Procedure-at-a-Glance
A hemolysate is the liquid produced when red blood cells are deliberately broken open so that hemoglobin can be tested. It is the starting material for hemoglobin electrophoresis, HPLC, capillary electrophoresis, and the alkaline denaturation test [1,2].
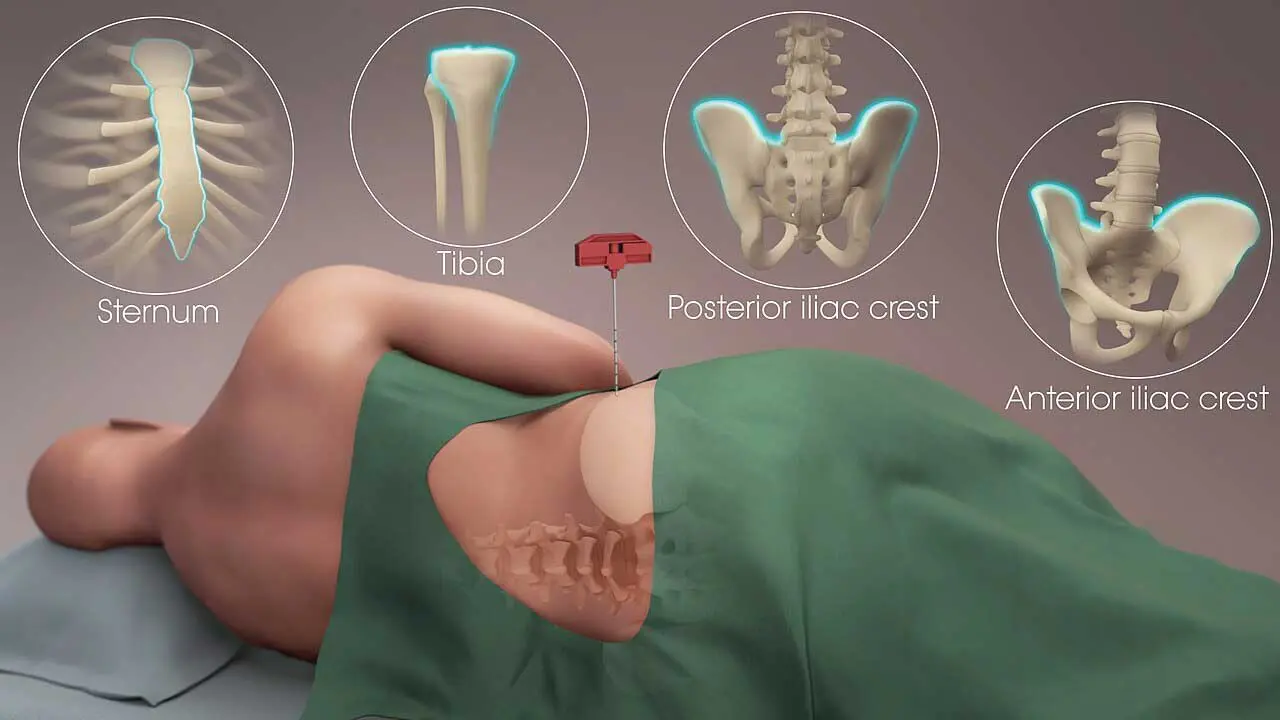
- Collection. Collect 3mL EDTA blood.
- Separation. Centrifuge at ~1000 × g for 5 min; remove plasma.
- Washing. Wash packed red cells 3× with 0.85 % saline.
- Lysis. Add hypotonic water or detergent (e.g., Triton X-100).
- Extraction (optional). Add organic solvent in a fume hood.
- Purification. Centrifuge at ~1000 × g for 15 min; filter.
- Storage. 4 °C for short-term, –70 °C or lower for long-term.
Why Hemolysate Preparation Matters
Hemoglobinopathies and thalassemias are among the most common single-gene disorders worldwide, and most laboratory tests that diagnose them depend on a clean preparation of hemoglobin. Plasma proteins and red cell membranes both interfere with hemoglobin separation, so removing them up front protects the result downstream [1,2].
