Key Takeaways
Essential thrombocythemia is a chronic blood cancer (specifically a myeloproliferative neoplasm) in which the bone marrow produces too many platelets, raising the risk of both clots and bleeding [1].
- Pathogenesis ▾:Primarily driven by mutations in JAK2, CALR, or MPL genes, disrupting the JAK-STAT pathway and promoting uncontrolled megakaryocyte (platelet precursor) growth [1,4].
- Symptoms ▾: Often asymptomatic, detected incidentally during routine blood tests.
- Diagnosis ▾: Diagnosis combines a persistent platelet count of ≥450 × 10⁹/L, bone-marrow biopsy findings, mutation testing, and exclusion of reactive or other clonal causes [2,3].
- Treatment ▾: Treatment in essential thrombocythemia is risk-stratified using the IPSET-thrombosis score: from observation alone in very-low-risk cases to cytoreductive therapy plus aspirin in high-risk cases [1].
*Click ▾ for more information
What is Essential Thrombocythemia (ET)?
Essential thrombocythemia (ET) is a chronic blood cancer in which the bone marrow makes too many platelets, the small cell fragments that plug damaged blood vessels and start the clotting process. The extra platelets are often abnormal in shape and function, which paradoxically causes both clotting and bleeding problems [1,4].
ET belongs to a family of diseases called myeloproliferative neoplasms (MPNs). In MPNs, an abnormal stem cell in the bone marrow drives uncontrolled production of one or more blood cell types. In essential thrombocythemia, the affected cell line is the megakaryocyte, the large bone-marrow cell that releases platelets [1].
Although ET is technically a cancer, its course is usually slow. With proper treatment most people live near-normal lifespans [1].
Pathogenesis and Pathophysiology

The JAK-STAT pathway
Think of the JAK-STAT pathway as a cellular intercom. Outside the cell, a signal (such as the hormone thrombopoietin) presses the buzzer. Inside, an enzyme called JAK (Janus kinase) answers and passes the message on to STAT (Signal Transducer and Activator of Transcription), which travels to the nucleus and tells the cell to grow and divide.
In essential thrombocythemia, that intercom is jammed in the "on" position. The cell keeps hearing "grow and divide" even when nothing is calling [1,4].
The three driver mutations
Roughly 90% of patients carry one of three mutations [1]:
- JAK2 V617F (about 50–60% of cases). A point mutation in the pseudokinase domain of JAK2 disables its self-braking function, leaving JAK2 constitutively active.
- CALR (calreticulin) mutations (about 20–25%). Mutant calreticulin binds the MPL receptor and activates it without needing thrombopoietin. Type 1 and Type 2 CALR mutations differ slightly in clinical behavior, with Type 1 carrying a higher risk of progression to myelofibrosis [6].
- MPL mutations (about 3–5%). MPL encodes the thrombopoietin receptor itself. Mutations like W515L cause the receptor to dimerize and signal on its own.
The remaining 10–15% are triple-negative ET. The driver in these patients is unclear, and additional gene testing (ASXL1, EZH2, TET2, IDH1/2, SRSF2, SF3B1) can sometimes reveal a clonal mutation that supports the diagnosis [1,2].

Why platelets misbehave
The mutations skew bone-marrow output toward megakaryocytes, so platelet production rises. Newer research also shows that red blood cells in essential thrombocythemia are stickier and more likely to bind vessel walls, contributing to thrombosis risk on top of the platelet effect [8].
Epidemiology and Risk Factors
ET is uncommon. Annual incidence is roughly 0.2 to 2.5 cases per 100,000 people, and prevalence sits at about 38 to 57 per 100,000 [1].
A few demographic patterns are worth knowing:
- Age. Most patients are diagnosed between 50 and 60 years, but ET can occur in children. Pediatric ET is genuinely different: more often triple-negative and frequently managed without cytoreduction [9].
- Sex. Women outnumber men roughly 2:1, especially in older age groups.
- Family history. Around 90% of cases are sporadic. A small minority (under 10%) have familial ET driven by germline predisposition; even then, most relatives never develop disease.
