Key Takeaways
Basophilia means a high basophil count, usually an absolute basophil count above about 0.1 x 10⁹/L. It is a sign of an underlying condition, not a disease in its own right.
- Role of Basophils ▾: Basophils drive allergic and inflammatory responses. They release histamine, heparin, and other chemicals, help defend against parasites, and steer the immune system toward Th2 (allergy-type) responses.
- Causes ▾: The most important causes of persistent basophilia are myeloproliferative neoplasms (MPNs) such as chronic myeloid leukemia (CML), polycythemia vera, essential thrombocythemia, and primary myelofibrosis. Reactive causes include allergies, chronic inflammation, and an underactive thyroid.
- Symptoms ▾: Basophilia rarely causes symptoms by itself. Any symptoms (fatigue, an enlarged spleen, itching, or allergy signs) come from the underlying condition.
- Investigations ▾: Starts with a complete blood count and blood smear first, then molecular tests (BCR::ABL1, JAK2, CALR, MPL) and a bone marrow biopsy if a blood cancer is suspected.
- Treatment ▾: Treatment targets the cause, not the basophil count: tyrosine kinase inhibitors for CML, cytoreduction or phlebotomy for other MPNs, antihistamines for allergies, and thyroid hormone for hypothyroidism.
*Click ▾ for more information
Introduction
Basophilia is a high number of basophils in the blood. Basophils are the rarest of the white blood cells, so when their count climbs, it usually means something else is going on. That "something" can be as ordinary as a stubborn allergy or as serious as a blood cancer. This article explains what the finding means, what causes it, how doctors track down the cause, and how it is managed [1].
What Do Basophils Actually Do?
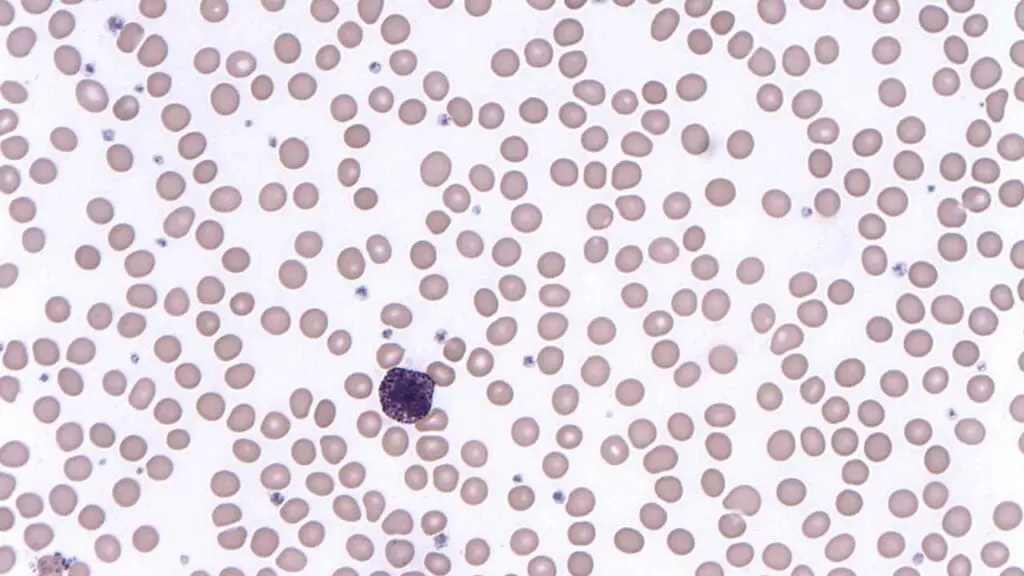
Basophils are small but busy. Under the microscope, their cytoplasm is packed with dark blue-purple granules so dense they hide the nucleus. Those granules are the key to their job: they store and release the chemicals that power allergic and inflammatory reactions.

Allergic and Hypersensitivity Reactions
This is the function basophils are best known for. The chain of events is straightforward. Basophils carry high-affinity receptors (called FcεRI) for IgE antibodies on their surface. When an allergen latches onto those IgE antibodies, it triggers degranulation, the rapid release of stored chemicals. The main mediators are:
- Histamine. It widens blood vessels and makes them leaky, which brings redness, swelling, itching, a runny nose, and watery eyes.