Screening for Hemoglobin Variants
Hemoglobin separation methods identify structural variants by their charge and migration behavior. A clean hemolysate is what allows these techniques to work clearly [3]:
- Hemoglobin S (HbS) is the variant in sickle cell disease. Early identification, especially in newborns, allows preventive measures against splenic sequestration and vaso-occlusive crises [7].
- Hemoglobin C (HbC) is most common in people of West African descent. On its own it causes mild hemolytic anemia; combined with HbS (HbSC disease) it produces a significant sickling disorder.
- Hemoglobin E (HbE) is widespread in Southeast Asia. The trait is often silent, but HbE/beta-thalassemia can cause severe anemia.
- Alpha-thalassemia and HbH disease appear as a fast-moving band (β4 tetramer) on alkaline electrophoresis and a characteristic peak on HPLC. They are frequent in Southeast Asian, Mediterranean, and Middle Eastern populations.
Diagnosing Thalassemias
Thalassemias are disorders of quantity, not structure — one globin chain is produced in reduced amounts. Hemolysate analysis quantifies the minor hemoglobins:
- HbA2 is normally 2.3–3.4 % of total hemoglobin in adults. Levels above 3.5 % are the classic marker of beta-thalassemia trait, the cut-off recommended by the International Council for Standardization in Haematology (ICSH) [2,4].
- HbF sits below about 1.8 % in adults [4]. Persistently high HbF can indicate delta-beta thalassemia or hereditary persistence of fetal hemoglobin (HPFH).
Alkaline Denaturation and Fetal Hemoglobin
The alkaline denaturation test (Singer / Betke method) takes advantage of one fact: HbF resists denaturation in alkali, while HbA does not. Apply alkali to a hemolysate, and the hemoglobin still in solution at the end of the reaction is essentially HbF.
That makes the test useful in two distinct settings, which the literature sometimes blurs:
- HbF quantitation in a hemolysate as part of thalassemia and HPFH workup.
- Fetomaternal hemorrhage (FMH) evaluation. Here, however, the Kleihauer-Betke acid-elution test and flow cytometry with an anti-HbF antibody are now the more common methods. Flow cytometry is the most sensitive and reproducible option and has become standard where it is available [6].
Monitoring Sickle Cell Treatment
For sickle cell disease, hydroxyurea raises HbF and reduces sickling, and serial hemoglobin analysis tracks that rise. Following the global market withdrawals of crizanlizumab (Adakveo) and voxelotor (Oxbryta) in 2023 and 2024 due to clinical efficacy and safety concerns respectively, disease modification relies heavily on hydroxyurea, L-glutamine, and newer definitive interventions [8,9]. These include the FDA-approved gene therapies exa-cel (Casgevy) and lovo-cel (Lyfgenia)—both of which depend on accurate HbF and HbS quantitation run on HPLC or capillary electrophoresis platforms that begin with a hemolysate.
Principle of Hemolysate Preparation
The goal is straightforward: rupture the red cell membrane without damaging the hemoglobin inside.
Two methods do this. Hypotonic lysis uses distilled water where water moves into the cell down its osmotic gradient until the membrane bursts. Detergent lysis uses a non-ionic surfactant such as Triton X-100, which dissolves the lipid bilayer directly. Both release hemoglobin into solution along with membrane fragments (stroma) and any leftover plasma proteins.
The next steps strip out those contaminants. Centrifugation pulls the heavy stroma down. Optional extraction with an organic solvent (toluene or chloroform) precipitates lipids and any remaining membrane material. Filtration removes fine debris. What remains is a clear, red, concentrated hemoglobin solution.
For most downstream tests the working concentration is approximately 10 g/dL of hemoglobin. Too dilute and the bands or peaks are weak; too concentrated and they smear or co-elute.
