Key Takeaways
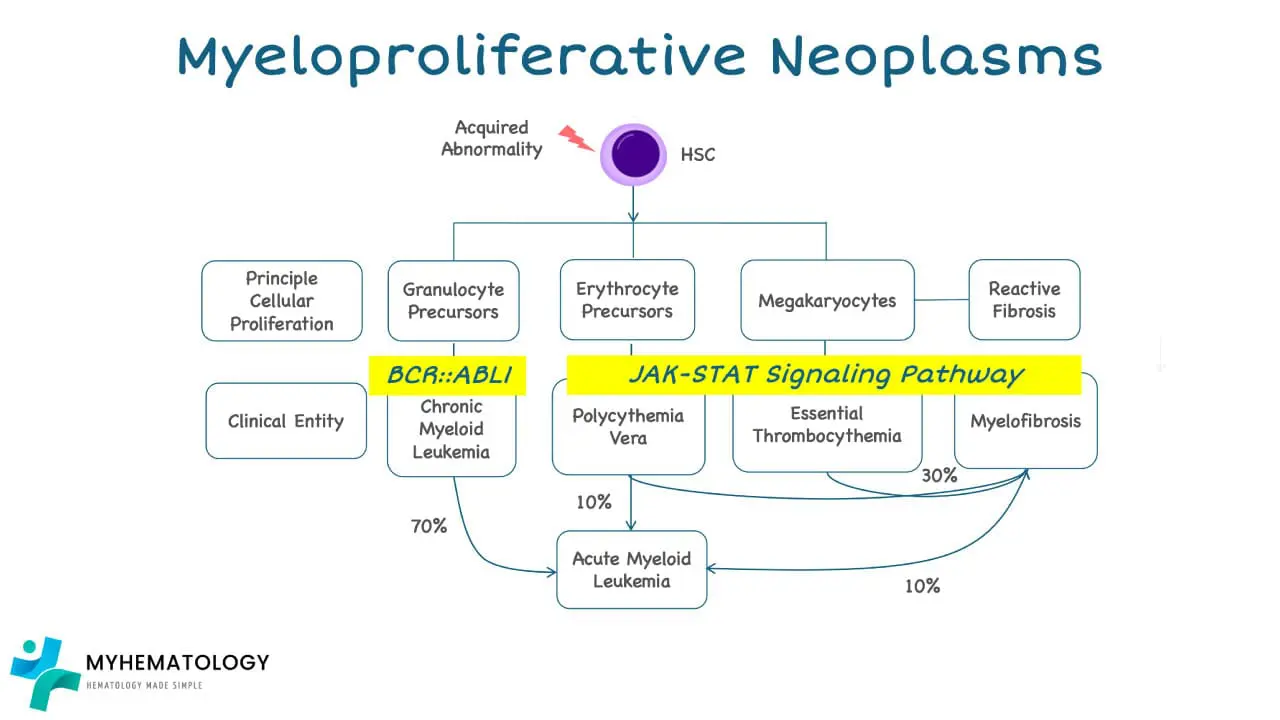
A myeloproliferative neoplasm is a chronic blood cancer in which bone marrow makes too many mature blood cells — red cells, white cells, platelets, or a combination. The three classical BCR::ABL1-negative MPNs are essential thrombocythemia (ET), polycythemia vera (PV), and primary myelofibrosis (PMF). Chronic myeloid leukemia (CML) is a separate BCR::ABL1-positive entity.
- Driver mutations ▾: in JAK2, CALR, or MPL are found in about 90% of patients. They lock the JAK-STAT signaling pathway in the "on" position, which fuels uncontrolled blood-cell production.
- Diagnosis ▾: Diagnosis rests on a complete blood count, peripheral smear, bone marrow biopsy, and molecular testing, interpreted against the WHO 5th edition (2022) or International Consensus Classification (2022) criteria [1,2].
- Treatment ▾: Treatment aims to lower thrombosis risk, ease symptoms, and normalize blood counts. It includes aspirin, phlebotomy, hydroxyurea, interferons (ropeginterferon alfa-2b), JAK inhibitors (including new once-daily extended-release formulations), emerging targeted agents like hepcidin mimetics (rusfertide), and, in selected cases, allogeneic stem cell transplant.
- Prognosis ▾: Prognosis varies by subtype: ET is the most indolent, PV is intermediate, and PMF is the most aggressive, with the highest risk of transformation to acute myeloid leukemia.
*Click ▾ for more information
What Is a Myeloproliferative Neoplasm?
