Key Takeaways
Hodgkin Lymphoma or formerly known as Hodgkin's disease is a heterogeneous group of disorders caused by malignant lymphocytes presenting as lymphadenopathy and defined by Reed-Sternberg cells.
- Hodgkin lymphoma signs and symptoms ▾: The most common symptom is a painless, rubbery swelling of the lymph nodes, typically located in the neck, armpit, or groin. Patients may also experience "B symptoms" like unexplained fever, drenching night sweats, and significant weight loss, as well as severe itching or rare pain in the lymph nodes after drinking alcohol.
- Laboratory investigations ▾: Diagnosis relies on an excisional lymph node biopsy to identify the characteristic, large Reed-Sternberg cells under a microscope. Following diagnosis, a whole-body PET-CT scan is the standard imaging tool used to map the exact extent and metabolic activity of the disease.
- Clinical staging of Hodgkin Lymphoma (HL) ▾: HL is staged from I to IV using the Lugano classification, which evaluates the number of affected lymph node regions and whether they are located on one or both sides of the diaphragm. These stages are further modified by letters such as "A" (absence of B symptoms) or "B" (presence of B symptoms) to help determine the prognosis and treatment intensity.
- Treatment and management ▾: HL is highly curable and is primarily treated with chemotherapy regimens, increasingly combined with targeted immunotherapy drugs like nivolumab or brentuximab vedotin. Early-stage disease may also incorporate involved-site radiation therapy, while relapsed cases might require high-dose chemotherapy followed by a stem cell transplant.
*Click ▾ for more information
Introduction
Hodgkin's disease, more correctly called Hodgkin lymphoma, is a cancer of the lymphatic system. It is a malignancy of B lymphocytes that gather in lymph nodes and cause them to swell. About 1 in 10 lymphomas is a Hodgkin lymphoma; the rest fall under the umbrella of non-Hodgkin lymphoma.
Two features set Hodgkin's disease apart from the non-Hodgkin lymphomas. The first is the Reed-Sternberg cell, a large abnormal cell visible on lymph node biopsy. The second is its tendency to start in one lymph node group and spread to the next in an orderly, contiguous way. That orderly spread is why staging shapes treatment so strongly in Hodgkin lymphoma — more so than in most other cancers.