Materials
- Fresh EDTA whole blood (3 mL)
- 0.85 % saline
- Distilled or deionized water
- Whatman No. 1 filter paper
- 5 mL glass tubes
- Pipettes and micropipettes
- Vortex mixer
- Refrigerated centrifuge (ideal)
- Lysis reagent — Triton X-100 (non-ionic detergent) or distilled water (hypotonic)
- Fine Pasteur pipette
- Optional: toluene or chloroform for solvent extraction
Safety note
Toluene and chloroform are volatile and require fume-hood handling and appropriate PPE. Carbon tetrachloride (CCl₄) appears in older protocols but is hepatotoxic and a probable human carcinogen; most modern laboratories no longer use it. Substitute toluene or chloroform, or skip the solvent step where the application allows.
Protocol
- Collect 3 mL of fresh blood into an EDTA tube. Inspect for micro-clots.
- Transfer the blood to a glass tube and centrifuge at ~1000 × g for 5 minutes (approximately 3000 rpm in a typical clinical bench centrifuge. Please confirm with your rotor specifications).
- Carefully aspirate the plasma layer without disturbing the red cells.
- Wash the red cells three times with 0.85 % saline. Resuspend gently after each wash, centrifuge as in step 2, and discard the supernatant. The supernatant of the third wash should be clear and colorless. This is the quality cue that washing is complete.
- Note the volume of packed red cells after the final wash.
- Lyse the cells using one of the following:
- Hypotonic lysis: add 0.75 volumes of distilled water relative to packed cells.
- Detergent lysis: add the manufacturer-recommended volume of Triton X-100 working solution.
- Vortex for 2–3 minutes.
- Optional solvent step (hypotonic lysis only): in a fume hood, add 0.5 volumes of toluene or chloroform relative to packed cells. Vortex vigorously for 2–3 minutes.
- Centrifuge at ~1000 × g for 15 minutes, ideally at 4 °C to limit hemoglobin oxidation.
- With a fine Pasteur pipette, collect the clear hemolysate. With hypotonic lysis alone, the hemolysate sits below the dark stromal plug. With solvent extraction, it sits above the solvent layer.
- Wet a piece of Whatman No. 1 filter paper with distilled water (so it does not soak up your sample) and filter the hemolysate.
- Adjust the hemoglobin concentration as required for your downstream assay (typically ~10 g/dL for gel electrophoresis; follow the manufacturer for HPLC or capillary electrophoresis).
- Store at 4 °C for use within ~24 hours, or aliquot and freeze at –70 °C or below for long-term storage. Thaw frozen aliquots on ice before use [1].
Quality Indicators

Before running the hemolysate on any platform, check three things:
- Color and clarity. A bright cherry-red, transparent solution suggests good lysis and minimal oxidation. Dark brown indicates methemoglobin formation; turbidity indicates lipid or membrane carryover.
- Hemoglobin concentration. Measure by spectrophotometry (cyanmethemoglobin method) or read directly from your automated analyzer. Adjust to the assay-appropriate target.
- Run a control hemolysate of known composition (HbA/F/S/C) alongside patient samples each batch.
Three methods are commonly used to measure hemoglobin in the hemolysate:
Common Challenges
Even a standardized protocol can yield poor results if variables aren't tightly controlled. Below are the most common issues encountered during hemolysate preparation and how to resolve them.
Where Manual Hemolysate Preparation Fits Today
Most routine hemoglobinopathy laboratories now use automated HPLC or capillary electrophoresis systems that lyse red cells inside the analyzer using a built-in dilution-and-lysis reagent. For a typical newborn or adult screening run, a manual hemolysate is not required [3].
Manual preparation still earns its place in several situations:
- Samples with very low hemoglobin where the analyzer's onboard lysis is not enough.
- Suspected unstable hemoglobins, where solvent extraction can help isolate the protein for further study.
- Research applications, including isoelectric focusing and protein chemistry studies.
- Troubleshooting ambiguous analyzer results, where a clean offline preparation can resolve interferences.
- Resource-limited settings where gel electrophoresis remains the primary method.