A myeloproliferative neoplasm (MPN) is a clonal disease of the bone marrow. A single hematopoietic stem cell acquires a mutation, gains a growth advantage, and pushes out too many mature blood cells. The result is the opposite of bone marrow failure. Instead of empty marrow, you see a marrow that will not stop working.
The three "classical" MPNs are essential thrombocythemia, polycythemia vera, and primary myelofibrosis. They are sometimes grouped together as the BCR::ABL1-negative MPNs to distinguish them from chronic myeloid leukemia, which is BCR::ABL1-positive and is treated as a related but separate disease [1,2].
The three classical MPNs at a glance
- Essential thrombocythemia (ET): persistently elevated platelet count, with proliferation of mature, hyperlobulated megakaryocytes in the marrow.
- Polycythemia vera (PV): elevated red cell mass, raised hemoglobin and hematocrit, often with smaller increases in white cells and platelets (panmyelosis).
- Primary myelofibrosis (PMF): progressive marrow scarring, abnormal megakaryocytes, and a leukoerythroblastic blood picture (immature white cells and nucleated red cells in circulation).
How common are MPNs?
MPNs are uncommon but not vanishingly rare. Global prevalence is estimated at roughly 35–50 cases per 100,000 people because the disease is chronic and patients live for years to decades with it. Most diagnoses occur after age 60, although younger adults are affected. ET makes up the largest share (around 50–60% of MPN diagnoses), followed by PV (15–25%) and PMF (10–20%) [3,5].
How MPNs Develop
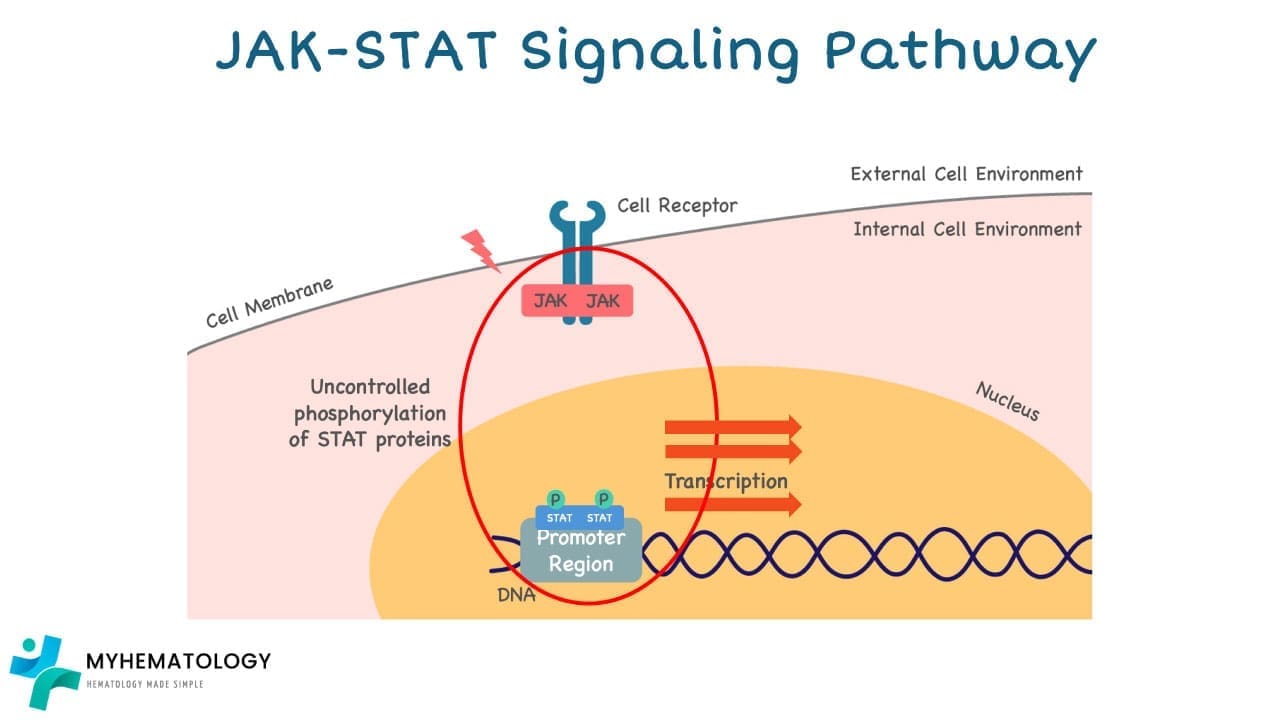
To understand MPN treatment, it helps to understand a single signaling pathway: JAK-STAT. Cytokines such as erythropoietin and thrombopoietin bind their receptors on hematopoietic cells. The receptor pulls in a kinase called JAK2, which phosphorylates STAT proteins. The phosphorylated STATs travel to the nucleus and switch on genes for cell growth and survival. When the cytokine signal stops, the pathway shuts off.
