Procedure-at-a-Glance
The leukocyte alkaline phosphatase (LAP) stain, also called the neutrophil alkaline phosphatase (NAP) stain, is a cytochemical test that measures the enzyme alkaline phosphatase inside mature neutrophils.
- Fix fresh smears in Cold Formalin-Methanol (0-10°C) for 30 seconds.
- Gently rinse with running tap water and air dry.
- Immerse dried slides in freshly prepared buffered substrate for 15 - 30 mins at room temperature.
- Wash thoroughly in running water.
- Apply counterstain for 3 mins.
- Rinse and air dry before microscopic examination.
A low LAP score classically suggests chronic myeloid leukemia (CML) or some myelodysplastic syndromes [1,5]. Historically, it was also associated with paroxysmal nocturnal hemoglobinuria (PNH), though flow cytometry is the modern diagnostic standard for PNH [9]. A high LAP score is typical of leukemoid reactions, polycythemia vera, primary myelofibrosis, pregnancy, and severe infection [1,4].
Introduction
The leukocyte alkaline phosphatase stain is one of those classic hematology tests. It is simple, inexpensive, and visually striking under the microscope. It was once the go-to lab tool for telling chronic myeloid leukemia apart from a leukemoid reaction. Today, molecular tests have taken over that job, but the LAP stain has not disappeared. It remains a teaching cornerstone and a practical fallback in many labs around the world [1].
This article walks through the principle, the protocol, and the clinical interpretation of the LAP score, with the modern diagnostic context kept in mind throughout.
Where the LAP Stain Fits Today
Current World Health Organization and International Consensus Classification frameworks (both updated in 2022) define CML by the presence of the BCR-ABL1 fusion gene, detected through quantitative RT-PCR or cytogenetic analysis [6,7]. Treatment response is also monitored by molecular methods, with European LeukemiaNet 2020 recommendations specifying BCR-ABL1 transcript milestones during tyrosine kinase inhibitor (TKI) therapy [8].
So where does the LAP stain still earn its place?
- As a rapid, low-cost adjunct when molecular testing is unavailable or delayed.
- As a teaching tool that links neutrophil maturation, enzyme biology, and clinical hematology in one slide.
- As a supportive marker in some myeloproliferative neoplasms and other non-CML conditions [3,4].
Knowing this context up front makes the rest of the article easier to interpret.
Differentiation of CML from Leukemoid Reaction
Both CML and a leukemoid reaction can push the white blood cell count well above normal. Both feature lots of neutrophils. To the naked eye on a slide, they can look surprisingly similar. The difference matters: one is a clonal cancer that needs lifelong TKI therapy, the other is a benign reaction to an infection or another stressor.
Several features help separate them, and the LAP score is one of the classic discriminators. The table below summarizes the main contrasts.
| Feature | Leukemoid Reaction | CML Neoplastic |
|---|---|---|
| Cause | Reactive (infection, inflammation) | Clonal myeloproliferative neoplasm |
| Onset | Acute | Insidious, chronic |
| Symptoms | Related to underlying cause | Fatigue, weight loss, night sweats, splenomegaly |
| WBC Count | Often <50,000/µL | Often >100,000/µL |
| Maturation | Mainly mature neutrophils, clear left shift | Full granulocyte spectrum (myelocyte bulge) |
| Blasts | Absent or <5% | <5% in chronic phase |
| Toxic Changes | Often present (Döhle bodies, vacuoles) | Usually absent |
| Basophilia / Eosinophilia | Generally absent or mild | Almost always present |
| LAP Score | Normal or elevated | Low or absent |
| Philadelphia Chromosome | Absent | Present in 90–95% of cases |
| BCR-ABL1 Fusion Gene | Absent | Present in virtually all cases |
| Splenomegaly | Absent or mild | Common, often marked |
Confirming CML
In a real workup, a low LAP score points toward CML, but the diagnosis is confirmed by detecting BCR-ABL1 [6,7].
Principle of LAP Stain
The stain is built on a simple chemistry trick. Mature neutrophils carry plenty of alkaline phosphatase (ALP) inside their cytoplasm. The test makes that enzyme reveal itself by leaving behind a colored deposit wherever it is active.
Here is what happens, step by step:
- A diazonium salt (a reactive coupling dye) is applied to the smear together with naphthol AS-BI phosphate, a substrate.
- ALP inside the neutrophil cytoplasm cleaves the phosphate from naphthol AS-BI phosphate, releasing free naphthol.
- The free naphthol couples with the diazonium salt to form an insoluble blue-violet or reddish-brown azo dye (the exact color depends on the salt used).