Reference Ranges (Adults)
| Hemoglobin | Typical Reference Range | Note |
|---|---|---|
| HbA | 95–98 % | Bulk adult hemoglobin (α₂β₂) |
| HbA2 | 2.3–3.4 % | >3.5 % suggests β-thalassemia trait [2, 4] |
| HbF | 0.0–1.8 % | Persistently elevated → δβ-thalassemia or HPFH [4] |
Frequently Asked Questions (FAQs)
What is a hemolysate, and why do laboratories prepare one?
A hemolysate is the liquid produced when red blood cells are deliberately broken open to release hemoglobin. Laboratories prepare it because clean, isolated hemoglobin is the starting material for tests that diagnose hemoglobin disorders such as sickle cell disease and thalassemia. Removing plasma proteins and red cell membranes first prevents background interference on hemoglobin electrophoresis, HPLC, and capillary electrophoresis.
Is hemolysate preparation still done by hand in modern laboratories?
Most routine hemoglobinopathy testing today is performed on automated HPLC or capillary electrophoresis analyzers that lyse the red cells inside the instrument. Manual hemolysate preparation is still used for atypical samples for example very low hemoglobin, suspected unstable hemoglobin variants, research, and troubleshooting unclear analyzer results.
Why is EDTA preferred over heparin or citrate?
EDTA preserves red cell morphology and hemoglobin integrity well for several days at 4 °C and does not interfere with most electrophoresis buffers. Heparin can be used in a pinch, but it can carry over into capillary electrophoresis runs and cause artifacts. Citrate dilutes the sample and can shift electrophoretic mobility, so it is avoided.
Why must red cells be washed three times before lysis?
Each wash removes more plasma protein. Plasma carries albumin and globulins that, if left behind, produce extra bands or peaks that can be mistaken for abnormal hemoglobins. By the third wash, the supernatant should be clear and colorless — that is the visual cue that washing is sufficient.
What does an "elevated HbA2" mean on a hemolysate report?
HbA2 is normally about 2.3–3.4 % of total hemoglobin in adults. When HbA2 rises above 3.5 %, the most common explanation is beta-thalassemia trait. Iron deficiency anemia can falsely lower HbA2, so iron studies should be checked alongside the hemoglobin analysis.
Has flow cytometry replaced the alkaline denaturation test for fetomaternal hemorrhage?
For quantifying fetomaternal hemorrhage, flow cytometry with an anti-HbF antibody is more sensitive and reproducible than the alkaline denaturation test or the manual Kleihauer-Betke smear, and many transfusion-medicine services have moved to it where available. The alkaline denaturation method is still used in some settings to quantify HbF in a hemolysate as part of thalassemia and HPFH workup, which is a different clinical question.
Glossary of Related Medical Terms
- Alkaline denaturation test (Singer / Betke): A laboratory test that estimates fetal hemoglobin by exposing a hemolysate to alkali. HbA breaks down quickly; HbF resists, so the leftover color tells you how much HbF is present.
- Capillary electrophoresis (CE): An automated technique that separates hemoglobin types inside a thin, electrically charged capillary tube. Common first-line method for hemoglobinopathy screening.
- Cyanmethemoglobin method: A spectrophotometric technique that converts hemoglobin to a stable colored form to measure its concentration accurately.
- EDTA (ethylenediaminetetraacetic acid): An anticoagulant that binds calcium and prevents clotting. The standard tube for hemoglobin studies.
- Fetomaternal hemorrhage (FMH): Passage of fetal red cells into the mother's circulation, which can cause Rh sensitization in Rh-negative mothers.
- Hemoglobinopathy: A genetic disorder caused by a structural change in a globin chain (e.g., sickle cell disease).
- Hb electrophoresis: A method that separates hemoglobin types based on how they move in an electric field.
- Hemolysate: The fluid that remains after red blood cells have been deliberately broken open. It contains hemoglobin and is the starting material for hemoglobin testing.