In MPNs, that off-switch fails. A mutation in JAK2, CALR, or MPL leaves the pathway constantly active, even without a cytokine signal — a state called constitutive activation [3,5].
The driver mutations
The frequencies below summarize the classical pattern in BCR::ABL1-negative MPNs [3,4,5]:
- JAK2 V617F is the most common mutation. It is found in roughly 95% of PV, 50–60% of ET, and 50–65% of PMF. The mutation swaps a single amino acid (valine for phenylalanine at position 617) and breaks the autoinhibitory domain that normally keeps JAK2 quiet.
- JAK2 exon 12 mutations account for most of the remaining PV cases that are JAK2 V617F-negative. They typically cause an isolated rise in red cells (erythrocytosis) without thrombocytosis.
- CALR mutations (insertions or deletions in exon 9) are found in about 25% of ET and PMF patients. CALR type 1 mutations in PMF are linked to better survival than JAK2 V617F.
- MPL mutations in exon 10 are seen in around 3–5% of ET and PMF.
- Triple-negative MPN describes the 10–15% of ET and PMF patients with none of the three classical drivers. Next-generation sequencing often finds non-canonical drivers in this group.
These mutations are usually mutually exclusive — a single patient typically carries one driver, not several.
Beyond the driver mutations, additional mutations can stack on top and worsen prognosis. The five "high-molecular-risk" (HMR) mutations recognized in PMF are ASXL1, SRSF2, EZH2, IDH1/2, and U2AF1 Q157. Modern myelofibrosis risk scores such as MIPSS70+ v2.0 incorporate them alongside karyotype and clinical features [10].
Risk Factors
The cause of any individual MPN is rarely identifiable, but several risk factors are well established.
- Age. Risk rises steadily after age 50. Median age at PV and PMF diagnosis sits around 65–70.
- Family history. A first-degree relative with an MPN raises baseline risk roughly five- to seven-fold, although absolute risk stays low.
- Sex. ET shows a slight female predominance; PV shows a slight male predominance.
- Radiation and chemicals. High-dose ionizing radiation and chronic exposure to benzene have been linked to MPN risk.
- Smoking has been associated with an increased risk of polycythemia vera in particular.
General and Specific Symptoms
MPN symptoms reflect their pathophysiology. Once you know what the marrow is overproducing, the clinical picture follows.