- Heparin. A natural blood thinner that keeps blood flowing to the inflamed area, supporting healing and the arrival of more immune cells.
- Leukotrienes and cytokines (such as IL-4 and IL-13). These are made fresh on demand. They amplify inflammation, recruit other immune cells like eosinophils, and push T helper cells toward the Th2 pattern that drives allergies and anti-parasite defense.
Defense Against Parasites
Eosinophils lead the fight against parasitic worms, but basophils help. By releasing their mediators and cytokines, they recruit and switch on the other immune cells needed to clear large parasites.
Steering the Immune Response
Basophils also shape the bigger immune picture. Their IL-4 output helps activate B cells to make antibodies (including IgE), nudges CD4+ T cells toward the Th2 phenotype, and lets basophils talk to other innate and adaptive immune cells.
Fueling Chronic Inflammation
When inflammation drags on, basophils keep it going. They release histamine and leukotrienes over and over, keep driving Th2 (allergy-type) immunity, and interact with cells like dendritic cells and T cells to sustain the cycle. This is part of why they matter in conditions such as asthma, atopic dermatitis (eczema), and inflammatory bowel disease.
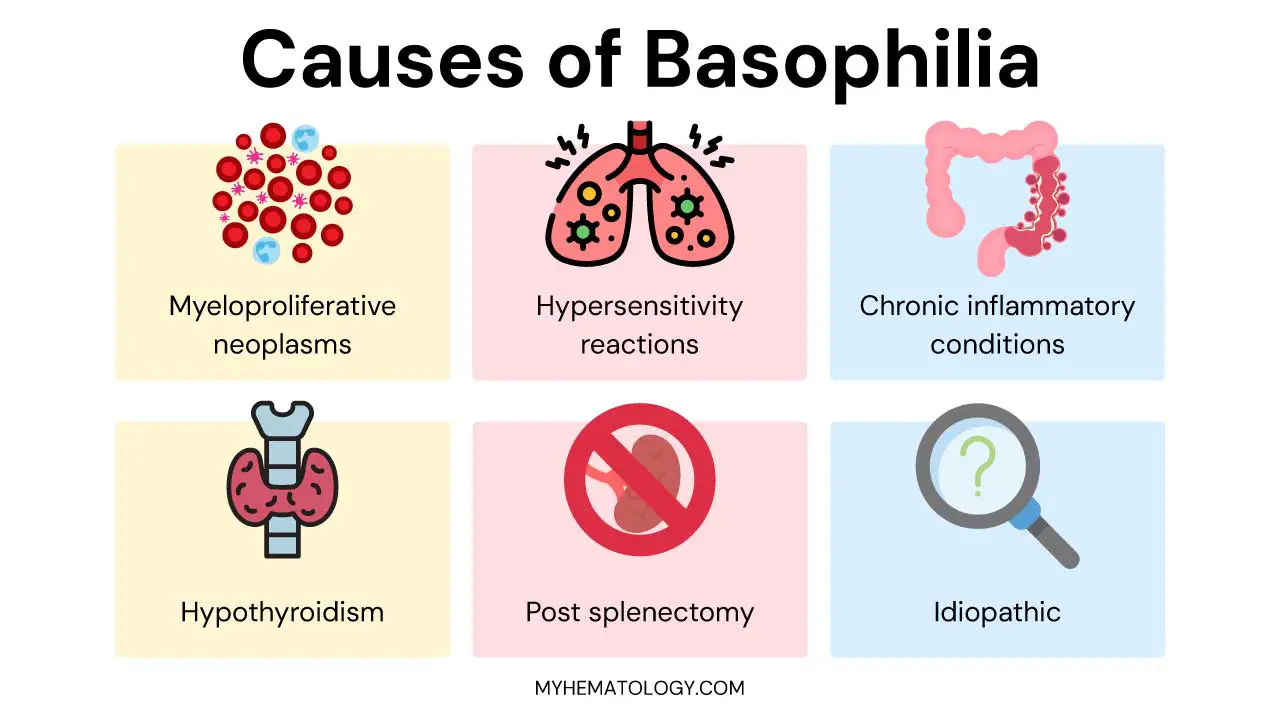
Causes of Basophilia (High Basophils)
Basophilia is a sign, not a diagnosis. The causes fall into two broad camps: reactive (the body responding to something) and neoplastic (a blood cancer). The neoplastic causes are the ones you must not miss.
