Key Takeaways
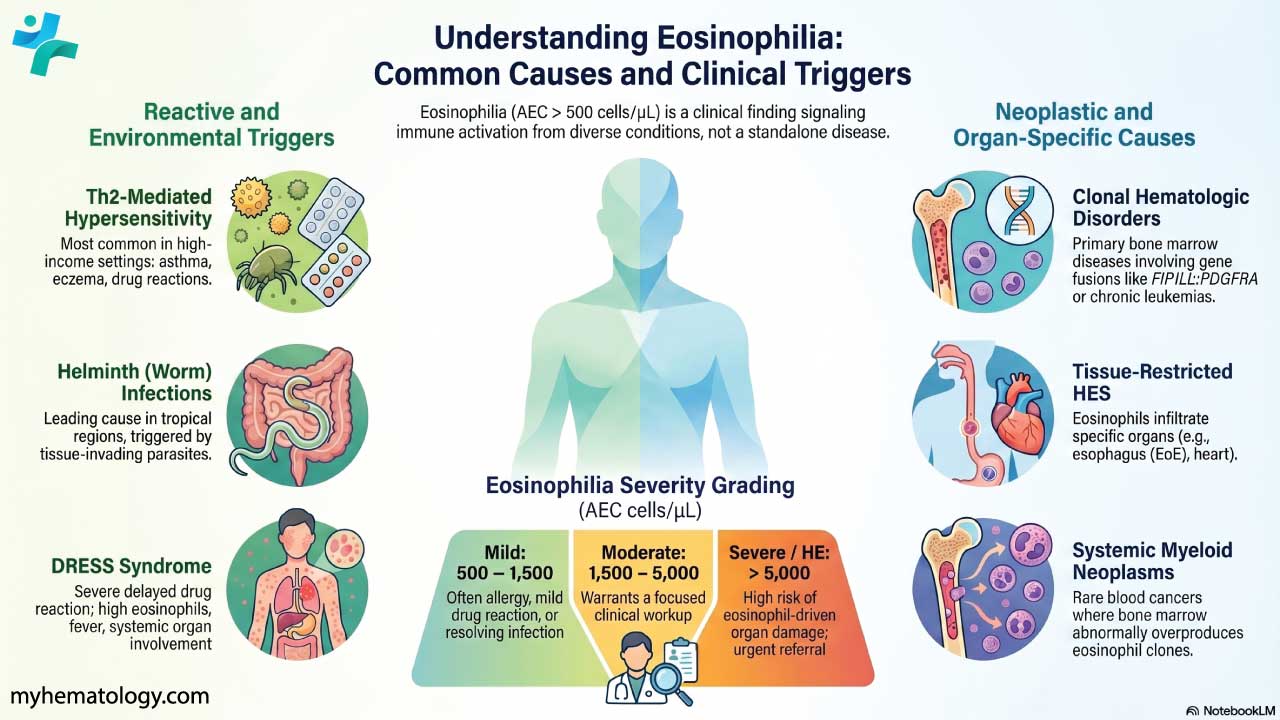
Eosinophilia is defined as more than 500 eosinophils per microliter (µL) of blood. It is a finding, not a disease, and signals that something, most often an allergy, parasite, drug reaction, or blood disorder, is driving the immune system [3].
- Causes ▾: The most common causes of eosinophilia split by geography: allergies, asthma, eczema, and drug reactions lead in high-income countries; helminth (worm) infections lead in tropical regions [3,4].
- Symptoms ▾: Vary widely depending on the cause and organs involved.
- Laboratory Investigations ▾: Confirm the count through CBC, rule out reactive causes, then if eosinophilia persists, move to bone marrow studies with cytogenetics and next-generation sequencing for fusion genes such as FIP1L1::PDGFRA [2,4].
- Treatment ▾: Treatment targets the cause first (antiparasitics, allergen avoidance, drug withdrawal). When eosinophils themselves drive organ damage, corticosteroids and IL-5–directed biologics are now mainstays [1,5].
*Click ▾ for more information
Introduction
Eosinophilia is a frequent and important laboratory finding, and it often turns up during routine bloodwork rather than as the reason a patient walks into clinic [3]. The trick is knowing what it signals — because the answer ranges from a passing allergy to a serious blood cancer. This article walks through what eosinophils do, what counts as eosinophilia, the main causes, how doctors investigate it, and how treatment has shifted over the past few years.

What are eosinophils?