Symptoms shared across MPNs
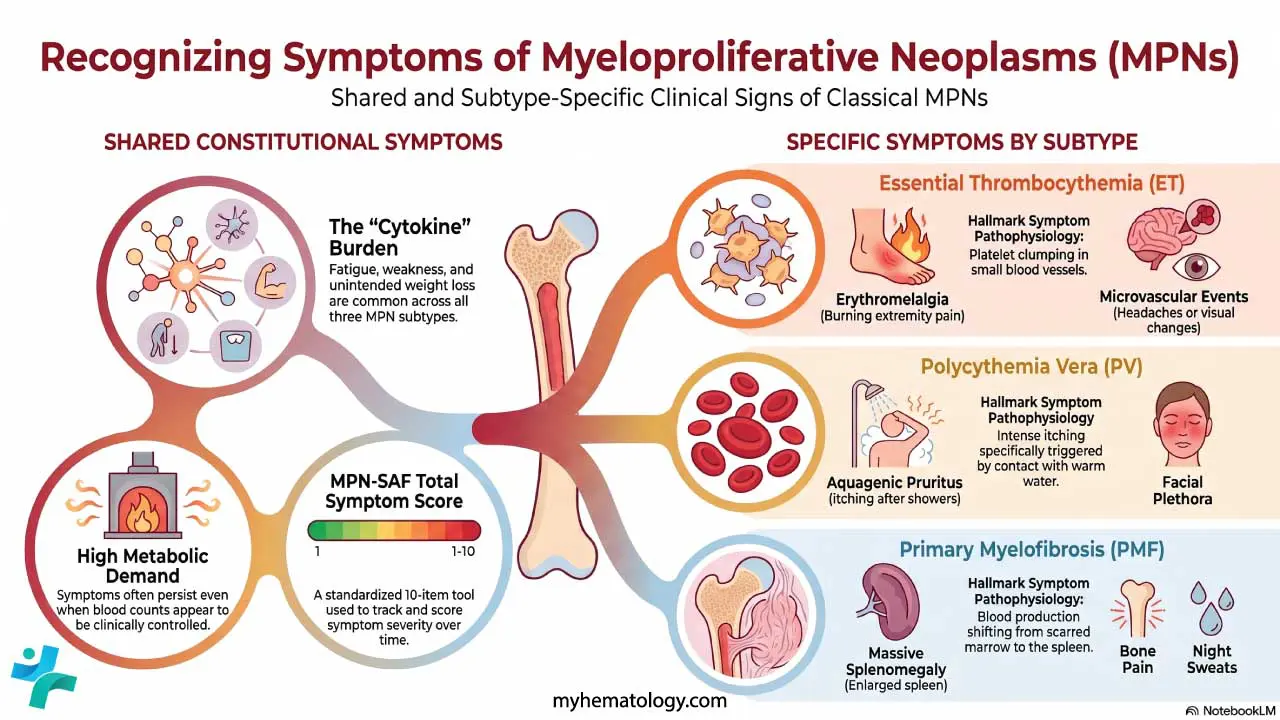
Fatigue, weakness, and unintended weight loss are common across all three subtypes. They often track with cytokine release, marrow stress, and increased metabolic demand. Patients sometimes describe these as the most disruptive features of life with an MPN, even when blood counts look "controlled."
Specific Symptoms by Subtype

- Essential thrombocythemia. Too many platelets means two opposite problems can occur. Microvascular events such as headache, visual changes, and erythromelalgia (burning pain and redness in the hands or feet) reflect platelet clumping in small vessels. Larger thrombotic events, including stroke and deep vein thrombosis, can also occur. Paradoxically, very high platelet counts can also impair clotting and cause bleeding.
- Polycythemia vera. Thicker, slower-flowing blood produces headache, dizziness, blurred vision, and facial plethora (a ruddy, flushed face). Aquagenic pruritus (intense itching after a warm shower) is a hallmark. Thrombosis, especially in unusual sites such as hepatic veins (Budd-Chiari syndrome), is a leading cause of morbidity.
- Primary myelofibrosis. As marrow scars, blood production shifts to the spleen and liver (extramedullary hematopoiesis), so massive splenomegaly is common and can extend into the pelvis. Patients also experience constitutional symptoms: night sweats, low-grade fever, and bone pain. Anemia is very common and is a major driver of fatigue.
For tracking symptoms over time, the MPN-SAF Total Symptom Score (MPN-SAF TSS) is now standard in clinical practice and trials. It scores ten common MPN symptoms and gives a single number that can be followed alongside blood counts.
Investigating Myeloproliferative Neoplasms
Working up a suspected MPN follows a clear sequence: rule out reactive causes, then build the diagnosis from blood, marrow, and molecular evidence.
Complete blood count and peripheral smear
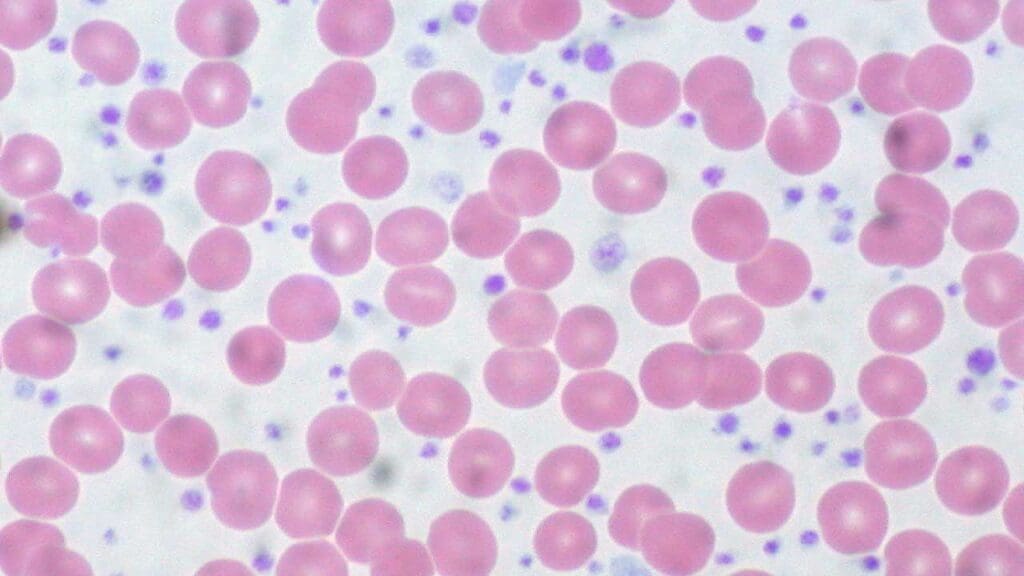
The CBC usually triggers the workup. Look for an isolated thrombocytosis (suggesting ET), an elevated red-cell count or hematocrit (suggesting PV), or a leukoerythroblastic picture with anemia and teardrop red cells (suggesting PMF). The smear adds visual confirmation: giant platelets in ET, plethoric red cells in PV, and tear-drop red cells with circulating immature white cells in PMF.