Essential Thrombocythemia (ET) Symptoms
Many patients have no symptoms. The diagnosis often surfaces incidentally on a routine blood test. When symptoms do occur, they fall into three groups: clotting-related, bleeding-related, and general.
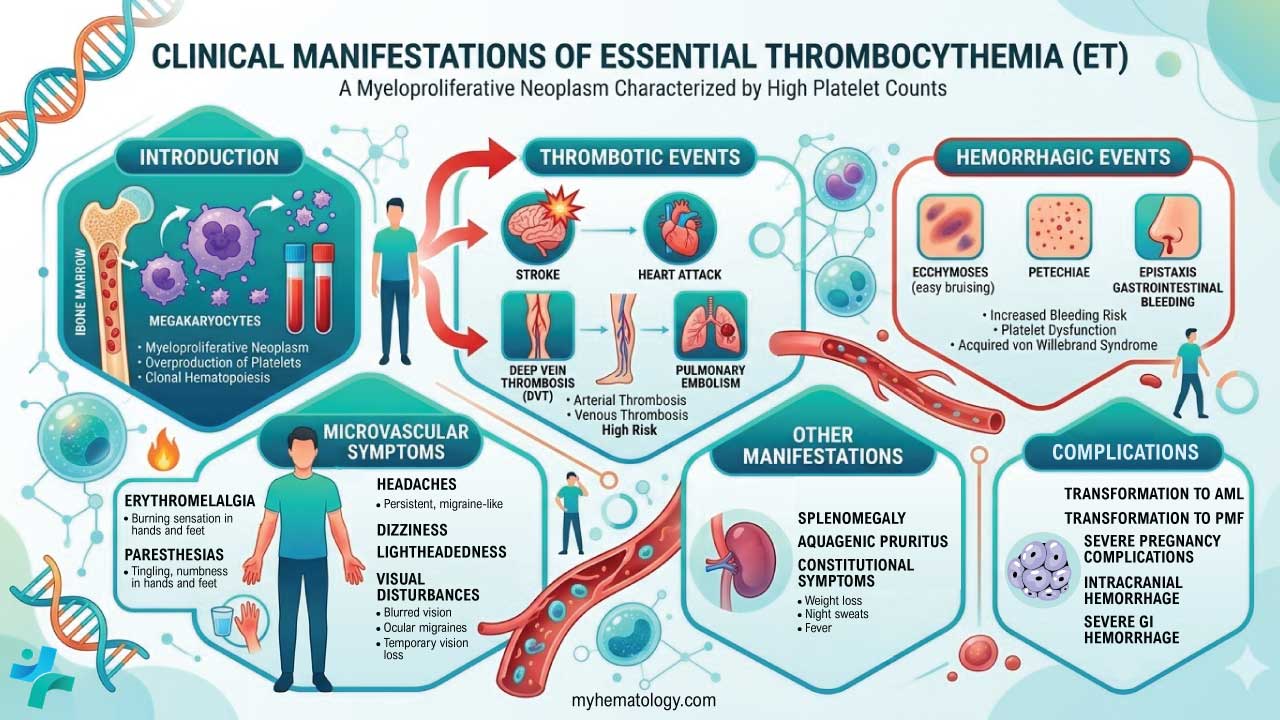
Clot-related symptoms
The extra platelets make blood "stickier." Where the clot forms determines what the patient feels.
Small-vessel symptoms
- Erythromelalgia — burning, throbbing, red, hot hands or feet, often relieved by cooling. This is one of the most characteristic ET symptoms.
- Headaches, sometimes migraine-like.
- Dizziness or lightheadedness.
- Visual disturbances such as transient blurring or "light shows."
- Tingling or numbness in fingers and toes (paresthesias).
Large-vessel events are more serious and include stroke, transient ischemic attack (TIA), heart attack, deep vein thrombosis (DVT), pulmonary embolism, and abdominal-vein thromboses such as Budd-Chiari syndrome [1].
Bleeding symptoms
Bleeding seems counterintuitive given the high platelet count, but the platelets in ET often function poorly. At very high counts (typically above 1,000–1,500 × 10⁹/L), platelets also consume large von Willebrand factor multimers, producing acquired von Willebrand syndrome (aVWS) [1]. Bleeding shows up as easy bruising, frequent nosebleeds, gum bleeding, gastrointestinal bleeding, heavy periods, and rarely blood in the urine.