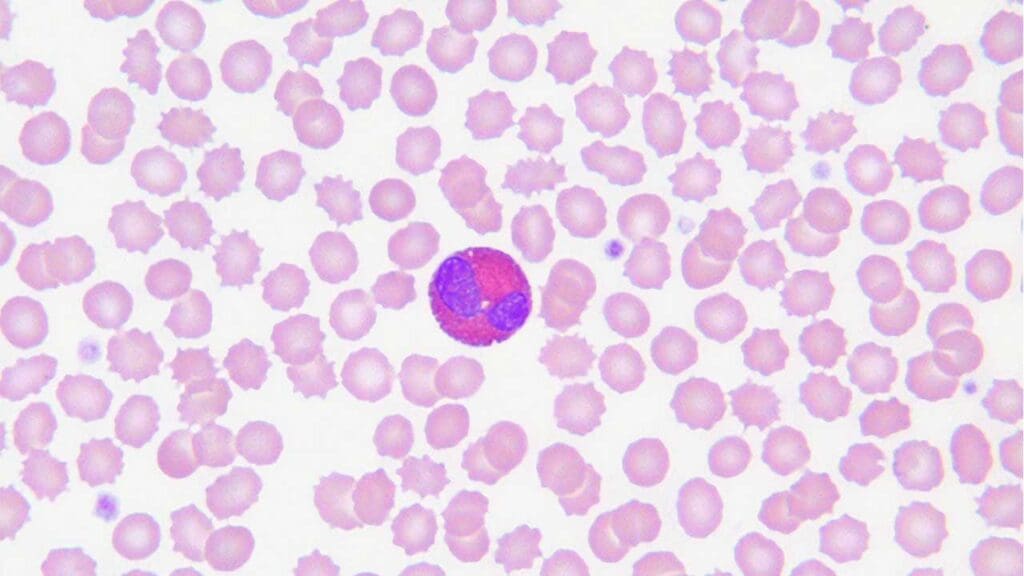
Eosinophils are a type of white blood cell, specifically a granulocyte (a white cell with granules in its cytoplasm). Their granules stain bright pink with eosin dye, which is how they got their name. Eosinophils have two well-known jobs: defending against parasitic worms and driving allergic inflammation [1].
What is a normal eosinophil count?
A normal absolute eosinophil count (AEC) is less than 500 cells per microliter (µL) or (< 0.5 x 10⁹/L). Reference ranges vary slightly between laboratories, so always check the range printed on the report.
What is Eosinophilia (High Eosinophils)?
Eosinophilia means an absolute eosinophil count above 500 cells/µL in the peripheral blood [3]. It is not a disease on its own. It is a signal that the bone marrow is producing more eosinophils than usual, usually because something is telling it to.
Mild eosinophilia
What it usually means Often allergy, mild drug reaction, or resolving infection.
Moderate eosinophilia
What it usually means Warrants a focused workup.
Severe eosinophilia / Hypereosinophilia (HE)
What it usually means Risk of eosinophil-driven organ damage; specialist referral [1,2].
When hypereosinophilia is accompanied by organ damage caused by the eosinophils, the picture is called hypereosinophilic syndrome (HES) [2].
Causes of Eosinophilia
Eosinophilia has a long list of causes, but they cluster into a manageable set of groups. The 2024 international consensus update sorts the more severe end of the spectrum into four buckets — HEFA (familial), HEUS (of undetermined significance), HEN (neoplastic/clonal), and HER (reactive) — which maps neatly onto how clinicians think about the workup [2].
Allergic and hypersensitivity reactions
Allergies are the most common driver of eosinophilia in high-income settings. The mechanism is a Th2 response: helper T cells release cytokines, particularly interleukin-5 (IL-5), which acts as a growth and survival signal for eosinophils. IL-4 and IL-13 also play roles. IL-5 is so central that several of the newer treatments simply block it [1].
Once recruited, eosinophils release toxic granule proteins (major basic protein, eosinophil cationic protein, eosinophil peroxidase, eosinophil-derived neurotoxin) that damage tissue and prolong inflammation.
Common allergic causes include:
- Asthma, especially eosinophilic asthma where sputum and blood eosinophils run high.
- Allergic rhinitis and conjunctivitis, often with eosinophils visible on nasal smears.
- Atopic dermatitis (eczema), with eosinophil infiltration in skin biopsies.
- Drug hypersensitivity reactions, ranging from mild rashes to DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms), which presents 2–8 weeks after exposure with fever, rash, swollen nodes, and organ involvement [3].
- Food allergies, sometimes with gastrointestinal symptoms and tissue eosinophilia on endoscopic biopsy.
Infections
Eosinophils are best known for defending against helminths (parasitic worms). The presence of helminth larvae migrating through tissue triggers a strong Th2 response and a sharp rise in eosinophils [3].
Common infectious causes:
- Intestinal helminths such as Ascaris, hookworm, Strongyloides, and whipworm. These are especially common in tropical regions.
- Tissue-invading helminths such as schistosomiasis, cysticercosis, and echinococcosis.
- Fungal infections, particularly Allergic Bronchopulmonary Aspergillosis (ABPA), an allergic response to Aspergillus in the airways.
- Protozoa rarely cause marked eosinophilia, with a few exceptions like Cystoisospora belli.
- Some viral infections can produce transient mild eosinophilia during recovery.
Before starting long-term steroids or immunosuppressants in anyone with eosinophilia from an endemic region, screen for Strongyloides with serology. Untreated strongyloidiasis can disseminate fatally under immunosuppression [3].