Bone marrow aspiration and biopsy
Bone marrow biopsy is essential for diagnosis. Findings include hypercellularity adjusted for age, distinctive megakaryocyte morphology by subtype, and the degree of reticulin or collagen fibrosis (graded 0–3). PV shows panmyelosis with prominent erythroid and megakaryocytic lineages. ET shows enlarged, hyperlobulated megakaryocytes with no significant fibrosis. PMF shows atypical clustered megakaryocytes with reticulin or collagen fibrosis.
Molecular testing
- Targeted PCR detects JAK2 V617F first because it is the most common mutation.
- If JAK2 V617F is negative, testing extends to JAK2 exon 12 (in suspected PV) or CALR and MPL (in suspected ET or PMF).
- Next-generation sequencing (NGS) panels are used to look for high-molecular-risk and non-canonical mutations, and they are now routine in PMF for risk stratification.
Other useful tests
- Serum erythropoietin (EPO) is the key test that separates PV from secondary polycythemia. In PV, EPO is suppressed because the marrow makes red cells without needing the signal. In secondary causes (chronic hypoxia, smoking, EPO-secreting tumors), EPO is elevated.
- Serum LDH and uric acid rise with high cell turnover.
- Imaging (ultrasound, CT, or MRI) documents splenomegaly and screens for splenic or portal vein thrombosis.
The 2022 classification systems
Two parallel diagnostic frameworks were published in 2022: the WHO 5th edition (WHO-HAEM5) and the International Consensus Classification (ICC) [1,2,6]. For PV, ET, and PMF, the two systems are largely concordant. Both require integration of clinical, morphologic, and molecular data, and both formally recognize early/prefibrotic PMF as a distinct entity from overt PMF.
Treatment and Management
Treatment plans are tailored to the specific myeloproliferative neoplasm, the patient's age and comorbidities, the driver mutation, and the calculated risk of thrombosis or progression.
As of the NCCN Guidelines Version 2.2026, there has been a strong philosophical shift toward phenotype-driven therapy. Rather than a rigid, stepwise medication algorithm based solely on risk scores, treatment selection is increasingly tailored to the patient's dominant clinical problem such as splenomegaly, anemia, or high symptom burden allowing for highly individualized care [11].
Goals of treatment
- Reduce the risk of thromboembolic events (the dominant cause of morbidity in PV and ET).
- Control symptoms and improve quality of life.
- Normalize blood counts where possible.
- Slow disease progression and, in selected cases, achieve cure.
Polycythemia vera
For low-risk PV (younger patients with no prior thrombosis), the standard backbone is therapeutic phlebotomy (target hematocrit <45%) plus low-dose aspirin. High-risk patients (age ≥60 or prior thrombosis) add cytoreductive therapy.
For cytoreduction, hydroxyurea has long been the workhorse. Ropeginterferon alfa-2b (Besremi), a long-acting pegylated interferon, was FDA-approved in 2021 for adults with PV. NCCN guidelines (v1.2024) now list it as a preferred first-line cytoreductive option for both low- and high-risk PV, regardless of treatment history [8]. Ropeginterferon has shown durable hematologic responses and reductions in JAK2 V617F allele burden in long-term follow-up.
A major recent shift in PV management is the development of rusfertide, a first-in-class hepcidin mimetic. Based on the successful Phase 3 VERIFY trial, rusfertide restricts iron availability to the bone marrow, effectively shutting off the overproduction of red blood cells at the source. It has been shown to provide sustained hematocrit control (under 45%) and drastically reduce or eliminate the need for frequent, draining therapeutic phlebotomies [12]. Additionally, a once-daily, extended-release (XR) formulation of ruxolitinib is now approved for PV, improving patient adherence and offering consistent 24-hour drug exposure without peak-and-trough side effects [13].