It is one of the most common cancers in young adults, and it is also one of the most curable. The 5-year survival is around 89% in the United States, and that figure has been climbing as treatment evolves [3].
What Are Reed-Sternberg Cells?
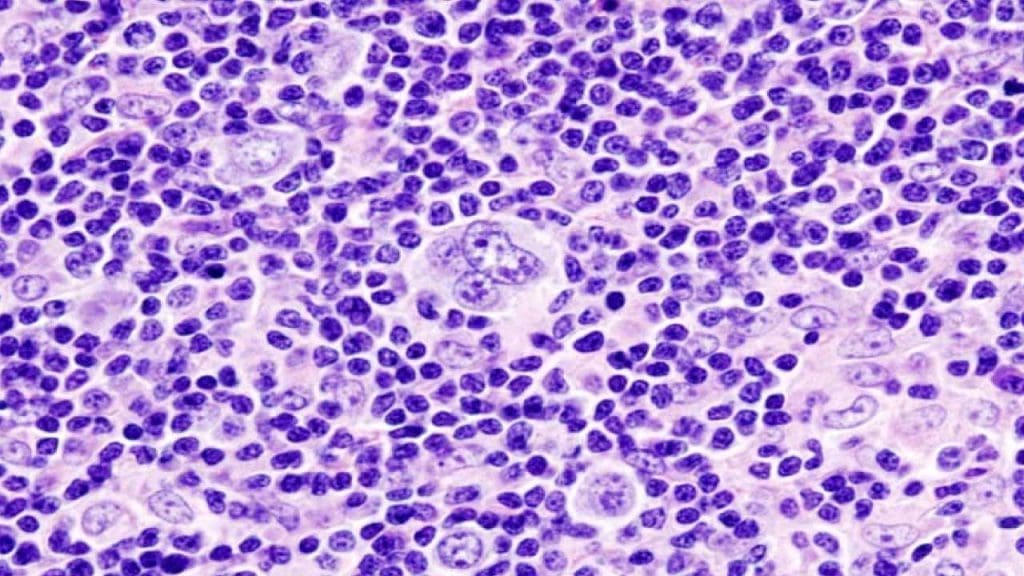
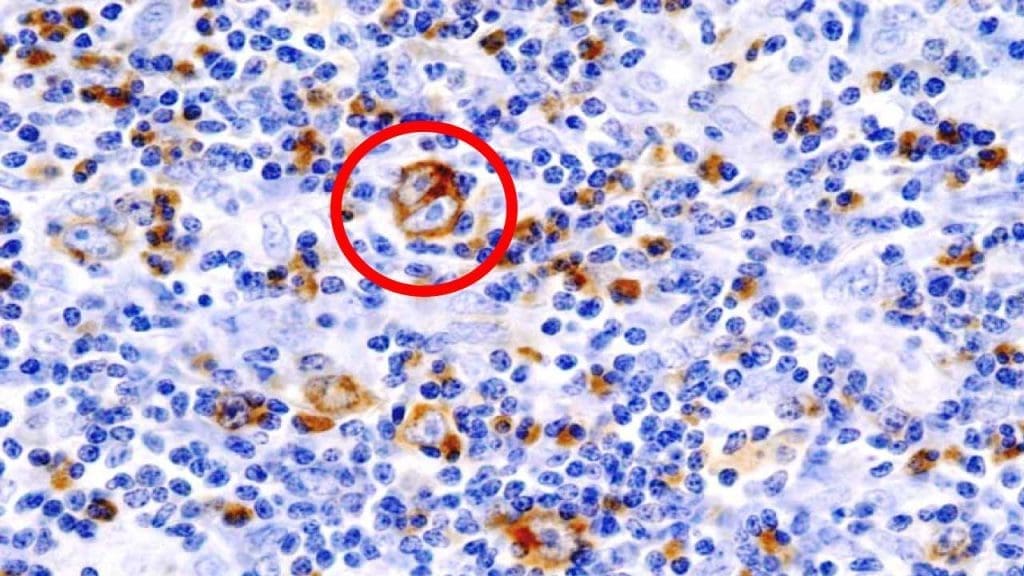
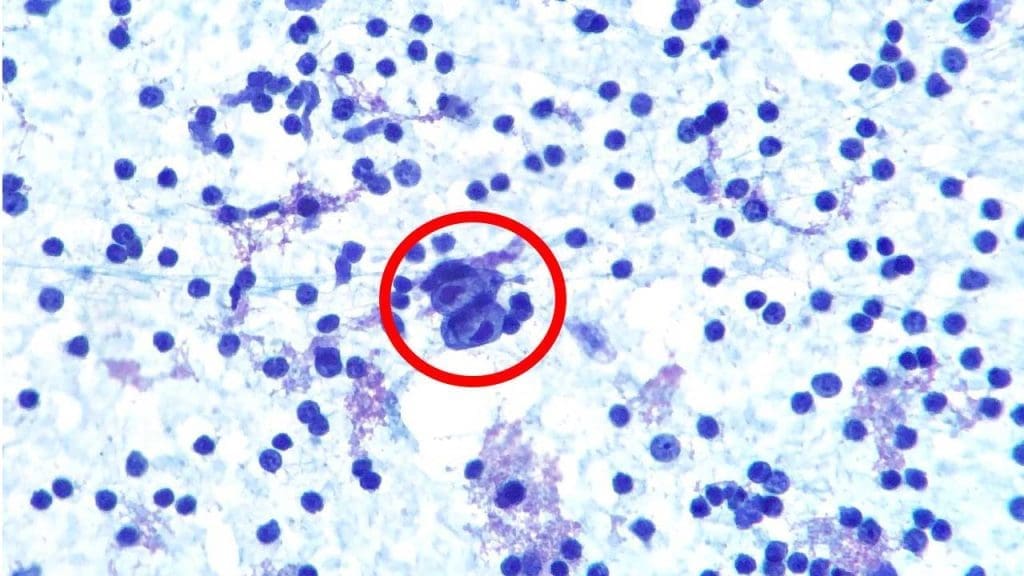
Reed-Sternberg (RS) cells are the diagnostic signature of classic Hodgkin lymphoma. They are large, abnormal cells with two or more prominent nuclei, often described as having an "owl-eye" appearance under the microscope. They derive from B lymphocytes (the antibody-producing white blood cells) but they have lost most of the features that make B cells recognizable as B cells.
The genetic story behind that transformation is unusual. RS cells carry mutations that destroy their ability to make a functional antibody, a state called a "crippled" immunoglobulin gene. Normally, a B cell that cannot produce a working antibody is told to die by apoptosis. RS cells escape that death sentence by activating survival signals — particularly the NF-κB and JAK-STAT pathways — and by displaying high levels of the immune checkpoint molecules PD-L1 and PD-L2, which let them hide from cytotoxic T cells [1]. This last point matters clinically: it explains why checkpoint inhibitors such as nivolumab and pembrolizumab are so effective in Hodgkin's disease.
RS cells also release cytokines that recruit a chaotic mix of inflammatory cells to the lymph node. So in a biopsy, the RS cells themselves are sparse (usually less than 1% of the cells in the field) and they sit inside a much larger crowd of reactive lymphocytes, eosinophils, plasma cells, and histiocytes. This is why an excisional biopsy (removing an entire node) is preferred over a needle biopsy: the pathologist needs both the rare RS cells and the surrounding architecture to make the diagnosis.

Hodgkin Lymphoma Subtypes
The World Health Organization divides Hodgkin lymphoma into two main families [1]:
- Classic Hodgkin lymphoma (cHL) — about 90% of cases.
- Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) — about 10% of cases.
The 2022 International Consensus Classification renamed NLPHL as nodular lymphocyte-predominant B-cell lymphoma (NLPBL), recognizing that it behaves more like an indolent B-cell non-Hodgkin lymphoma than classic Hodgkin lymphoma. The WHO 5th edition kept the older "NLPHL" name but accepts NLPBL as an alternative [1,2,8]. Either term is currently acceptable.