- HPLC (high-performance liquid chromatography): An automated technique that separates hemoglobin variants on a column. Quantifies HbA, HbA2, HbF, and most variants in a single run.
- HPFH (hereditary persistence of fetal hemoglobin): A benign condition where HbF stays high into adulthood.
- Hypotonic lysis: Bursting cells by placing them in a solution with less solute than the cell interior, drawing water in until the membrane ruptures.
- Isoelectric focusing (IEF): A high-resolution gel method that separates hemoglobins by their isoelectric point.
- Kleihauer-Betke (KB) test: A microscopic acid-elution test that counts fetal red cells in a maternal blood smear. Used for FMH quantitation.
- Methemoglobin: Oxidized hemoglobin (iron in the Fe³⁺ state) that cannot carry oxygen. Gives a brown discoloration.
- Packed red blood cells (pRBCs): Red cells separated from plasma by centrifugation.
- Stroma: The empty membrane "ghosts" left after red cells are lysed and hemoglobin is released.
- Thalassemia: A genetic disorder where one of the globin chains is produced in reduced amounts.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Bain BJ, Bates I, Laffan MA. Dacie and Lewis Practical Haematology: Expert Consult: Online and Print (Elsevier) 12th Edition. 2016.
- Stephens, A. D., Colah, R., Fucharoen, S., Hoyer, J., Keren, D., McFarlane, A., Perrett, D., Wild, B. J., & International Council for Standardization in Haematology (ICSH) (2015). ICSH recommendations for assessing automated high-performance liquid chromatography and capillary electrophoresis equipment for the quantitation of HbA2. International journal of laboratory hematology, 37(5), 577–582. https://doi.org/10.1111/ijlh.12413
- Frömmel C. (2018). Newborn Screening for Sickle Cell Disease and Other Hemoglobinopathies: A Short Review on Classical Laboratory Methods-Isoelectric Focusing, HPLC, and Capillary Electrophoresis. International journal of neonatal screening, 4(4), 39. https://doi.org/10.3390/ijns4040039
- Rodriguez-Capote, K., & Higgins, T. N. (2015). Incidence of hemoglobinopathies and thalassemias in Northern Alberta. Establishment of reference intervals for HbF and HbA2. Clinical biochemistry, 48(10-11), 698–702. https://doi.org/10.1016/j.clinbiochem.2015.04.001
- Kunarathnam V, Yarrarapu SNS, Mikes BA. Kleihauer-Betke Test. [Updated 2026 Mar 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430876/
- Peruzzi, B., Guerrieri, S., Biagioli, T., Lanzilao, L., Pratesi, S., Bencini, S., Statello, M., Carraresi, A., Stefanelli, S., Tonelli, M., Brogi, M., Capone, M., Mazzoni, A., Gelli, A. M. G., Fanelli, A., Caporale, R., & Annunziato, F. (2024). HPLC and flow cytometry combined approach for HbF analysis in fetomaternal haemorrhage evaluation. Practical laboratory medicine, 40, e00401. https://doi.org/10.1016/j.plabm.2024.e00401
- Ball, J., Bradley, A., Le, A., Tisdale, J. F., & Uchida, N. (2025). Current and future treatments for sickle cell disease: From hematopoietic stem cell transplantation to in vivo gene therapy. Molecular therapy : the journal of the American Society of Gene Therapy, 33(5), 2172–2191. https://doi.org/10.1016/j.ymthe.2025.03.016
- European Medicines Agency. (2023). Revocation of authorisation for sickle cell disease medicine Adakveo. EMA/359200/2023.
- Food and Drug Administration. (2024). FDA alerts health care professionals and patients of the voluntary withdrawal of Oxbryta (voxelotor) from the market due to safety concerns. FDA Drug Safety Communications.
- Oshiro, I., Takenaka, T., & Maeda, J. (1982). New method for hemoglobin determination by using sodium lauryl sulfate (SLS). Clinical biochemistry, 15(2), 83–88. https://doi.org/10.1016/s0009-9120(82)91069-4