Essential thrombocythemia
ET management hinges on the IPSET-thrombosis score. Very-low-risk patients may need only observation. Low-risk patients often receive low-dose aspirin if they carry JAK2 V617F or have cardiovascular risk factors. High-risk patients add cytoreduction, usually hydroxyurea, with anagrelide or interferon as alternatives.
However, recent data has challenged the traditional reliance on hydroxyurea and anagrelide. Ropeginterferon alfa-2b is now recognized in the 2026 NCCN Guidelines for ET management, following the Phase 3 SURPASS ET trial which demonstrated its superiority over anagrelide as a second-line treatment for high-risk, hydroxyurea-resistant patients [14]. Furthermore, disease-modifying therapies are actively entering the clinic; recent data for INCA44989, a novel monoclonal antibody targeting mutated calreticulin (mutCALR), showed significant overall response rates and the ability to reduce the mutant allele burden in ET patients, pushing treatment goals beyond mere symptom control [15].
Primary myelofibrosis
PMF is the most therapeutically challenging MPN, and the treatment landscape has expanded significantly with JAK inhibitors [7]:
- Ruxolitinib was the first approved JAK1/JAK2 inhibitor. It reduces spleen size and constitutional symptoms in MF and is also approved for PV. It is now available in a once-daily, extended-release (XR) tablet formulation, which improves tolerability and maintains steady therapeutic levels without the traditional twice-daily dosing [13].
- Fedratinib is a JAK2-selective inhibitor used in patients who fail or do not tolerate ruxolitinib.
- Pacritinib has a specific niche: MF with severe thrombocytopenia (platelets <50 × 10⁹/L), where ruxolitinib is poorly tolerated.
- Momelotinib (Ojjaara) was FDA-approved for intermediate- or high-risk MF in adults. It inhibits JAK1, JAK2, and ACVR1. The ACVR1 effect lowers hepcidin, frees up iron, and improves erythropoiesis. Because older JAK inhibitors can worsen anemia, clinical guidelines now heavily emphasize momelotinib as a preferred frontline choice for patients presenting with an anemia-dominant phenotype [7,11].
For younger fit patients with high-risk PMF, allogeneic stem cell transplantation remains the only curative option but carries substantial morbidity and mortality.
Supportive care and monitoring
All MPN patients need ongoing monitoring: regular CBCs, periodic symptom assessment using MPN-SAF TSS, imaging when splenomegaly progresses, and repeat bone marrow biopsy if disease behavior changes. Cardiovascular risk reduction, smoking cessation, and good control of blood pressure and lipids meaningfully reduce thrombotic events [9].

Prognosis and the Risk of Transformation
Prognosis depends on subtype, age, blood counts, mutation profile, and karyotype.
- Essential thrombocythemia has the best prognosis, with life expectancy approaching that of the age-matched general population. Risk of transformation to AML is around 1–5% over a lifetime.
- Polycythemia vera has a median survival in the range of 14–20 years. Risk of transformation to AML is around 5–10%, with secondary myelofibrosis (post-PV MF) developing in around 10–20% over 15–20 years.
- Primary myelofibrosis has the most variable prognosis. Median survival ranges from a few years in high-risk disease to over a decade in low-risk disease. Risk of transformation to AML reaches 10–20% over 10 years and is higher in the presence of high-molecular-risk mutations [10].
Modern prognostic scores i.e. IPSET for ET, IPSS-R for PV, and MIPSS70+ v2.0 or GIPSS for PMF, guide both intensity of treatment and decisions about transplant referral [10].
Frequently Asked Questions (FAQs)
What is a myeloproliferative neoplasm?
A myeloproliferative neoplasm (MPN) is a chronic blood cancer in which the bone marrow makes too many mature blood cells. The three classical BCR::ABL1-negative MPNs are essential thrombocythemia (too many platelets), polycythemia vera (too many red cells), and primary myelofibrosis (marrow scarring with abnormal blood-cell production). Most cases are driven by a mutation in JAK2, CALR, or MPL.
How are MPNs diagnosed?
Diagnosis combines a complete blood count, peripheral blood smear, bone marrow aspiration and biopsy, and molecular testing for JAK2 V617F, JAK2 exon 12, CALR, and MPL mutations. Serum erythropoietin helps separate polycythemia vera from secondary causes of a high red-cell count. Diagnosis is then matched against either the WHO 5th edition (2022) or the International Consensus Classification (2022) criteria.