Classic Hodgkin Lymphoma
Classic Hodgkin's disease has four histological subtypes:

Nodular sclerosis is the most common form, especially in young adults. Two features define it. First are lacunar cells — variant RS cells whose cytoplasm shrinks during tissue fixation, leaving each cell sitting in an apparent empty space. Second are thick collagen bands deposited by reactive fibroblasts that divide the lymph node into nodules. EBV is rarely involved in this subtype.
Mixed cellularity Hodgkin lymphoma is most common in older men. The lymph node shows a busy mixture of inflammatory cells, plenty of RS cells, and an intermediate number of lymphocytes. About 70% of cases are EBV-positive.
Lymphocyte-rich Hodgkin lymphoma is uncommon. Small lymphocytes dominate the picture, with relatively few RS cells. Around 40% are linked to EBV.
Lymphocyte-depleted Hodgkin lymphoma is rare in immunocompetent people but more common in patients with HIV. RS cells dominate, lymphocytes are sparse, and EBV is almost always present.
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL/NLPBL)
NLPHL (now also known as NLPBL) is uncommon and tends to affect young to middle-aged men [8]. The cervical, axillary, and inguinal lymph nodes are most often involved, while mediastinal and abdominal nodes are characteristically spared. The defining cell is the popcorn cell, a variant RS cell with a lobulated nucleus that looks like a popped kernel of corn. Classic RS cells are rare or absent. Unlike classic HL, the tumor cells in NLPHL are CD20-positive and CD30/CD15-negative — the reason rituximab (an anti-CD20 antibody) plays a role in treatment.

Summary of Hodgkin Lymphoma Classifications
| Subtype | Key Characteristics | |
|---|---|---|
|
Classic Hodgkin Lymphoma (cHL)
|
||
|
Most Common Nodular Sclerosis |
Most common subtype in young adults; lacunar cells; collagen bandsEBV rare | |
| Mixed Cellularity | Older men; mixed inflammatory infiltrate with abundant Reed-Sternberg cells~70% EBV+ | |
| Lymphocyte-rich | Predominantly small lymphocytes; few Reed-Sternberg cells~40% EBV+ | |
|
Rare Lymphocyte-depleted |
Rare; enriched in HIV-positive patients; abundant Reed-Sternberg cellsAlmost always EBV+ | |
|
Distinct Entity NLPHL / NLPBL |
Uncommon; young to middle-aged men; "popcorn" (LP) cells; CD20-positive, CD30/CD15-negative; typically involves cervical, axillary, or inguinal nodes | |
Clinical Manifestations

The most common sign of Hodgkin's disease is a painless, asymmetrical, firm, and rubbery lymph node usually in the neck, sometimes in the underarm or groin. Cervical nodes are involved most often, followed by axillary and then inguinal nodes. About half of patients develop splenomegaly (an enlarged spleen) during their illness, though it is rarely massive.
Other common features include:
- Fever
- Pruritus (itching)
- Pain in affected lymph nodes after drinking alcohol — a rare but classic finding
- Fatigue
- Hypermetabolic symptoms: unintentional weight loss, drenching night sweats, anorexia, cachexia (severe muscle wasting)
A small subset of patients show Pel-Ebstein fever — a cyclical pattern of fevers lasting several days, then settling, then recurring. It is uncommon but iconic in clinical teaching.
The combination of unexplained fever above 38°C, drenching night sweats, and weight loss greater than 10% of body weight over 6 months is known formally as B symptoms. Their presence carries weight in staging and treatment decisions, as you'll see below.
Less common findings include bone pain, headaches, skin rashes, jaundice, and peripheral neuropathy.
Investigations & Diagnosis
Lymph Node Biopsy: The Gold Standard
An excisional biopsy (a surgical removal of an entire enlarged lymph node) is the preferred diagnostic test. As mentioned earlier, RS cells are sparse, and the pathologist needs both the cells and the surrounding inflammatory architecture to be sure. Core needle biopsy is sometimes used but can miss the diagnosis.
Once the tissue is in the lab, several techniques are applied:
Histopathology. The biopsy is stained with hematoxylin and eosin (H&E). The pathologist looks for RS cells with their characteristic owl-eye appearance, set within an inflammatory background.
Immunohistochemistry (IHC). Antibodies are used to detect specific proteins on the tumor cells. In classic Hodgkin's disease, RS cells are typically:
- CD30 positive
- CD15 positive
- CD20 negative or weakly positive
- CD45 negative
- PAX5 positive (often weakly)
- EBV-LMP1 sometimes positive, especially in mixed cellularity and lymphocyte-depleted subtypes
In NLPHL/NLPBL the pattern is essentially flipped: CD20 strongly positive, CD30 and CD15 negative.
Flow cytometry. While highly effective for diagnosing non-Hodgkin lymphomas, flow cytometry on lymph node aspirates is notoriously poor for diagnosing classic Hodgkin lymphoma. Reed-Sternberg cells are large, fragile, and too sparse (often <1% of the sample) to be reliably detected without being destroyed during sample processing. Therefore, a negative flow cytometry result does not rule out Hodgkin's disease, and IHC on the excisional biopsy remains the absolute workhorse.