General symptoms
These reflect chronic systemic inflammation: fatigue (often the most disabling symptom), night sweats, low-grade fever, unexplained weight loss, splenomegaly (which can cause early fullness), and itching after a warm shower (aquagenic pruritus). The validated MPN-SAF Total Symptom Score is increasingly used to track these symptoms over time [1].
Complications
Most complications of essential thrombocythemia stem from clots, bleeding, or rarely disease progression [1]:
- Major arterial thrombosis can cause disabling stroke, large myocardial infarction, or limb ischemia.
- Major venous thrombosis includes massive pulmonary embolism and Budd-Chiari syndrome.
- Transformation to primary myelofibrosis affects roughly 1% of patients per year, with a 15-year cumulative risk closer to 10–15% [1,4].
- Transformation to acute myeloid leukemia (AML) affects fewer than 1% per year but carries a poor prognosis when it occurs.
- Pregnancy complications include miscarriage, pre-eclampsia, intrauterine growth restriction, and stillbirth.
- Intracranial or severe gastrointestinal hemorrhage is rare but life-threatening.
Laboratory Investigations and Diagnosis
Confirming ET means proving clonal thrombocytosis and excluding mimics, especially pre-fibrotic primary myelofibrosis (pre-PMF).
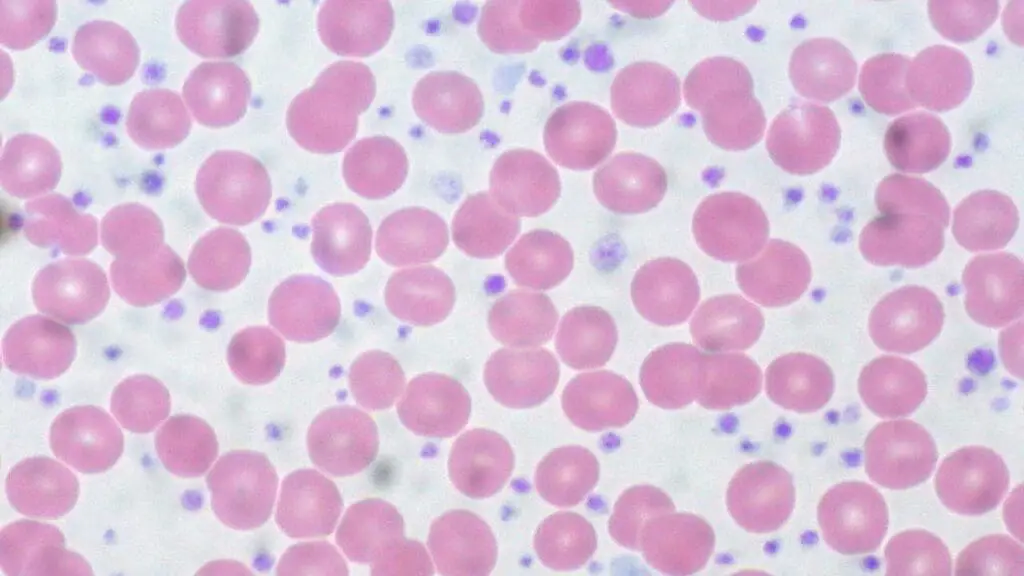
Peripheral blood
The starting point is a complete blood count (CBC) and a peripheral blood smear:
- Platelet count ≥450 × 10⁹/L, persistent for at least 3–6 months.
- Hemoglobin and white cell count are usually normal. A high hemoglobin points toward polycythemia vera. A high neutrophil count raises suspicion for pre-PMF.
- Smear shows numerous platelets with significant size variation (anisocytosis), often including giant platelets. Teardrop cells or immature precursors should not be present in true ET.
Bone marrow biopsy
A bone marrow aspirate and trephine biopsy is mandatory. The classic findings are [1,2]:
- Normal or mildly increased cellularity for age.
- A proliferation of large, mature megakaryocytes with hyperlobulated, "staghorn-like" nuclei, scattered or in loose groups.
- Reticulin fibrosis grade 0 or 1. Grade 2 or higher suggests pre-PMF or post-ET myelofibrosis.