- The deposit shows up as granules in the cytoplasm under the microscope.
The more enzyme present, the heavier the staining. Mature, healthy neutrophils stain darkly; immature or abnormal neutrophils, like those in CML, stain weakly or not at all [1].

Materials
- Fresh, unstained peripheral blood smears (heparinized blood or fresh capillary smears)
- Known positive control smear (e.g., from a patient with a confirmed leukemoid reaction, or third-trimester pregnancy) and a known negative control smear (e.g., from a confirmed CML case)
- Freshly prepared fixative: 1 part 40% formaldehyde to 9 parts absolute methanol, kept ice-cold (0–10°C)
- Naphthol AS-BI phosphate
- 0.2 mol/L Tris buffer, pH 9.0
- Fast Blue BB salt (the coupling azo dye)
- Neutral red, 0.02% aqueous solution (counterstain)
- Filter paper and funnel
- Mounting medium (Depex) and coverslips
Safety Note
Formaldehyde, N,N-dimethylformamide (DMF), and diazonium salts are all hazardous. Work in a fume hood, wear gloves and eye protection, and dispose of waste according to local biohazard and chemical-safety rules.
Protocol
The full method is summarized at the start of the article. The detailed steps are:
- Prepare stock substrate solution. Dissolve 30 mg naphthol AS-BI phosphate in 0.5 mL N,N-dimethylformamide and add 100 mL 0.2 mol/L Tris buffer.
- Prepare working buffered substrate solution. Warm 40 mL of stock substrate solution to room temperature and add 24 mg of Fast Blue BB salt. Mix until fully dissolved. Filter through filter paper before use.
- Fix the smears. Place fresh smears in the chilled fixative for 30 seconds.
- Rinse with gently running tap water for 2–3 minutes. Air dry.
- Incubate the slides in working buffered substrate solution for 15–30 minutes at room temperature.
- Rinse with gently running tap water for 1–2 minutes.
- Air dry the slides.
- Counterstain in neutral red for 3 minutes.
- Rinse briefly and air dry.
- Mount with Depex and apply a coverslip.
- View under oil immersion (×100 objective).
Manufacturer kits may vary slightly. Always follow the kit insert when one is supplied.
Interpretation
The LAP score reflects how mature and how active a sample's neutrophils are. Stronger staining means more enzyme, which generally means more mature, healthy cells.
To produce a score:
- Count 100 consecutive mature neutrophils and band forms under oil immersion. Skip eosinophils and basophils — they do not carry the enzyme.
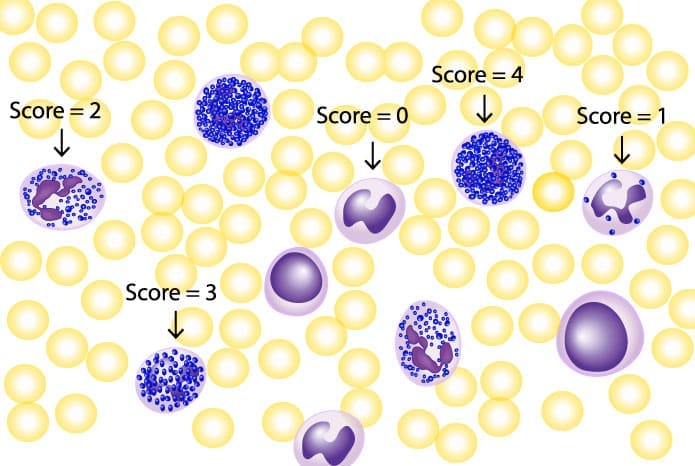
- Grade each cell on the 0–4 scale below.
- Add the grades together.
| Grade | Neutrophil Staining | Interpretation |
|---|---|---|
|
0
|
No stained granules | Negative |
|
1
|
Occasional stained granules | Weakly positive |
|
2
|
Moderate granules | Positive |
|
3
|
Numerous granules | Strongly positive |
|
4
|
Dense granules covering the nucleus | Heavily positive |
Because each of 100 cells can score 0 to 4, the total falls between 0 and 400. The normal adult range is 20–100 [1].
Worked example. Say 30 neutrophils score 0, 40 score 1, 20 score 2, and 10 score 3. The LAP score = (30×0) + (40×1) + (20×2) + (10×3) = 0 + 40 + 40 + 30 = 110. That sits just above the normal range, suggesting mild reactive elevation.
A score above 100 suggests a leukemoid reaction or another reactive cause. A score below 20 raises concern for CML, PNH, or another bone marrow disorder. As always, the LAP score is interpreted alongside the full clinical picture and other lab results [1].
