), transferrin or TIBC (the body's iron-carrying capacity), and transferrin saturation (the percentage of that capacity currently in use). Looking at all four together is what makes accurate iron studies interpretation possible. Any single test on its own can mislead.
What ferritin level confirms iron deficiency?
In otherwise healthy adults, a ferritin below 30 micrograms per liter is widely accepted as a sensitive marker of iron deficiency, and below 15 confirms absolute deficiency. In people with inflammation or chronic disease, ferritin can be falsely high. The WHO recommends using a ferritin threshold of 70 micrograms per liter in that setting. In pregnancy, ferritin below 30 is the usual cut-off.
Why is my ferritin normal but I still have iron deficiency symptoms?
Ferritin behaves as an acute-phase reactant. That means inflammation, infection, liver disease, or recent illness can push it up even when iron stores are low. This is why doctors often check CRP at the same time, or order tests like transferrin saturation, soluble transferrin receptor, or reticulocyte hemoglobin to look past the inflammation. A pattern of normal-to-high ferritin with low transferrin saturation and high CRP is a classic clue for functional iron deficiency.
Do I need to fast before an iron panel?
Usually not. Most labs do not require fasting. However, serum iron levels swing throughout the day and rise after iron-containing meals or supplements, so many clinicians prefer a morning sample taken before breakfast and before that day's iron tablet. Always follow your own lab's instructions.
What is the difference between iron deficiency and iron deficiency anemia?
Iron deficiency means iron stores are depleted. Iron deficiency anemia is the later stage, when stores are gone, hemoglobin starts to fall, and the body cannot make enough healthy red blood cells. Iron deficiency without anemia is common and still causes real symptoms like fatigue, hair loss, and exercise intolerance.
How long does it take iron levels to recover with treatment?
Symptoms often improve within a few weeks of starting iron therapy, but rebuilding ferritin stores typically takes about three months with oral iron. Intravenous iron works faster and is now standard when oral iron is poorly tolerated, ineffective, or when stores need to be replenished quickly, such as before surgery or in advanced chronic kidney disease. Follow-up blood tests guide when to stop or continue treatment.
Glossary of Related Medical Terms
- Anemia of chronic disease (ACD) — Anemia caused by ongoing inflammation or chronic illness, where iron is present in the body but trapped in storage and not available to make red blood cells. Also called anemia of inflammation.
- Erythropoiesis — The production of new red blood cells, mainly in the bone marrow.
- Ferritin — A protein that stores iron inside cells. Blood levels of ferritin reflect how much iron the body has in reserve.
- Functional iron deficiency — A state where total body iron is normal or high, but the iron cannot be released fast enough to keep up with red blood cell production. Common in chronic inflammation.
- Hemochromatosis — A condition, usually genetic, where the body absorbs and stores too much iron, eventually damaging the liver, heart, and other organs.
- Hepcidin — A liver hormone that controls how much iron is absorbed from food and released from storage. Inflammation raises hepcidin; iron deficiency lowers it.
- Iron studies (iron panel) — A group of blood tests typically including serum iron, ferritin, transferrin or TIBC, and transferrin saturation, used together to assess iron status.
- Microcytic anemia — Anemia in which red blood cells are smaller than normal (low MCV). Iron deficiency is the most common cause.
- Reticulocyte hemoglobin content (Ret-He or CHr) — The average amount of hemoglobin in newly made red blood cells. Drops early in iron deficiency, before ferritin or MCV change.
- Soluble transferrin receptor (sTfR) — A blood marker that rises when cells are starved for iron. Useful because it is not raised by inflammation.
- Transferrin — The main blood protein that carries iron to tissues.
- Transferrin saturation (TSAT) — The percentage of transferrin currently carrying iron. Low in iron deficiency, high in iron overload.