Myeloproliferative Neoplasms (MPNs)
These are the most important and most serious causes of lasting basophilia. MPNs are chronic conditions where the bone marrow overproduces one or more blood cell types. Because basophils grow from the same myeloid stem cell line that is disturbed in these disorders, a high basophil count is a common feature [1].
- Chronic myeloid leukemia (CML). The classic culprit, and usually the first suspect when basophilia is significant. CML is defined by the Philadelphia chromosome, t(9;22), which creates the BCR::ABL1 fusion gene. Basophilia is often one of the earliest signs.
- Polycythemia vera (PV). Mainly an overproduction of red blood cells, but white cells (including basophils) and platelets often rise too. Most patients carry the JAK2 V617F mutation.
- Essential thrombocythemia (ET). Mainly too many platelets, sometimes with mild to moderate basophilia. Often linked to JAK2, CALR, or MPL mutations.
- Primary myelofibrosis (PMF). Marked by scarring of the bone marrow, which leads to blood production outside the marrow, an enlarged spleen, and sometimes basophilia.
- Less common MPNs. Atypical CML and chronic myelomonocytic leukemia (CMML) can also raise basophils.
Why the basophil number matters in MPNs. Recent 2025 data has firmly established that basophilia is not just an incidental finding. In primary myelofibrosis, polycythemia vera, and essential thrombocythemia, elevated basophils closely correlate with specific high-risk genetic mutations and shorter failure-free survival, making it a recognized prognostic marker of more active disease [3,4].
Allergic and Hypersensitivity Reactions
Because basophils sit at the center of allergy, their numbers can climb in allergic disease. This is a reactive cause.
- Acute reactions. Severe events like anaphylaxis, acute hives (urticaria), or angioedema can cause a brief, temporary rise, though this is less typical than the eosinophilia seen in allergy.
- Chronic allergic conditions. Ongoing allergen exposure in allergic asthma, chronic allergic rhinitis, or atopic dermatitis can keep basophils mildly to moderately elevated.
- Drug or food allergies. Specific reactions can sometimes nudge basophils up.
Chronic Inflammatory and Infectious Conditions
- Inflammatory bowel disease (IBD). Both Crohn's disease and ulcerative colitis are often linked to basophilia, reflecting ongoing immune activity in the gut.
- Rheumatoid arthritis (RA). This autoimmune joint disease can sometimes raise basophils.
- Chronic infections. Less commonly than eosinophilia, but basophilia has been reported with some chronic bacterial infections (such as tuberculosis) and certain viral infections.
Endocrine Disorders
- Hypothyroidism (an underactive thyroid). A long-recognized teaching association. When the thyroid slows the body's metabolism, basophil counts can edge up. The exact mechanism is not fully understood and may involve altered cytokine signaling.
After Spleen Removal (Post-Splenectomy)
The spleen normally filters blood cells from circulation. After it is removed, several cell counts, including basophils, can rise temporarily.
Idiopathic Basophilia (High Basophils)
Sometimes a thorough workup finds no cause. This is called idiopathic basophilia, a diagnosis of exclusion.
Signs and Symptoms Associated with Basophilia
Here is the key point: basophilia itself usually causes no specific symptoms. Whatever a patient feels comes from the underlying condition. So when clinicians see basophilia, they shift their attention to finding the primary disease.
Therefore, when evaluating a patient with basophilia (high basophils), the clinician's focus shifts to identifying the primary disease process.
From Myeloproliferative Neoplasms (MPNs)
Because MPNs are a frequent cause, their symptoms are the ones most often seen. They tend to be non-specific, which is exactly why a careful workup matters.