Clinical Significance of a High LAP score (NAP score)
A high LAP score most often points to a benign, reactive process where mature neutrophils are produced in larger-than-usual numbers. Common causes include:
- Leukemoid reaction from severe infection (sepsis, pneumonia, abscess), inflammation (rheumatoid arthritis, vasculitis, inflammatory bowel disease), tissue necrosis (burns, myocardial infarction, pancreatitis), some solid tumors, or corticosteroid therapy [1].
- Myeloproliferative neoplasms other than CML. Polycythemia vera classically shows a high LAP score linked to the JAK2 V617F mutation [4]. Essential thrombocythemia tends to be normal to slightly raised. Primary myelofibrosis is variable, and some calreticulin (CALR)-mutated cases show notably low scores [3].
- Hodgkin lymphoma in some cases [1].
- Down syndrome, in whom the LAP score is naturally higher.
- Pregnancy and lactation because of hormonal changes.
- Post-splenectomy state.
- Severe physical or emotional stress, or major trauma
| Condition | Typical LAP Score | Genetic Hallmark | |
|---|---|---|---|
| CML | Very low to absent (0–15) | BCR-ABL1 (Ph+) | |
| Polycythemia Vera | High (>100) | JAK2 V617F | |
| Essential Thrombocythemia | Normal to slightly high | JAK2 CALR MPL | |
| Primary Myelofibrosis | Variable (normal to low) | JAK2 CALR MPL | |
| Leukemoid Reaction | High | None (reactive) |
Clinical Significance of a Low LAP score (NAP score)
A low LAP score is the more "exam-classic" finding because it points at a smaller, more specific list of diagnoses:
- Chronic myeloid leukemia. The textbook association. Neutrophils carrying the BCR-ABL1 fusion gene express far less alkaline phosphatase [1,7].
- Paroxysmal nocturnal hemoglobinuria (PNH). LAP is anchored to the cell surface by a GPI link, which is missing on PNH cells, so the score is low [1]. Today, high-sensitivity flow cytometry (utilizing FLAER, CD55, and CD59 markers) is the required gold standard for PNH diagnosis; the LAP score is no longer used clinically for this purpose [9].
- Aplastic anemia. Reduced and abnormal neutrophil production lowers the score.
- Pernicious anemia (severe vitamin B12 deficiency) can lower the score because of impaired neutrophil maturation.
- Some myelodysplastic syndromes, especially those with higher blast counts [5].
A note on CML follow-up
A classic low score in chronic-phase CML can rise during superimposed infection, after splenectomy, or in blast crisis. The score is dynamic, not fixed, which is one reason it has been replaced for monitoring by BCR-ABL1 transcript measurement [8].
Troubleshooting the LAP/NAP Stain
| Observation | Likely Cause | Corrective Action |
|---|---|---|
| All cells score 0 |
|
|
| Weak or faded staining |
|
|
| “Muddy” background |
|
|
| Poor neutrophil morphology |
|
|
| Non-specific lymphocyte staining |
|
|
| High RBC background |
|
|
Newer semi-automated NAP rating systems [2], as well as flow cytometric quantification of neutrophil alkaline phosphatase [10], are increasingly utilized to reduce the subjectivity and inter-observer variability of manual microscopic scoring.
Frequently Asked Questions (FAQs)
Why can't EDTA blood be used for the LAP stain?
EDTA chelates the specific divalent cations (namely zinc and magnesium) that alkaline phosphatase absolutely requires for its structural integrity and catalytic activity [11], inactivating the enzyme within minutes. The result is a falsely low score. Use heparinized blood or, ideally, fresh capillary blood smears made directly from a finger prick.
How is the leukocyte alkaline phosphatase score calculated?
Count 100 consecutive mature neutrophils and band forms under oil immersion. Grade each on a 0–4 scale based on staining intensity. Add the grades. The total falls between 0 and 400, with a normal adult range of about 20–100.
Is the LAP score still used to diagnose CML?
Not as a primary diagnostic tool. CML is confirmed by detecting BCR-ABL1 with quantitative RT-PCR or by finding the Philadelphia chromosome on cytogenetics [6,7]. The LAP stain is now an inexpensive adjunct and a teaching tool.
Can the LAP score change in the same CML patient over time?
Yes. A classically low LAP score in chronic-phase CML can climb toward normal during infection, after splenectomy, or in CML blast crisis. This is why LAP is interpreted alongside the rest of the clinical picture.