Can a myeloproliferative neoplasm be cured?
For most patients, MPNs are managed as long-term conditions rather than cured. The only potentially curative treatment is allogeneic stem cell transplantation, which is generally reserved for younger patients with high-risk myelofibrosis because of its serious risks. Modern therapies aim to reduce thrombosis, control symptoms, and slow progression.
What are the newest treatments for MPNs?
Two recent additions stand out. Ropeginterferon alfa-2b (Besremi) is now an NCCN-preferred first-line cytoreductive option for polycythemia vera regardless of risk category. Momelotinib (Ojjaara), approved by the FDA in September 2023, is a JAK1/JAK2/ACVR1 inhibitor designed for intermediate- or high-risk myelofibrosis in patients who also have anemia. Ruxolitinib, fedratinib, and pacritinib remain established JAK inhibitor options.
What is the risk that an MPN turns into acute leukemia?
The risk of transformation to acute myeloid leukemia varies by subtype. Essential thrombocythemia carries the lowest lifetime risk (around 1–5%), polycythemia vera is intermediate (around 5–10%), and primary myelofibrosis carries the highest risk (up to 10–20% over 10 years). High-molecular-risk mutations such as ASXL1, SRSF2, EZH2, and IDH1/2 increase that risk further.
Are myeloproliferative neoplasms inherited?
The mutations that cause most MPNs (JAK2, CALR, MPL) are usually acquired during life, not inherited. There is, however, a small familial predisposition: having a first-degree relative with an MPN raises baseline risk by roughly five- to seven-fold, although the absolute risk remains low. Targeted genetic counseling is reasonable when several relatives are affected.
Glossary of Related Medical Terms
- Myeloproliferative neoplasm (MPN): A group of chronic blood cancers in which the bone marrow makes too many of one or more types of mature blood cell.
- Hematopoietic stem cell (HSC): The bone-marrow stem cell from which all blood cells originate.
- JAK-STAT pathway: A signaling system that carries growth and survival signals from outside a cell to its nucleus. Mutations that lock it "on" drive most MPNs.
- JAK2 V617F: The single most common MPN mutation. A swap of the amino acid valine for phenylalanine at position 617 in the JAK2 gene that keeps the protein active without an external signal.
- Triple-negative MPN: An MPN with no detectable JAK2, CALR, or MPL mutation. Often carries non-canonical drivers found on next-generation sequencing.
- Constitutive activation: Unregulated, constant "on" state of a protein or pathway, even without a signal telling it to switch on.
- Megakaryocyte: Large bone-marrow cell that buds off platelets.
- Erythromelalgia: Burning pain, redness, and warmth in fingers or toes caused by platelet clumping in small vessels.
- Aquagenic pruritus: Intense itching after contact with water (often warm) — a hallmark symptom of polycythemia vera.
- Splenomegaly: Enlargement of the spleen.
- Extramedullary hematopoiesis: Blood-cell production outside the bone marrow, usually in the spleen or liver. A common compensation in primary myelofibrosis.
- Phlebotomy: Therapeutic removal of blood to lower red-cell mass; standard care in polycythemia vera.
- Leukoerythroblastosis: A blood smear pattern showing immature white cells and nucleated red cells — typical of marrow stress in PMF.
- Hepcidin: The master hormone of iron metabolism. High hepcidin traps iron away from red-cell production and contributes to anemia in myelofibrosis.
- MPN-SAF TSS: The MPN Symptom Assessment Form Total Symptom Score — a validated 10-item tool to track symptom burden over time.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850.