- Constitutional ("B") symptoms: persistent fatigue not relieved by rest, unexplained weight loss, drenching night sweats, and low-grade fever.
- Splenomegaly (enlarged spleen): abdominal fullness, feeling full quickly after small meals (early satiety), and left-upper-quadrant pain.
- Effects from other blood cell lines: anemia (pallor, breathlessness, dizziness), abnormal platelet counts (easy bruising, or burning red hands and feet known as erythromelalgia, or clotting), and high white cells (more infections).
- Pruritus (itching): a prominent symptom in MPNs, especially polycythemia vera. It is thought to come partly from histamine released by basophils and mast cells, and it often worsens after a warm shower.
- Bone or joint pain: especially in primary myelofibrosis.
From Allergic Reactions
If an allergy is behind the basophilia, expect classic allergy symptoms driven by histamine release: hives, swelling (angioedema), and itching on the skin; sneezing, congestion, and wheezing in the airways; and cramping, nausea, or diarrhea from food allergy. Anaphylaxis is a medical emergency, with airway swelling, a sharp drop in blood pressure, and widespread hives.
From Chronic Inflammation or Infection
Symptoms reflect the specific disease: bloody diarrhea and weight loss in IBD; joint pain and stiffness in RA; persistent cough, fever, and night sweats in tuberculosis.
From Hypothyroidism
Fatigue, weight gain, cold intolerance, constipation, dry skin, hair loss, a slow heart rate, and low mood.
How Basophilia is Investigated
Lab testing is essential because basophilia is a finding, not a diagnosis. The approach is sequential: start simple, then escalate if a serious cause is suspected [2].
A Note on the Number Itself
The absolute basophil count (cells per liter) is the figure that matters clinically, with a normal adult range of roughly 0.02–0.1 x 10⁹/L. The relative count (basophils as a percentage of all white cells) can be misleading on its own, because it shifts when other cell counts change. While the 2022 International Consensus Classification utilized a 20% relative cutoff to define accelerated-phase CML [6], 2026 clinical data demonstrates that absolute basophil concentration is a significantly more accurate predictor of tyrosine kinase inhibitor (TKI) failure than percentages. Consequently, clinical practice is shifting toward absolute thresholds (e.g., ≥12 x 10⁹/L) for risk assessment [8].
Initial Screening Tests
Complete blood count (CBC) with differential. This is the cornerstone. It gives the absolute basophil count and shows the other cell lines. Basophilia alongside high neutrophils, eosinophils, or platelets strongly suggests an MPN. Isolated basophilia is less common and points more toward allergic or thyroid causes. Anemia or low platelets may appear in myelofibrosis or chronic inflammation.
Peripheral blood smear. A trained scientist examines the blood under a microscope, catching things automated counters miss. Immature cells (blasts, promyelocytes, myelocytes) strongly suggest an MPN, especially CML. The smear may also show eosinophilia, abnormal cell shapes (such as teardrop red cells in myelofibrosis), or nucleated red cells. The smear also confirms machine flags, since analyzers can occasionally misclassify cells and report a falsely high basophil count
Targeted Investigations (Based on Clinical Suspicion)
Bone marrow examination (aspirate and biopsy). Done when an MPN is suspected, particularly with persistent basophilia plus other count abnormalities or immature cells on the smear. Chromosome analysis looks for the Philadelphia chromosome, t(9;22). Special stains (such as tryptase) can quantify mast cells if mastocytosis is on the differential. (Mast cells and basophils share some features and chemicals like histamine, which is why mastocytosis can enter the picture.)
Molecular genetic testing. Essential for diagnosing MPNs.
- BCR::ABL1 fusion gene: the hallmark of CML, tested by PCR. Its presence confirms CML.
- JAK2 V617F: common in PV, ET, and PMF.
- CALR and MPL: tested in suspected ET or PMF, especially when JAK2 is negative.
- Other genes (CSF3R, SRSF2, ASXL1) may be tested depending on the suspected subtype. Next-generation sequencing (NGS) panels are now standard practice to identify a broader range of mutations when initial single-gene tests are negative, aiding in both definitive diagnosis and prognostic risk stratification [7].