Why does pregnancy raise the LAP score?
LAP activity rises naturally during the second and third trimesters because of hormonal shifts, particularly higher estrogen and progesterone. The score returns to baseline after delivery.
What are the most common reasons for a false-low LAP score?
EDTA-anticoagulated blood, smears older than 24–48 hours, fixative warmer than 10°C, and unfiltered or expired diazonium salt. Fresh smears, chilled fixative, and freshly prepared and filtered reagents prevent most errors.
Glossary of Related Medical Terms
- Alkaline phosphatase (ALP): Enzyme that removes phosphate groups; the version inside mature neutrophils is what this stain measures.
- Azo dye: Colored compound formed when a diazonium salt reacts with naphthol; produces the visible granules during the LAP stain.
- BCR-ABL1 fusion gene: Faulty gene formed by the t(9;22) translocation; the genetic hallmark of CML.
- Diazonium salt: Reactive chemical that pairs with released naphthol to form the azo dye seen under the microscope.
- GPI anchor: Molecular tether holding LAP and other proteins on the cell surface; missing in PNH.
- Leukemoid reaction: Non-cancerous spike in white blood cells (often >50,000/µL) that can mimic leukemia.
- Left shift: More immature neutrophils than usual in peripheral blood.
- Naphthol AS-BI phosphate: The substrate that ALP cleaves during the stain.
- Philadelphia chromosome (Ph): Shortened chromosome 22 carrying BCR-ABL1; the cytogenetic hallmark of CML.
- Tyrosine kinase inhibitor (TKI): Drug class (imatinib and others) that blocks BCR-ABL1; first-line CML therapy.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Bain BJ, Bates I, Laffan MA. Dacie and Lewis Practical Haematology: Expert Consult: Online and Print (Elsevier) 12th Edition. 2016.
- Sugano, K., Hashi, K., Goto, M., Nishi, K., Maeda, R., Kono, K., Yamamoto, M., Okada, K., Kaga, S., Miwa, K., Mikami, T., & Masauzi, N. (2017). Semi-Automatic Rating Method for Neutrophil Alkaline Phosphatase Activity. Journal of clinical laboratory analysis, 31(1), e22022. https://doi.org/10.1002/jcla.22022
- Kondo, T., Tasaka, T., Tomioka, N., Sano, F., Tokunaga, H., Suemori, S., Tsujioka, T., Matsuhashi, Y., Nakanishi, H., Wada, H., Tohyama, K., & Sugihara, T. (2016). Low neutrophil alkaline phosphatase score is a new aspect of calreticulin-mutated myeloproliferative neoplasms. SpringerPlus, 5(1), 1146. https://doi.org/10.1186/s40064-016-2829-6
- Basquiera, A. L., Fassetta, F., Soria, N., Barral, J. M., Ricchi, B., & García, J. J. (2007). Accuracy of leukocyte alkaline phosphatase score to predict JAK2 V617F mutation. Haematologica, 92(5), 704–705. https://doi.org/10.3324/haematol.10991
- Lipshitz, J., Limaye, S., & Patel, D. (2010). Leukocyte alkaline phosphatase score correlation with bone marrow blast percentage in myelodysplastic syndrome. Acta haematologica, 124(3), 179–181. https://doi.org/10.1159/000320272
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Hochhaus, A., Baccarani, M., Silver, R. T., Schiffer, C., Apperley, J. F., Cervantes, F., Clark, R. E., Cortes, J. E., Deininger, M. W., Guilhot, F., Hjorth-Hansen, H., Hughes, T. P., Janssen, J. J. W. M., Kantarjian, H. M., Kim, D. W., Larson, R. A., Lipton, J. H., Mahon, F. X., Mayer, J., Nicolini, F., … Hehlmann, R. (2020). European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia, 34(4), 966–984. https://doi.org/10.1038/s41375-020-0776-2
- Sutherland, D. R., Keeney, M., & Illingworth, A. (2012). Practical guidelines for the high-sensitivity detection and monitoring of paroxysmal nocturnal hemoglobinuria clones by flow cytometry. Cytometry. Part B, Clinical cytometry, 82(4), 195–208. https://doi.org/10.1002/cyto.b.21023
- McPherson, R. A., & Pincus, M. R. (2021). Henry's Clinical Diagnosis and Management by Laboratory Methods (24th ed.). Elsevier.
- Coleman J. E. (1992). Structure and mechanism of alkaline phosphatase. Annual review of biophysics and biomolecular structure, 21, 441–483. https://doi.org/10.1146/annurev.bb.21.060192.002301