Molecular testing
Mutation testing for JAK2, CALR, and MPL is now central to diagnosis. While identifying these driver mutations is a requirement, the 2026 National Comprehensive Cancer Network (NCCN) guidelines heavily emphasize broader multigene Next-Generation Sequencing (NGS) [14]. Identifying additional 'high-risk' non-driver mutations (such as ASXL1, SRSF2, or TP53) helps doctors predict disease progression and highly individualize the patient's long-term treatment plan. BCR-ABL1 must also always be tested to rule out chronic myeloid leukemia (CML), which can present with isolated thrombocytosis [1,2].
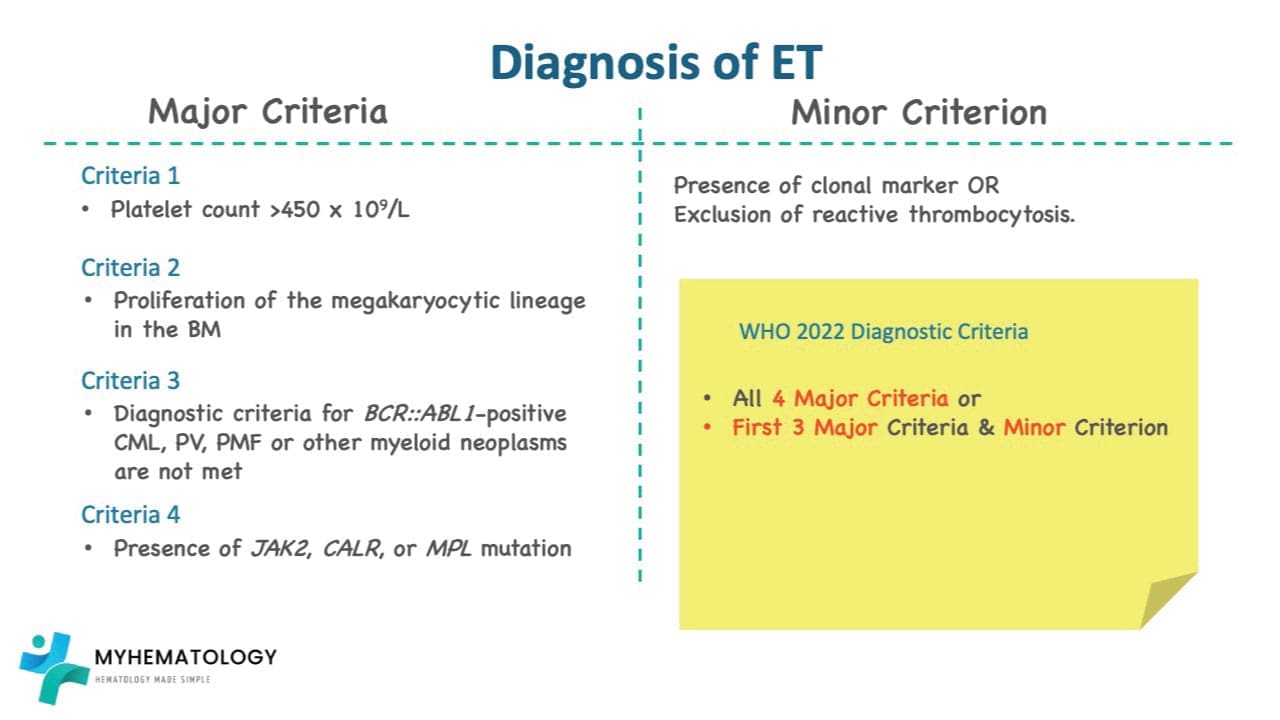
Diagnostic criteria
ET is currently defined by two parallel classifications published in 2022: the WHO 5th edition [3] and the International Consensus Classification (ICC) [2]. They overlap heavily. Both require all four major criteria, or the first three majors plus a minor criterion:
| Type | Criterion |
|---|---|
| Major 1 | Platelet count ≥450 × 10⁹/L |
| Major 2 | Bone-marrow biopsy showing large/mature megakaryocytes with hyperlobulated nuclei; no significant granulocytic or erythroid expansion; reticulin grade ≤1 |
| Major 3 | Does not meet criteria for BCR-ABL1+ CML, polycythemia vera, primary myelofibrosis, MDS, or other myeloid neoplasms |
| Major 4 | Presence of a JAK2, CALR, or MPL mutation |
| Minor | A clonal marker (e.g., from NGS) or absence of evidence for reactive thrombocytosis |
Excluding reactive causes
Because reactive thrombocytosis is far more common than essential thrombocythemia, baseline workup also includes iron studies, inflammatory markers (CRP, ESR), lactate dehydrogenase, and uric acid [1].