Allergy testing. If allergy seems likely and MPN markers are negative: total and specific IgE, skin prick tests, and the basophil activation test (a functional test of how basophils respond to an allergen).
Thyroid function tests. If hypothyroidism is suspected from the clinical picture.
Inflammatory markers (ESR and CRP). Non-specific, but they support the presence of chronic inflammation in conditions like IBD or RA.
Parasitology/infectious testing. If parasitic infection is suspected (for example, relevant travel history with eosinophilia), stool ova and parasite exams or serology may help.

Treatment and Management
Treatment is aimed almost entirely at the underlying cause, not the basophil count. The number on its own rarely needs treating unless it is exceptionally high (very rare) or it is driving symptoms such as MPN-related itching from histamine release [1].
What this looks like in practice depends on the cause:
- CML: tyrosine kinase inhibitors (TKIs) such as imatinib, which block the BCR::ABL1 protein. These transformed CML from a fatal disease into a chronic, often well-controlled one.
- Other MPNs: approaches such as phlebotomy (removing blood) and low-dose aspirin in polycythemia vera, and cytoreductive drugs to lower overactive cell production, chosen according to the specific neoplasm and the patient's risk.
- Allergic causes: antihistamines and avoiding the trigger, with broader allergy management as needed.
- Hypothyroidism: thyroid hormone replacement (levothyroxine).
When a full workup finds no cause and the basophilia is mild and symptom-free, doctors often choose a "watch and wait" approach with periodic CBCs. Treatment is reserved for when symptoms or other count abnormalities appear.
A Note on Evolving Classifications
In 2022, two major classification systems updated how they handle CML phases, and they disagreed. The 2022 ICC kept the accelerated phase and defined it using just three variables: blast percentage, basophil count, and additional cytogenetic abnormalities. The 2022 WHO 5th edition took a different path. It deleted the accelerated phase entirely, judging the designation less relevant in the era of effective TKI therapy, while the European LeukemiaNet and NCCN guidelines retained it.
Adding to this landscape, the 2025 European LeukemiaNet (ELN) recommendations acknowledged this diagnostic schism. While remaining neutral on the formal label of the accelerated phase, the ELN emphasizes that patients presenting with advanced features such as rapidly rising basophils require vigilant monitoring and often early transition to second-generation TKIs [9].
The Practical Lesson
"High basophils mean progression" is a useful rule of thumb, but the exact thresholds and even whether "accelerated phase" exists now depend on which system you follow [5,6].
Frequently Asked Questions (FAQs)
Is basophilia dangerous?
Basophilia itself rarely causes harm. The concern is the cause behind it. Mild basophilia from an allergy or infection is usually harmless and temporary. Persistent or markedly high basophilia can be an early sign of a blood cancer such as CML, which does need treatment. That is why doctors investigate the cause rather than treating the number.
Can high basophils make you tired?
No. High basophils do not directly cause fatigue. Tiredness comes from the underlying condition driving the count up, such as a myeloproliferative neoplasm or chronic inflammation.
What is the most serious cause of high basophils?
Myeloproliferative neoplasms, a group of chronic blood cancers, are the most serious causes. CML is the classic example, and basophilia is often one of its earliest findings.
How is the cause of basophilia diagnosed?
It starts with a complete blood count and a blood smear. If a blood cancer is suspected, doctors add molecular tests (BCR::ABL1, JAK2, CALR, MPL) and often a bone marrow biopsy. If allergy or thyroid disease is more likely, allergy testing or thyroid function tests are done instead.
Can COVID-19 affect basophil levels?
Yes. During acute COVID-19, especially severe illness, basophils more often drop than rise, and a low count can signal a worse outcome. As patients recover, the count tends to rebound and can briefly rise above normal.
Glossary of Related Medical Terms
- Basophil: The rarest type of white blood cell. Its granules release histamine and other chemicals during allergic and inflammatory reactions.
- Basophilia: An abnormally high number of basophils in the blood, usually above about 0.1 x 10⁹/L. It is a sign of an underlying condition, not a disease by itself.