Blood Tests
Blood tests cannot diagnose Hodgkin lymphoma on their own, but they help judge disease extent and prognosis:
- Complete blood count (CBC) with differential. May show normocytic normochromic anemia, lymphopenia, neutrophilia, or eosinophilia.
- ESR and CRP. Non-specific markers of inflammation, often raised, and a high ESR is associated with worse prognosis in some studies.
- LDH. Elevated levels reflect higher cell turnover and tumor burden.
- Liver and kidney function tests. Screen for organ involvement and inform treatment choices.
- Albumin. Low levels suggest worse prognosis.
- Beta-2 microglobulin. Elevated levels point to higher tumor burden.
- Viral serology (HIV, hepatitis B, hepatitis C). Important for treatment planning. EBV serology can support the diagnostic picture but is not itself diagnostic.
- Circulating tumor DNA (ctDNA). Although still largely in the realm of clinical trials and advanced treatment centers, measuring cell-free DNA (cfDNA) in the blood to detect the "crippled" immunoglobulin gene rearrangements or somatic mutations of RS cells is a rapidly emerging tool. It shows high promise as a complement to PET-CT for measuring minimal residual disease (MRD) and predicting relapse earlier than traditional imaging [9].
Investigations for Staging
PET-CT is the central staging tool. It combines functional imaging (PET, which detects metabolically active tissue) with anatomical imaging (CT). PET-CT identifies nodal and extranodal disease, including spleen, liver, and bone marrow involvement, and it is required for the Lugano classification [5].
Bone marrow biopsy is no longer routinely indicated for the vast majority of patients with classic Hodgkin lymphoma, regardless of stage, provided a high-quality PET-CT is performed. PET-CT has a high enough sensitivity for focal marrow lesions that invasive biopsies rarely change clinical management. Today, it is reserved almost exclusively for cases where PET-CT is unavailable or where the patient has unexplained cytopenias that are strongly discordant with the imaging findings [5,10].
Contrast-enhanced CT of the neck, chest, abdomen, and pelvis remains useful, particularly when PET-CT is unavailable.
Chest X-ray is largely historical; CT has replaced it for serious staging questions.
MRI has a limited role in initial staging, but is preferred in pregnancy (to avoid ionizing radiation) and for suspected spinal cord or brain involvement.
Hodgkin Lymphoma Staging
Staging in Hodgkin's disease answers two questions: where is the cancer, and how much of it is there? The current standard system is the Lugano classification, which is itself an evolution of the older Ann Arbor system and now incorporates PET-CT findings [5]. The Cotswolds-modified Ann Arbor system is still encountered in older literature and remains useful for teaching the underlying anatomical logic.
Lugano Classification
| Stage | Description |
|---|---|
| I | Single lymph node region or single lymphoid structure (e.g., spleen, thymus, Waldeyer's ring) |
| IE E | Single extralymphatic site without nodal involvement (rare in HL) |
| II | Two or more lymph node regions on the same side of the diaphragm |
| IIE E | Contiguous extralymphatic extension from a nodal site, on the same side of the diaphragm |
| III | Lymph node involvement on both sides of the diaphragm; may include the spleen |
| IIIE E | Involvement of lymph node regions on both sides of the diaphragm with localized extralymphatic involvement |
| IIIS S | Involvement of lymph node regions above the diaphragm with splenic involvement |
| IIIE+S E+S | Involvement of lymph node regions on both sides of the diaphragm with splenic and localized extralymphatic involvement |
| IV | Disseminated involvement of one or more extralymphatic organs (bone marrow, lung, liver), with or without nodal disease |
So a patient with disease confined to a single neck node and no B symptoms is stage IA; a patient with disease above and below the diaphragm with B symptoms is stage IIIB.
Risk Stratification: The International Prognostic Score (IPS)
For advanced-stage classic Hodgkin lymphoma, the International Prognostic Score is a useful tool. It counts seven adverse factors at diagnosis [7]:
- Albumin <40 g/L
- Hemoglobin <105 g/L
- Male sex
- Age ≥45 years
- Stage IV disease
- White cell count ≥15 × 10⁹/L
- Lymphocyte count <0.6 × 10⁹/L or <8% of the white cell count
More factors mean a worse prognosis. The IPS guides how intensive treatment should be in advanced-stage disease.
Treatment & Management
Treatment of Hodgkin's disease is one of the success stories of modern oncology. Most patients are cured. Care is delivered by a multidisciplinary team and combines chemotherapy, radiation therapy, immunotherapy, and for relapsed or refractory disease — high-dose chemotherapy with stem cell transplant. PET-CT guides decisions throughout.
Main Treatment Modalities
Chemotherapy is the backbone. The traditional regimen is ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine). For advanced-stage disease in many centers, AVD (the same regimen without bleomycin) is now used to spare patients from bleomycin-related lung injury, particularly when interim PET shows good response [6]. The newer N-AVD regimen (nivolumab plus AVD) has changed the field for advanced-stage classic Hodgkin lymphoma, and more on that below.
Radiation therapy is often combined with chemotherapy, especially for early-stage or bulky disease. Modern involved-site radiation therapy (ISRT) targets only the originally affected areas to reduce long-term side effects.