Differential Diagnosis of Thrombocytosis
About 80–90% of high platelet counts have a non-malignant explanation [1]. The main categories are:
Reactive thrombocytosis — driven by infection, inflammation (rheumatoid arthritis, lupus), tissue injury or surgery, blood loss or iron deficiency, certain medications (erythropoietin, corticosteroids), and post-splenectomy states.
Other myeloproliferative neoplasms — chronic myeloid leukemia, polycythemia vera, primary myelofibrosis. Each has distinguishing features, especially BCR-ABL1 in CML and elevated red cell mass in PV.
Spurious thrombocytosis — laboratory artifact from cryoglobulins, microcytic red cell fragments, or bacterial debris counted as platelets.
Pre-fibrotic primary myelofibrosis (pre-PMF) — the trickiest mimic and arguably the most important one to recognize. Both share elevated platelet counts and the same driver mutations, but their bone-marrow features and prognoses differ significantly.
Essential Thrombocythemia (ET) Treatment and Management
Essential thrombocythemia is a chronic disease, and the treatment goal is prevention rather than cure. Allogeneic stem cell transplant is the only curative option but is reserved for transformation to myelofibrosis or AML, not for ET itself [1].
Risk stratification: the revised IPSET-thrombosis score
Treatment hinges on thrombotic risk. The revised IPSET-thrombosis model assigns points for [1]:
The score then sorts patients into four tiers:
Essential Thrombocythemia
Antiplatelet therapy
Low-dose aspirin (75–100 mg daily) prevents microvascular symptoms such as erythromelalgia and many arterial events. Twice-daily aspirin is increasingly favored in JAK2-positive patients and in CALR-mutated patients with arterial events, because rapid platelet turnover blunts a single daily dose [5].
There is one big caveat. In extreme thrombocytosis (platelets above 1,000–1,500 × 10⁹/L), aspirin may worsen bleeding caused by acquired von Willebrand syndrome. A ristocetin cofactor assay and von Willebrand factor antigen panel should be checked before starting aspirin in this setting [1].
Cytoreductive therapy
Cytoreduction lowers platelet (and often white-cell) counts. Three main agents are used [1,7,10]:
Hydroxyurea (HU) remains a long-established first-line option in high-risk patients, particularly those over 60. It is well tolerated but its effect is purely cytoreductive (it lowers counts but does not change the underlying genetics of the disease) [1].
Pegylated interferon-alfa (including ropeginterferon alfa-2b) is rapidly becoming the preferred first-line option for younger patients and those seeking a deep molecular response. Based on the highly successful SURPASS-ET and EXCEED-ET trials, the FDA accepted the supplemental Biologics License Application (sBLA) for ropeginterferon alfa-2b in ET with an expected action (PDUFA) date of August 30, 2026 [11]. This medication has been shown to meaningfully reduce the JAK2 V617F mutant allele burden, meaning it can actively suppress the clone of cells causing the cancer [12]. It is also the only safe cytoreductive choice during pregnancy.
Anagrelide is strictly a second-line agent. It blocks megakaryocyte maturation, but the 2025 SURPASS-ET trial proved it is vastly inferior to ropeginterferon alfa-2b for maintaining durable responses (6.0% vs. 42.9%) [10]. It also carries a higher risk of progression to myelofibrosis and can cause cardiac side effects.
Anticoagulation
If a patient develops venous thromboembolism, low-molecular-weight heparin or a direct oral anticoagulant (DOAC) is started, usually with cytoreduction added to lower the underlying thrombotic drive. DOAC use in MPN-related thrombosis, including splanchnic vein thrombosis, is supported by retrospective evidence and is now common practice [1].