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Tefferi, A., & Pardanani, A. (2015). Myeloproliferative Neoplasms: A Contemporary Review. JAMA oncology, 1(1), 97–105. https://doi.org/10.1001/jamaoncol.2015.89
- Rumi, E., & Cazzola, M. (2017). Diagnosis, risk stratification, and response evaluation in classical myeloproliferative neoplasms. Blood, 129(6), 680–692. https://doi.org/10.1182/blood-2016-10-695957
- Mahmud, M., Vasireddy, S., Gowin, K., & Amaraneni, A. (2023). Myeloproliferative Neoplasms: Contemporary Review and Molecular Landscape. International journal of molecular sciences, 24(24), 17383. https://doi.org/10.3390/ijms242417383
- Gianelli, U., Thiele, J., Orazi, A., Gangat, N., Vannucchi, A. M., Tefferi, A., & Kvasnicka, H. M. (2023). International Consensus Classification of myeloid and lymphoid neoplasms: myeloproliferative neoplasms. Virchows Archiv : an international journal of pathology, 482(1), 53–68. https://doi.org/10.1007/s00428-022-03480-8
- Gerds, A. T., Verstovsek, S., Vannucchi, A. M., Al-Ali, H. K., Lavie, D., Kuykendall, A. T., Grosicki, S., Iurlo, A., Goh, Y. T., Lazaroiu, M. C., Egyed, M., Fox, M. L., McLornan, D., Perkins, A., Yoon, S. S., Gupta, V., Kiladjian, J. J., Granacher, N., Lee, S. E., Ocroteala, L., … Mesa, R. (2023). Momelotinib versus danazol in symptomatic patients with anaemia and myelofibrosis previously treated with a JAK inhibitor (MOMENTUM): an updated analysis of an international, double-blind, randomised phase 3 study. The Lancet. Haematology, 10(9), e735–e746. https://doi.org/10.1016/S2352-3026(23)00174-6
- Gisslinger, H., Klade, C., Georgiev, P., Krochmalczyk, D., Gercheva-Kyuchukova, L., Egyed, M., Rossiev, V., Dulicek, P., Illes, A., Pylypenko, H., Sivcheva, L., Mayer, J., Yablokova, V., Krejcy, K., Grohmann-Izay, B., Hasselbalch, H. C., Kralovics, R., Kiladjian, J. J., & PROUD-PV Study Group (2020). Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study. The Lancet. Haematology, 7(3), e196–e208. https://doi.org/10.1016/S2352-3026(19)30236-4
- Barbui, T., Ghirardi, A., Carobbio, A., De Stefano, V., Rambaldi, A., Tefferi, A., & Vannucchi, A. M. (2024). Thrombosis in myeloproliferative neoplasms: a viewpoint on its impact on myelofibrosis, mortality, and solid tumors. Blood cancer journal, 14(1), 188. https://doi.org/10.1038/s41408-024-01169-6
- Tefferi, A., Guglielmelli, P., Lasho, T. L., Gangat, N., Ketterling, R. P., Pardanani, A., & Vannucchi, A. M. (2018). MIPSS70+ Version 2.0: Mutation and Karyotype-Enhanced International Prognostic Scoring System for Primary Myelofibrosis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 36(17), 1769–1770. https://doi.org/10.1200/JCO.2018.78.9867
- National Comprehensive Cancer Network. (2026). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Myeloproliferative Neoplasms, Version 2.2026. Retrieved from https://www.nccn.org
- Kremyanskaya, M., Kuykendall, A. T., Pemmaraju, N., Ritchie, E. K., Gotlib, J., Gerds, A., Palmer, J., Pettit, K., Nath, U. K., Yacoub, A., Molina, A., Saks, S. R., Modi, N. B., Valone, F. H., Khanna, S., Gupta, S., Verstovsek, S., Ginzburg, Y. Z., Hoffman, R., & REVIVE Trial Investigators (2024). Rusfertide, a Hepcidin Mimetic, for Control of Erythrocytosis in Polycythemia Vera. The New England journal of medicine, 390(8), 723–735. https://doi.org/10.1056/NEJMoa2308809
- Jakafi.com (2026). Jakafi XR (ruxolitinib extended-release tablets) Prescribing Information. Wilmington, DE.
- Mesa, R., Gill, H., Zhang, L., Jin, J., Kirito, K., Komatsu, N., Qin, A., Xiao, Z., Tashi, T., Shimoda, K., Ohishi, K., Chen, S., Zuo, X., Shirane, S., Hu, Y., Zhang, S., Wang, Y., Takenaka, K., Ichii, M., Xu, N., … SURPASS-ET Study Group (2025). Ropeginterferon alfa-2b in hydroxyurea-intolerant or hydroxyurea-refractory essential thrombocythaemia (SURPASS ET): a multicentre, open-label, randomised, active-controlled, phase 3 study. The Lancet. Haematology, 12(11), e862–e875. https://doi.org/10.1016/S2352-3026(25)00264-9
- Gupta, V., et al. (2025). Safety and efficacy of INCA033989, a novel first in class mutant calreticulin-specific monoclonal antibody, in patients with essential thrombocythemia. Blood (ASH Annual Meeting Abstracts).146 (Supplement 1): 1024. https://doi.org/10.1182/blood-2025-1024