- TIBC (Total Iron-Binding Capacity) — A measure of how much iron transferrin in the blood could carry if all binding sites were full.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Fletcher, A., Forbes, A., Svenson, N., Wayne Thomas, D., & A British Society for Haematology Good Practice Paper (2022). Guideline for the laboratory diagnosis of iron deficiency in adults (excluding pregnancy) and children. British journal of haematology, 196(3), 523–529. https://doi.org/10.1111/bjh.17900
- Kelly, A. U., McSorley, S. T., Patel, P., & Talwar, D. (2017). Interpreting iron studies. BMJ (Clinical research ed.), 357, j2513. https://doi.org/10.1136/bmj.j2513
- Snook, J., Bhala, N., Beales, I. L. P., Cannings, D., Kightley, C., Logan, R. P., Pritchard, D. M., Sidhu, R., Surgenor, S., Thomas, W., Verma, A. M., & Goddard, A. F. (2021). British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut, 70(11), 2030–2051. https://doi.org/10.1136/gutjnl-2021-325210
- Pasricha, S. R., Tye-Din, J., Muckenthaler, M. U., & Swinkels, D. W. (2021). Iron deficiency. Lancet (London, England), 397(10270), 233–248. https://doi.org/10.1016/S0140-6736(20)32594-0
- Camaschella C. (2019). Iron deficiency. Blood, 133(1), 30–39. https://doi.org/10.1182/blood-2018-05-815944
- Hands, K., Daru, J., Evans, C., Kotze, A., Lewis, C., Narayan, S., Richards, T., Taylor, C., Timmins, S., Wilson, A., & BSH Committee (2024). Identification and management of preoperative anaemia in adults: A British Society for Haematology Guideline update. British journal of haematology, 205(1), 88–99. https://doi.org/10.1111/bjh.19440
- Ganz T. (2019). Anemia of Inflammation. The New England journal of medicine, 381(12), 1148–1157. https://doi.org/10.1056/NEJMra1804281
- Fertrin K. Y. (2020). Diagnosis and management of iron deficiency in chronic inflammatory conditions (CIC): is too little iron making your patient sick?. Hematology. American Society of Hematology. Education Program, 2020(1), 478–486. https://doi.org/10.1182/hematology.2020000132
- WHO guideline on use of ferritin concentrations to assess iron status in individuals and populations [Internet]. Geneva: World Health Organization; 2020. EXECUTIVE SUMMARY. Available from: https://www.ncbi.nlm.nih.gov/books/NBK569877/
- Auerbach, M., & Adamson, J. W. (2016). How we diagnose and treat iron deficiency anemia. American journal of hematology, 91(1), 31–38. https://doi.org/10.1002/ajh.24201
- McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., Burri, H., Butler, J., Čelutkienė, J., Chioncel, O., Cleland, J. G. F., Coats, A. J. S., Crespo-Leiro, M. G., Farmakis, D., Gilard, M., Heymans, S., Hoes, A. W., Jaarsma, T., Jankowska, E. A., Lainscak, M., … ESC Scientific Document Group (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European heart journal, 42(36), 3599–3726. https://doi.org/10.1093/eurheartj/ehab368
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. (2026). KDIGO 2026 Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney International.
- Mayo Clinic Laboratories. (2024). Test Definition: IRON (Serum). Mayo Foundation for Medical Education and Research.
- Moretti, D., Goede, J. S., Zeder, C., Jiskra, M., Chatzinakou, V., Tjalsma, H., Melse-Boonstra, A., Brittenham, G., Swinkels, D. W., & Zimmermann, M. B. (2015). Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood, 126(17), 1981–1989. https://doi.org/10.1182/blood-2015-05-642223
- Ko, C. W., Siddique, S. M., Patel, A., Harris, A., Sultan, S., Altayar, O., & Falck-Ytter, Y. (2020). AGA Clinical Practice Guidelines on the Gastrointestinal Evaluation of Iron Deficiency Anemia. Gastroenterology, 159(3), 1085–1094. https://doi.org/10.1053/j.gastro.2020.06.046
- Doehner, W., Anker, S. D., et al. (2018). Iron deficiency in heart failure: An overview. JACC: Heart Failure, 6(11), 909–916. https://doi.org/10.1016/j.jchf.2018.07.015
- McDonagh, T. A., Metra, M., Adamo, M., et al.; ESC Scientific Document Group. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 42(36), 3599–3726. https://doi.org/10.1093/eurheartj/ehab368
- Thomas, D. W., Hinchliffe, R. F., Briggs, C., Macdougall, I. C., Littlewood, T., & Cavill, I.; British Committee for Standards in Haematology. (2013). Guideline for the laboratory diagnosis of functional iron deficiency. British Journal of Haematology, 161(5), 639–648. https://doi.org/10.1111/bjh.12311