JAK inhibitors
Ruxolitinib is approved for myelofibrosis and polycythemia vera. In essential thrombocythemia it is used off-label or in trials for hydroxyurea-resistant patients with severe constitutional symptoms or splenomegaly. It controls symptoms well; whether it changes long-term disease trajectory in ET is still being studied [1].
Beyond JAK Inhibitors: LSD1 Inhibitors
While JAK inhibitors like ruxolitinib are primarily used to manage severe symptoms and spleen enlargement, a new class of medications called LSD1 inhibitors is poised to change how ET is treated. The leading investigational drug, bomedemstat, targets an enzyme crucial for platelet production. In July 2026, bomedemstat successfully completed enrollment for its pivotal global Phase 3 clinical trial (MK-3543-007) testing it directly against hydroxyurea in newly diagnosed patients [13]. If successful, it could offer a highly targeted, disease-modifying alternative to traditional chemotherapy.
Pregnancy with essential thrombocythemia
Pregnancy in ET is high-risk but usually successful with a coordinated hematology and maternal-fetal medicine plan [1].
Pre-conception: stop hydroxyurea and anagrelide at least 3–6 months before trying to conceive. Optimize blood pressure and stop smoking.
During pregnancy: all patients receive low-dose aspirin (unless aVWS contraindicates it). High-risk patients (prior thrombosis, prior pregnancy complications) add LMWH and, if cytoreduction is needed, pegylated interferon. Interferon is the only cytoreductive agent considered safe in pregnancy because it does not cross the placenta.
Around delivery: stop aspirin around 7 days before elective induction or C-section; pause LMWH 12–24 hours before delivery to allow neuraxial anesthesia.
Postpartum: the 6–12 weeks after delivery are the highest-risk period for thrombosis. Restart LMWH 6–12 hours after delivery and continue at least 6 weeks. Hydroxyurea and anagrelide are avoided during breastfeeding; interferon remains compatible.
Living with Essential Thrombocythemia
Beyond medication, daily choices matter. Patients should know to:
- Treat cardiovascular risk factors aggressively. Stop smoking, control blood pressure, manage cholesterol and diabetes.
- Consider an anti-inflammatory eating pattern (the Mediterranean diet has the best evidence for chronic inflammatory conditions).
- Recognize red-flag symptoms that require urgent assessment: sudden severe headache, one-sided weakness or numbness, slurred speech, sudden vision loss, calf swelling and pain, sudden chest pain or shortness of breath, severe abdominal pain, or any unusual bleeding.
- Attend regular hematology follow-up. Even patients on observation alone need periodic blood counts and symptom checks.
Prognosis
With proper management most people with essential thrombocythemia live close to a normal lifespan. Median survival is around 18 years overall and exceeds 26 years in low-risk patients [1,4]. Outcomes are influenced by mutation type (CALR Type 1 carries a higher MF risk; JAK2 carries a higher thrombotic risk), age at diagnosis, and additional non-driver mutations such as ASXL1 and TP53 [6].
Regular follow-up is essential not just for adjusting medication but for catching the rare but important transformations to myelofibrosis or acute leukemia early.
Frequently Asked Questions (FAQs)
Is essential thrombocythemia serious?
Essential thrombocythemia is technically a cancer, but with proper management it is generally not life-shortening. Most patients live close to a normal lifespan, with median survival around 18 years and longer in low-risk groups. The main risks are blood clots and, less commonly, bleeding, both of which are reduced by treatment.
Can essential thrombocytosis be cured?
No. Essential thrombocythemia is a chronic clonal disease driven by acquired mutations. Allogeneic stem cell transplant is theoretically curative but is too risky for ET itself; it is reserved for cases that progress to myelofibrosis or acute leukemia. Treatments instead aim to prevent complications and control symptoms.
Is essential thrombocythemia a form of leukemia?
No. Essential thrombocythemia is a myeloproliferative neoplasm, a sister category to leukemia in the broader family of blood cancers. Leukemia involves overproduction of abnormal white blood cells; in essential thrombocythemia the affected line is megakaryocytes, which produce platelets. Transformation to acute myeloid leukemia is possible but rare (under 1% per year).