- Absolute basophil count: The actual number of basophils per liter of blood, as opposed to the percentage of all white cells. This is the number that matters clinically.
- Degranulation: The process where a basophil rapidly dumps its stored chemicals (like histamine) into surrounding tissue.
- Histamine: A chemical that widens blood vessels and makes them leaky, causing redness, swelling, and itching.
- Myeloproliferative neoplasm (MPN): A group of chronic blood cancers in which the bone marrow makes too many blood cells. Examples include CML, PV, ET, and PMF.
- Chronic myeloid leukemia (CML): A blood cancer driven by the BCR::ABL1 fusion gene (the Philadelphia chromosome). Basophilia is a classic feature.
- Philadelphia chromosome: An abnormal chromosome formed when parts of chromosomes 9 and 22 swap places, creating the BCR::ABL1 gene that causes CML.
- JAK2 V617F: A common gene mutation found in PV, ET, and PMF.
- Tyrosine kinase inhibitor (TKI): A targeted drug (such as imatinib) that blocks the abnormal protein driving CML.
- Splenomegaly: An enlarged spleen, which can cause belly fullness and feeling full quickly after eating.
- Pruritus: The medical term for itching.
- Peripheral blood smear: A drop of blood spread on a slide and examined under a microscope to look at cell shape and detect abnormal cells.
- Reactive: Describes a blood count change caused by the body responding to something (an allergy, infection, or inflammation) rather than by cancer.
- Idiopathic: Having no identifiable cause after thorough investigation.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Sticco KL, Pandya NK, Zubair M, et al. Basophilia. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535365/
- Feriel, J., Depasse, F., & Geneviève, F. (2020). How I investigate basophilia in daily practice. International journal of laboratory hematology, 42(3), 237–245. https://doi.org/10.1111/ijlh.13146
- Dingli, S., Fathima, S., Faldu, P., Gangat, N., Dingli, D., & Tefferi, A. (2025). Basophilia and eosinophilia in primary myelofibrosis: phenotype, genotype, and prognostic correlates. Blood cancer journal, 15(1), 72. https://doi.org/10.1038/s41408-025-01285-x
- Faldu, P., Yousuf, M., Abdelmagid, M., Dingli, S., Begna, K., Zepeda Mendoza, C. J., Reichard, K. K., He, R., Pardanani, A., Gangat, N., & Tefferi, A. (2025). Basophilia and eosinophilia in polycythemia vera and essential thrombocythemia: clinical, genotype, and prognostic correlates. Annals of hematology, 104(6), 3223–3234. https://doi.org/10.1007/s00277-025-06422-x
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Mroczkowska-Bękarciak, A., Szeremet, A., Chyrko, O., & Wróbel, T. (2026). CALR-mutant myeloproliferative neoplasms: insights from next-generation sequencing. Journal of applied genetics, 67(1), 155–164. https://doi.org/10.1007/s13353-025-00947-7
- Vantyghem, S., Peterlin, P., Thépot, S., Ménard, A., Dubruille, V., Debord, C., Guillaume, T., Garnier, A., Le Bourgeois, A., Wuilleme, S., Godon, C., Theisen, O., Eveillard, M., Delaunay, J., Maisonneuve, H., Morineau, N., Villemagne, B., Vigouroux, S., Subiger, F., Lestang, E., … Le Bris, Y. (2021). Diagnosis and prognosis are supported by integrated assessment of next-generation sequencing in chronic myeloid malignancies. A real-life study. Haematologica, 106(3), 701–707. https://doi.org/10.3324/haematol.2019.242677
- Valent, P., Sotlar, K., Blatt, K., Hartmann, K., Reiter, A., Sadovnik, I., Sperr, W. R., Bettelheim, P., Akin, C., Bauer, K., George, T. I., Hadzijusufovic, E., Wolf, D., Gotlib, J., Mahon, F. X., Metcalfe, D. D., Horny, H. P., & Arock, M. (2017). Proposed diagnostic criteria and classification of basophilic leukemias and related disorders. Leukemia, 31(4), 788–797. https://doi.org/10.1038/leu.2017.15