Immunotherapy. Checkpoint inhibitors (nivolumab and pembrolizumab) block PD-1 and reactivate the immune response against RS cells. Brentuximab vedotin is an antibody-drug conjugate that targets CD30, the protein heavily expressed on classic HL cells.
Stem cell transplant. Used mainly for relapsed or refractory disease. Autologous transplant (using the patient's own stem cells) is the standard; allogeneic transplant (using a donor's stem cells) is reserved for selected cases.
Surgery is mostly limited to obtaining biopsies. Splenectomy is rarely done now.
Bleomycin-induced lung injury
Bleomycin is effective but carries a real risk of pulmonary toxicity, which can be severe and sometimes fatal. The risk rises with cumulative dose, age over 40, smoking, and pre-existing lung disease. Patients on bleomycin should report new cough or breathlessness immediately. The shift toward bleomycin-free regimens such as AVD and N-AVD is driven largely by this concern.
Frontline Therapy: From ABVD to Nivolumab + AVD
For decades, ABVD was the global standard for classic Hodgkin lymphoma. That picture has changed.
The RATHL trial showed that patients with advanced-stage disease and a negative interim PET after two cycles of ABVD could safely drop bleomycin and continue with AVD, with no loss of efficacy and less lung toxicity [6]. This established the principle of PET-adapted therapy.
The SWOG S1826 trial compared nivolumab plus AVD (N-AVD) against brentuximab vedotin plus AVD (BV-AVD) in patients aged 12 and older with stage III or IV classic Hodgkin lymphoma [3]. At a median follow-up of 2.1 years, the 2-year progression-free survival was 92% with N-AVD compared with 83% with BV-AVD (a hazard ratio of 0.45). Updated 3-year follow-up confirmed the durability of the benefit. On the strength of these data, NCCN now lists N-AVD as a preferred frontline regimen for advanced-stage classic Hodgkin's disease, and the FDA has accepted this regimen for priority review in the first-line setting [3].
While the progression-free survival (PFS) of N-AVD is exceptional, physicians must weigh it against the primary alternative regimen: brentuximab vedotin plus AVD (BV-AVD). Long-term follow-up from the ECHELON-1 trial demonstrated that BV-AVD provides a proven, significant overall survival (OS) benefit compared to standard ABVD—a monumental achievement in a disease that is already highly curable [12]. Furthermore, the SWOG S1826 trial noted that N-AVD carries a higher risk of immune-related toxicities in patients over the age of 60. Therefore, the choice between N-AVD and BV-AVD in advanced disease remains highly individualized, balancing the patient's age and comorbidities with the prioritization of PFS versus established OS data.
Stage-Based Treatment (General Principles)
- Early-stage favorable risk (I–II). Traditionally, this is managed with a short chemotherapy course (typically 2 cycles of ABVD) followed by involved-site radiation therapy (ISRT). However, modern practice heavily emphasizes de-escalation to spare young patients from the late effects of radiation. Based on trials like RAPID and EORTC/LYSA H10, if a patient achieves a completely negative interim PET scan (Deauville 1–2) after 2 or 3 cycles of ABVD, radiotherapy can often be safely omitted entirely in favor of 1 to 2 additional cycles of chemotherapy [11].
- Early-stage unfavorable risk (I–II). More cycles of chemotherapy (4 cycles of ABVD or escalated regimens) followed by ISRT.
- Advanced-stage (III–IV). Six cycles of combination therapy. N-AVD is now a preferred option for adolescents and adults [3]. ABVD or escalated BEACOPP remain alternatives in specific contexts. Radiation may be added for residual bulky disease.
Response Assessment and Follow-Up
Interim PET-CT is performed after 2–4 cycles to score response on the Deauville 5-point scale. A good response (Deauville 1–3) often allows treatment to be de-escalated; a poor response may prompt intensification.
End-of-treatment PET-CT confirms complete remission.
Surveillance continues for years afterward. Routine scans are not recommended in patients with a clear end-of-treatment PET unless new symptoms arise. Long-term follow-up focuses on late effects rather than relapse alone, as you'll see in the survivorship section.
Relapsed or Refractory Disease
If Hodgkin's disease comes back or fails to respond, options include:
- Salvage chemotherapy (regimens such as ICE, DHAP, or ESHAP)
- High-dose chemotherapy with autologous stem cell transplant — the standard of care for chemosensitive relapse
- Allogeneic transplant — for selected patients who fail autologous transplant
- Brentuximab vedotin and checkpoint inhibitors (nivolumab, pembrolizumab) — highly active in this setting
- Clinical trials of novel agents
Special Populations
- Children and adolescents. Treatment is tailored to minimize long-term toxicity, especially to growing tissues.
- Pregnancy. Treatment balances fetal safety against maternal disease control and is adapted by trimester.
- Older adults. Comorbidities and tolerance of chemotherapy guide modified regimens.
- NLPHL / NLPBL. Often managed less aggressively than classic HL. Options include observation after complete excision of stage I disease, rituximab monotherapy, or limited radiation [8].
Survivorship: Living Well After Cure
Because most patients with Hodgkin lymphoma are cured, and many are cured young, survivorship is a major part of the curriculum. Long-term issues to monitor include:
- Cardiovascular disease — anthracyclines (the "A" in ABVD) and chest radiation increase the risk of cardiomyopathy and coronary disease decades later.