Why does essential thrombocythemia cause bleeding when platelets are high?
Bleeding in essential thrombocythemia happens because the extra platelets are often dysfunctional. They may have abnormal granules, poor activation responses, and reduced ability to aggregate. At very high counts, platelets also consume von Willebrand factor multimers and produce acquired von Willebrand syndrome, which impairs platelet adhesion to the vessel wall. Aspirin therapy can compound the bleeding tendency, which is why von Willebrand testing is important before starting aspirin in extreme thrombocytosis.
Why does essential thrombocythemia cause fatigue?
Fatigue is one of the most common and disabling symptoms of essential thrombocythemia. It comes from several sources: chronic systemic inflammation driven by abnormal cytokine release, mild anemia in some patients, splenomegaly, microcirculatory disturbances, the psychological weight of a chronic cancer diagnosis, and side effects of medications. Validated tools such as the MPN Symptom Assessment Form (MPN-SAF TSS) help clinicians track and manage it.
Is essential thrombocythemia hereditary?
In most cases, essential thrombocythemia (ET) is not considered hereditary. It arises from acquired genetic mutations that In about 90% of cases, no. The mutations occur in bone-marrow cells after birth and are not inherited. A minority (under 10%) represents familial essential thrombocythemia, where a germline predisposition is passed down. Even within these families, most relatives never develop the disease, and routine genetic screening of family members is not standard.
Can someone with essential thrombocythemia donate blood?
Generally, no. The platelets in essential thrombocythemia are often functionally abnormal, which raises concerns about clot quality in the recipient, and donation could perturb the donor's own counts. Most blood services exclude individuals with diagnosed myeloproliferative neoplasms, including essential thrombocythemia.
What is the difference between essential thrombocythemia and polycythemia vera?
Both are myeloproliferative neoplasms, but they affect different cell lines. Polycythemia vera is dominated by red-cell overproduction and is almost always JAK2-mutated. Essential thrombocythemia primarily involves overproduction of platelets and can be driven by JAK2, CALR, or MPL mutations. The two diseases can also evolve into each other in a small number of patients.
What happens if hydroxyurea stops working?
Patients who become resistant or intolerant to hydroxyurea are switched to second-line therapy. Pegylated interferon, especially ropeginterferon alfa-2b, is now well supported by recent phase 3 evidence (SURPASS-ET, 2025) showing it outperforms anagrelide in this setting [10]. Anagrelide and clinical-trial options remain available, and patients with severe symptoms may try ruxolitinib off-label.
Are there diet or lifestyle recommendations for essential thrombocythemia?
There is no diet that cures essential thrombocythemia, but an anti-inflammatory pattern most often the Mediterranean diet is reasonable given the inflammatory biology of MPNs. The biggest lifestyle wins are tightly managing cardiovascular risk factors: stopping smoking, controlling blood pressure, treating diabetes, and addressing cholesterol. These compound with treatment to reduce thrombotic risk.
Glossary of Related Medical Terms
- Acquired von Willebrand syndrome (aVWS): Bleeding disorder where excess platelets bind and remove von Willebrand factor from circulation.
- Cytoreductive therapy: Medications that lower the bone marrow's output of blood cells. Hydroxyurea and pegylated interferon are the main agents in essential thrombocythemia.
- Erythromelalgia: Burning, red, hot pain in hands or feet caused by microvascular platelet thrombosis.
- JAK-STAT pathway: A cellular signaling system that controls blood-cell growth and is permanently switched on in essential thrombocythemia.
- Megakaryocyte: The large bone-marrow cell that releases platelets.
- Myeloproliferative neoplasm (MPN): A group of chronic blood cancers featuring overproduction of mature blood cells.
- Pre-fibrotic primary myelofibrosis (pre-PMF): An early form of myelofibrosis that mimics essential thrombocythemia but has different bone-marrow features and a worse prognosis.
- Reticulin fibrosis: Microscopic scarring in the bone marrow; graded 0 to 3.
- Thrombocythemia / thrombocytosis: A high platelet count. Thrombocythemia is the clonal disease; thrombocytosis is a broader term that also covers reactive causes.
- Thrombopoietin (TPO): Liver-made hormone that stimulates platelet production.
- Triple-negative ET: Essential thrombocythemia without a detectable JAK2, CALR, or MPL mutation.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Tefferi, A., Vannucchi, A. M., & Barbui, T. (2024). Essential thrombocythemia: 2024 update on diagnosis, risk stratification, and management. American journal of hematology, 99(4), 697–718. https://doi.org/10.1002/ajh.27216
- Gianelli, U., Thiele, J., Orazi, A., Gangat, N., Vannucchi, A. M., Tefferi, A., & Kvasnicka, H. M. (2023). International Consensus Classification of myeloid and lymphoid neoplasms: myeloproliferative neoplasms. Virchows Archiv : an international journal of pathology, 482(1), 53–68. https://doi.org/10.1007/s00428-022-03480-8
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Godfrey, A. L., Green, A. C., & Harrison, C. N. (2023). Essential thrombocythemia: challenges in clinical practice and future prospects. Blood, 141(16), 1943–1953. https://doi.org/10.1182/blood.2022017625
- Tefferi, A., & Barbui, T. (2024). Aspirin use in essential thrombocythemia: Once-daily or twice-daily or not at all?. American journal of hematology, 99(8), 1450–1453. https://doi.org/10.1002/ajh.27369
- Guglielmelli, P., Szuber, N., Gangat, N., Capecchi, G., Maccari, C., Harnois, M., Karrar, O., Abdelmagid, M., Balliu, M., Nacca, E., Atanasio, A., Sestini, I., Désilets, A., Loscocco, G. G., Rotunno, G., Busque, L., Tefferi, A., & Vannucchi, A. M. (2024). CALR mutation burden in essential thrombocythemia and disease outcome. Blood, 143(13), 1310–1314. https://doi.org/10.1182/blood.2023023428
- Kiladjian, J. J., Marin, F. F., Al-Ali, H. K., Alvarez-Larrán, A., Beggiato, E., Bieniaszewska, M., Breccia, M., Buxhofer-Ausch, V., Cerna, O., Crisan, A. M., Danaila, C. D., De Stefano, V., Döhner, K., Empson, V., Gora-Tybor, J., Griesshammer, M., Grosicki, S., Guglielmelli, P., García-Gutierrez, V., Heidel, F. H., … Klade, C. (2024). ROP-ET: a prospective phase III trial investigating the efficacy and safety of ropeginterferon alfa-2b in essential thrombocythemia patients with limited treatment options. Annals of hematology, 103(7), 2299–2310. https://doi.org/10.1007/s00277-024-05665-4
- Grenier, J. M. P., El Nemer, W., & De Grandis, M. (2024). Red Blood Cell Contribution to Thrombosis in Polycythemia Vera and Essential Thrombocythemia. International journal of molecular sciences, 25(3), 1417. https://doi.org/10.3390/ijms25031417
- Picard, A., Bayart, S., Deparis, M., De Maricourt, C. D., Haro, S., Jourdain, A., Mallebranche, C., Rialland, F., Luque Paz, D., Pastoret, C., Gandemer, V., & Cousin, E. (2025). Polycythemia vera and essential thrombocythemia in children, still a challenge for pediatricians. European journal of pediatrics, 184(2), 173. https://doi.org/10.1007/s00431-025-05993-1
- Mesa, R. A., Gill, H., Xiao, Z., et al. (2025). Ropeginterferon alfa-2b versus anagrelide for the treatment of essential thrombocythemia: Topline results of the phase 3 SURPASS-ET trial [Conference abstract]. Journal of Clinical Oncology, 43(16_suppl), Abstract 6500. http://dx.doi.org/10.1200/JCO.2025.43.16_suppl.6500
- https://www.targetedonc.com/view/ropeginterferon-alfa-s-supplemental-bla-moves-on-as-pdufa-date-issued
- https://www.onclive.com/view/fda-accepts-sbla-for-ropeginterferon-alfa-2b-for-essential-thrombocythemia
- https://clinicaltrials.gov/study/NCT06456346
- National Comprehensive Cancer Network (NCCN). (2026). NCCN Guidelines for Patients: Myeloproliferative Neoplasms (Version 1.2026). NCCN.org.