- Secondary cancers — particularly breast cancer in women treated with chest radiation under age 30, lung cancer in those who smoke after bleomycin or chest RT, and treatment-related leukemias.
- Thyroid dysfunction — common after neck or chest radiation; periodic TSH checks are standard [4].
- Infertility — fertility preservation (sperm banking, oocyte or embryo cryopreservation) should be discussed before chemotherapy starts in any patient of reproductive age.
- Pulmonary issues — late effects from bleomycin or chest radiation.
- Immune-related adverse events (irAEs) — With the integration of checkpoint inhibitors like nivolumab into frontline (N-AVD) and salvage therapies, long-term monitoring must now include surveillance for immune-related toxicities. These can manifest as late-onset autoimmune conditions, including checkpoint-induced hypothyroidism, pneumonitis, or colitis, requiring distinct management strategies separate from traditional chemotherapy toxicities [3,13].
A note for caregivers
During active treatment, the most important things to watch for at home are new or worsening cough, fever, shortness of breath, or signs of infection. These can emerge quickly and need urgent contact with the treating team. After treatment, the priority shifts to keeping survivorship clinic appointments — these visits catch late effects long before symptoms appear.
Hodgkin Lymphoma Prognosis
Hodgkin lymphoma is one of the most treatable cancers. Overall, the 5-year relative survival in the United States is around 89%, and the 10-year figure is about 80%. Stage drives the numbers most strongly:
- Early-stage disease — 5-year survival 93–95%
- Advanced-stage disease — 5-year survival around 83%
Other important factors include age (younger patients fare better), overall health, IPS in advanced disease, response to interim PET, and subtype. Patients whose disease responds quickly to chemotherapy — measured by an early negative PET — have especially favorable outcomes.
Frequently Asked Questions (FAQs)
What is the survival rate for Hodgkin lymphoma?
The 5-year relative survival in the United States is around 89%, and 10-year survival is approximately 80%. Early-stage disease has a 5-year survival of 93–95%, while advanced-stage disease is around 83%. Outcomes depend on stage, age, response to therapy, and subtype, and have continued to improve with newer regimens such as nivolumab plus AVD [3].
Who is most likely to get Hodgkin's disease?
Hodgkin lymphoma has a bimodal age distribution, with peaks in young adults aged 20–40 and in adults over 55–60. Men are slightly more affected than women overall, although nodular sclerosis classic HL is more common in young women. Risk is higher in people with weakened immune systems (HIV, autoimmune disease, transplant immunosuppression), in those with prior Epstein-Barr virus infection, and in close relatives of patients with the disease.
Is lymphoma a type of leukemia?
No. Both are blood cancers, but they differ in origin and presentation. Leukemia begins in the bone marrow and usually shows up in blood and marrow with abnormal counts. Lymphoma begins in the lymphatic system and usually shows up as enlarged lymph nodes or tumors in lymphoid organs. Hodgkin lymphoma and non-Hodgkin lymphoma are the two main families of lymphoma.
Is lymphoma benign or malignant?
"Lymphoma" is the name for a group of cancers of the lymphatic system, so by definition lymphomas are malignant. There are non-cancerous conditions of lymphoid tissue, such as Castleman disease and reactive lymphoid hyperplasia, that can mimic lymphoma clinically but these are not lymphomas in the strict sense.
What's the difference between Hodgkin's disease and Hodgkin lymphoma?
There is no difference. "Hodgkin's disease" was the original name, used from the time Thomas Hodgkin first described the condition in 1832. The cancer was renamed "Hodgkin lymphoma" because it is a malignancy of lymphocytes, the same family as non-Hodgkin lymphoma. Modern textbooks, guidelines, and clinical practice use "Hodgkin lymphoma," but the older term still appears in patient materials and casual conversation.
How is Hodgkin lymphoma different from non-Hodgkin lymphoma?
Two main features set it apart. First, Hodgkin lymphoma has Reed-Sternberg cells, which are large, abnormal B-cell-derived tumor cells visible on a lymph node biopsy. Non-Hodgkin lymphomas do not. Second, Hodgkin lymphoma usually starts in one lymph node group and spreads to the next adjacent group in a predictable pattern, while non-Hodgkin lymphoma tends to be more scattered from the start. This orderly spread is why staging guides treatment so closely in Hodgkin lymphoma.
Is Hodgkin lymphoma curable?
Yes. Hodgkin lymphoma is one of the most curable cancers. The 5-year relative survival rate in the United States is around 89%, and most patients with early-stage disease can expect long-term remission. Even advanced-stage disease has a 5-year survival around 83%. Cure rates have improved further with newer regimens such as nivolumab plus AVD chemotherapy.
What are B symptoms and why do they matter?
B symptoms are three specific findings used in staging: unexplained fever above 38 °C, drenching night sweats, and unexplained weight loss greater than 10% of body weight over 6 months. They matter because their presence (designated "B" after the stage number, as in "stage IIB") signals more systemic disease and influences prognosis and treatment intensity.
What does PET-CT do that a regular CT does not?
A regular CT shows anatomy — the size and shape of organs and lymph nodes. A PET-CT adds a metabolic image: cancer cells take up a radiolabeled sugar more avidly than normal tissue, so they light up. This combination allows doctors to see disease that a CT alone might miss, and it lets them measure how well treatment is working partway through chemotherapy. PET-CT is now central to both staging (via the Lugano classification) and response assessment in Hodgkin lymphoma.
Why is Reed-Sternberg cell identification so important for diagnosis?
The Reed-Sternberg cell is the diagnostic hallmark of classic Hodgkin lymphoma. But these cells are sparse (often less than 1% of the cells in an affected lymph node) so a small needle biopsy can easily miss them. That is why an excisional biopsy, which removes a whole lymph node, is preferred. The pathologist needs both the Reed-Sternberg cells and the surrounding inflammatory background to make the diagnosis with confidence.
Glossary of Related Medical Terms
- Allogeneic stem cell transplant — A transplant using stem cells from a matched donor (rather than the patient's own).
- Autologous stem cell transplant — A transplant using the patient's own stem cells, harvested before high-dose chemotherapy.
- B symptoms — A specific trio of constitutional symptoms used in lymphoma staging: unexplained fever above 38 °C, drenching night sweats, and unexplained weight loss greater than 10% of body weight over 6 months.
- Cachexia — Severe weight loss and muscle wasting linked to chronic illness.
- CD15, CD20, CD30, CD45 — Cluster-of-differentiation markers: surface proteins on cells that are detected by antibodies to identify cell type. Their pattern fingerprints which lymphoma is which.
- Deauville criteria — A 5-point visual scoring system for interpreting PET scans during and after lymphoma treatment.
- Epstein-Barr virus (EBV) — A common human herpesvirus that causes infectious mononucleosis and is linked to several lymphomas.
- Excisional biopsy — Surgical removal of an entire lymph node for laboratory examination.
- FDG-avid — Taking up the radiolabeled sugar (fluorodeoxyglucose) used in PET scans, indicating high metabolic activity typical of cancer cells.
- Hypermetabolism — A state of increased energy use by the body, leading to weight loss, fatigue, and night sweats.
- Immunohistochemistry (IHC) — A laboratory technique that uses antibodies to stain specific proteins in tissue, helping identify cell types under the microscope.
- Lacunar cell — A variant of a Reed-Sternberg cell seen in nodular sclerosis classic Hodgkin lymphoma; appears to sit in an empty space because its cytoplasm shrinks during processing.
- Lugano classification — The current standard staging system for Hodgkin and non-Hodgkin lymphoma, integrating PET-CT findings.
- Lymphadenopathy — Enlarged lymph nodes.
- Pel-Ebstein fever — A rare but classic pattern of fevers in Hodgkin lymphoma, cycling over days to weeks.
- PET-CT — Combined positron emission tomography and computed tomography scan; shows both metabolic activity and anatomical detail.
- Popcorn cell — A variant Reed-Sternberg cell with a lobulated nucleus that looks like a popped kernel of corn; characteristic of NLPHL/NLPBL.
- Pruritus — Itching.
- Reed-Sternberg cell — The large, abnormal B-cell-derived tumor cell that defines classic Hodgkin lymphoma. Often described as having an "owl-eye" appearance under the microscope.
- Splenomegaly — Enlargement of the spleen.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Alaggio, R., Amador, C., Anagnostopoulos, I., Attygalle, A. D., Araujo, I. B. O., Berti, E., Bhagat, G., Borges, A. M., Boyer, D., Calaminici, M., Chadburn, A., Chan, J. K. C., Cheuk, W., Chng, W. J., Choi, J. K., Chuang, S. S., Coupland, S. E., Czader, M., Dave, S. S., de Jong, D., … Xiao, W. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia, 36(7), 1720–1748. https://doi.org/10.1038/s41375-022-01620-2
- Campo, E., Jaffe, E. S., Cook, J. R., Quintanilla-Martinez, L., Swerdlow, S. H., Anderson, K. C., Brousset, P., Cerroni, L., de Leval, L., Dirnhofer, S., Dogan, A., Feldman, A. L., Fend, F., Friedberg, J. W., Gaulard, P., Ghia, P., Horwitz, S. M., King, R. L., Salles, G., San-Miguel, J., … Zelenetz, A. D. (2022). The International Consensus Classification of Mature Lymphoid Neoplasms: a report from the Clinical Advisory Committee. Blood, 140(11), 1229–1253. https://doi.org/10.1182/blood.2022015851
- Herrera, A. F., LeBlanc, M., Castellino, S. M., Li, H., Rutherford, S. C., Evens, A. M., Davison, K., Punnett, A., Parsons, S. K., Ahmed, S., Casulo, C., Bartlett, N. L., Tuscano, J. M., Mei, M. G., Hess, B. T., Jacobs, R., Saeed, H., Torka, P., Hu, B., Moskowitz, C., … Friedberg, J. W. (2024). Nivolumab+AVD in Advanced-Stage Classic Hodgkin's Lymphoma. The New England journal of medicine, 391(15), 1379–1389. https://doi.org/10.1056/NEJMoa2405888
- Eichenauer, D. A., Aleman, B. M. P., André, M., Federico, M., Hutchings, M., Illidge, T., Engert, A., Ladetto, M., & ESMO Guidelines Committee (2018). Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology, 29(Suppl 4), iv19–iv29. https://doi.org/10.1093/annonc/mdy080
- Cheson, B. D., Fisher, R. I., Barrington, S. F., Cavalli, F., Schwartz, L. H., Zucca, E., Lister, T. A., Alliance, Australasian Leukaemia and Lymphoma Group, Eastern Cooperative Oncology Group, European Mantle Cell Lymphoma Consortium, Italian Lymphoma Foundation, European Organisation for Research, Treatment of Cancer/Dutch Hemato-Oncology Group, Grupo Español de Médula Ósea, German High-Grade Lymphoma Study Group, German Hodgkin's Study Group, Japanese Lymphorra Study Group, Lymphoma Study Association, NCIC Clinical Trials Group, Nordic Lymphoma Study Group, … United Kingdom National Cancer Research Institute (2014). Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 32(27), 3059–3068. https://doi.org/10.1200/JCO.2013.54.8800
- Johnson, P., Federico, M., Kirkwood, A., Fosså, A., Berkahn, L., Carella, A., d'Amore, F., Enblad, G., Franceschetto, A., Fulham, M., Luminari, S., O'Doherty, M., Patrick, P., Roberts, T., Sidra, G., Stevens, L., Smith, P., Trotman, J., Viney, Z., Radford, J., … Barrington, S. (2016). Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin's Lymphoma. The New England journal of medicine, 374(25), 2419–2429. https://doi.org/10.1056/NEJMoa1510093
- Hasenclever, D., & Diehl, V. (1998). A prognostic score for advanced Hodgkin's disease. International Prognostic Factors Project on Advanced Hodgkin's Disease. The New England journal of medicine, 339(21), 1506–1514. https://doi.org/10.1056/NEJM199811193392104
- Borchmann, P., Eichenauer, D. A., Frigola, G., & Campo, E. (2025). Nodular Lymphocyte-Predominant Hodgkin Lymphoma: Update on Biology and Treatment. Hematological oncology, 43 Suppl 2(Suppl 2), e70080. https://doi.org/10.1002/hon.70080
- Spina, V., Bruscaggin, A., Cuccaro, A., Martini, M., Di Trani, M., Forestieri, G., Manzoni, M., Condoluci, A., Arribas, A., Terzi-Di-Bergamo, L., Locatelli, S. L., Cupelli, E., Ceriani, L., Moccia, A. A., Stathis, A., Nassi, L., Deambrogi, C., Diop, F., Guidetti, F., Cocomazzi, A., … Rossi, D. (2018). Circulating tumor DNA reveals genetics, clonal evolution, and residual disease in classical Hodgkin lymphoma. Blood, 131(22), 2413–2425. https://doi.org/10.1182/blood-2017-11-812073
- El-Galaly, T. C., d'Amore, F., Mylam, K. J., de Nully Brown, P., Bøgsted, M., Bukh, A., Specht, L., Loft, A., Iyer, V., Hjorthaug, K., Nielsen, A. L., Christiansen, I., Madsen, C., Johnsen, H. E., & Hutchings, M. (2012). Routine bone marrow biopsy has little or no therapeutic consequence for positron emission tomography/computed tomography-staged treatment-naive patients with Hodgkin lymphoma. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 30(36), 4508–4514. https://doi.org/10.1200/JCO.2012.42.4036
- Radford, J., Illidge, T., Counsell, N., Hancock, B., Pettengell, R., Johnson, P., Wimperis, J., Culligan, D., Popova, B., Smith, P., McMillan, A., Brownell, A., Kruger, A., Lister, A., Hoskin, P., O'Doherty, M., & Barrington, S. (2015). Results of a trial of PET-directed therapy for early-stage Hodgkin's lymphoma. The New England journal of medicine, 372(17), 1598–1607. https://doi.org/10.1056/NEJMoa1408648
- Ansell, S. M., Radford, J., Connors, J. M., Długosz-Danecka, M., Kim, W. S., Gallamini, A., Ramchandren, R., Friedberg, J. W., Advani, R., Hutchings, M., Evens, A. M., Smolewski, P., Savage, K. J., Bartlett, N. L., Eom, H. S., Abramson, J. S., Dong, C., Campana, F., Fenton, K., Puhlmann, M., … ECHELON-1 Study Group (2022). Overall Survival with Brentuximab Vedotin in Stage III or IV Hodgkin's Lymphoma. The New England journal of medicine, 387(4), 310–320. https://doi.org/10.1056/NEJMoa2206125
- Brahmer, J. R., Lacchetti, C., Schneider, B. J., Atkins, M. B., Brassil, K. J., Caterino, J. M., Chau, I., Ernstoff, M. S., Gardner, J. M., Ginex, P., Hallmeyer, S., Holter Chakrabarty, J., Leighl, N. B., Mammen, J. S., McDermott, D. F., Naing, A., Nastoupil, L. J., Phillips, T., Porter, L. D., Puzanov, I., … National Comprehensive Cancer Network (2018). Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 36(17), 1714–1768. https://doi.org/10.1200/JCO.2017.77.6385