Hematologic disorders
A subset of eosinophilia comes from the bone marrow itself producing eosinophils abnormally. This is the HEN (neoplastic) category in the new classification [2].
The 2022 WHO classification groups several of these conditions under a major umbrella: myeloid/lymphoid neoplasms with eosinophilia and tyrosine-kinase gene fusions (MLN-eo-TK). This category covers rearrangements of PDGFRA, PDGFRB, FGFR1, JAK2, and FLT3 [2]. Identifying the specific gene fusion matters because some of them, most famously FIP1L1::PDGFRA, respond dramatically to the tyrosine kinase inhibitor imatinib [2,4].
Key hematologic causes:
- Hypereosinophilic syndrome (HES) — persistently elevated AEC >1500/µL (> 1.5 x 10⁹/L) with organ damage. Now subclassified as HEFA, HEUS, HEN, or HER depending on the underlying mechanism [1,2].
- Chronic eosinophilic leukemia (CEL) — a rare myeloproliferative neoplasm with sustained clonal eosinophilia.
- MLN-eo-TK — the WHO 2022 category above.
- Hodgkin lymphoma — Reed-Sternberg cells release cytokines (including IL-5) that recruit eosinophils. Treating the lymphoma usually resolves the eosinophilia.
- Systemic mastocytosis with an associated hematologic neoplasm — mast cell disease can present alongside eosinophilic disorders.
Organ-Specific Eosinophilic Diseases
In these conditions, eosinophils accumulate in one organ rather than circulating in high numbers. Peripheral eosinophilia may be modest or absent. The 2024 consensus introduced the term tissue-restricted HES for these cases [2].
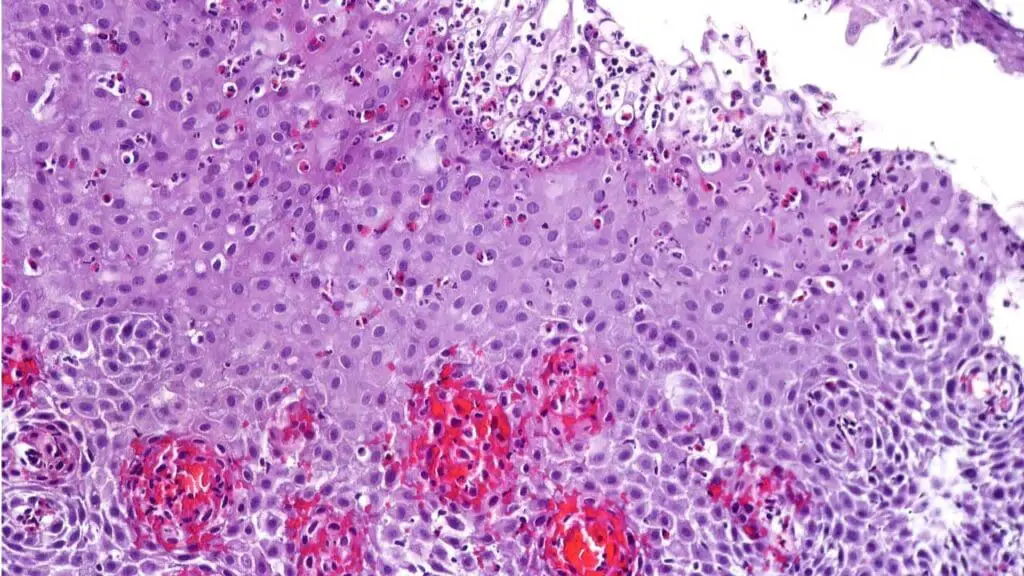
- Eosinophilic esophagitis (EoE) — eosinophils packed into the esophageal lining, causing trouble swallowing and food impaction. Triggered mostly by food antigens. Diagnosis needs endoscopy with biopsy.
- Eosinophilic gastroenteritis (EoG) — similar mechanism, lower in the gut.
- Eosinophilic asthma — a severe asthma subtype with high airway eosinophils, often very responsive to anti-IL-5 biologics.
- Eosinophilic myocarditis — eosinophil infiltration of heart muscle. Can present with heart failure, arrhythmias, or sudden death. Diagnosed on cardiac MRI and endomyocardial biopsy.
- Eosinophilic pneumonia — lung infiltration causing cough and breathlessness.
- Eosinophilic dermatoses — including bullous pemphigoid and Wells syndrome.
Other Causes
- Connective tissue diseases, especially Eosinophilic Granulomatosis with Polyangiitis (EGPA), formerly Churg-Strauss syndrome. Asthma, vasculitis, and eosinophilia together [5].
- Endocrine disorders — Addison's disease can produce mild eosinophilia.
- Solid tumors — some release cytokines that drive eosinophil production.
- Primary immunodeficiencies — rare but can present with eosinophilia.
Idiopathic Eosinophilia
Sometimes a thorough workup turns up nothing. This is idiopathic eosinophilia, which the new classification calls HEUS (hypereosinophilia of undetermined significance) when sustained [2]. Some of these cases eventually declare themselves as a defined disorder.
Symptoms
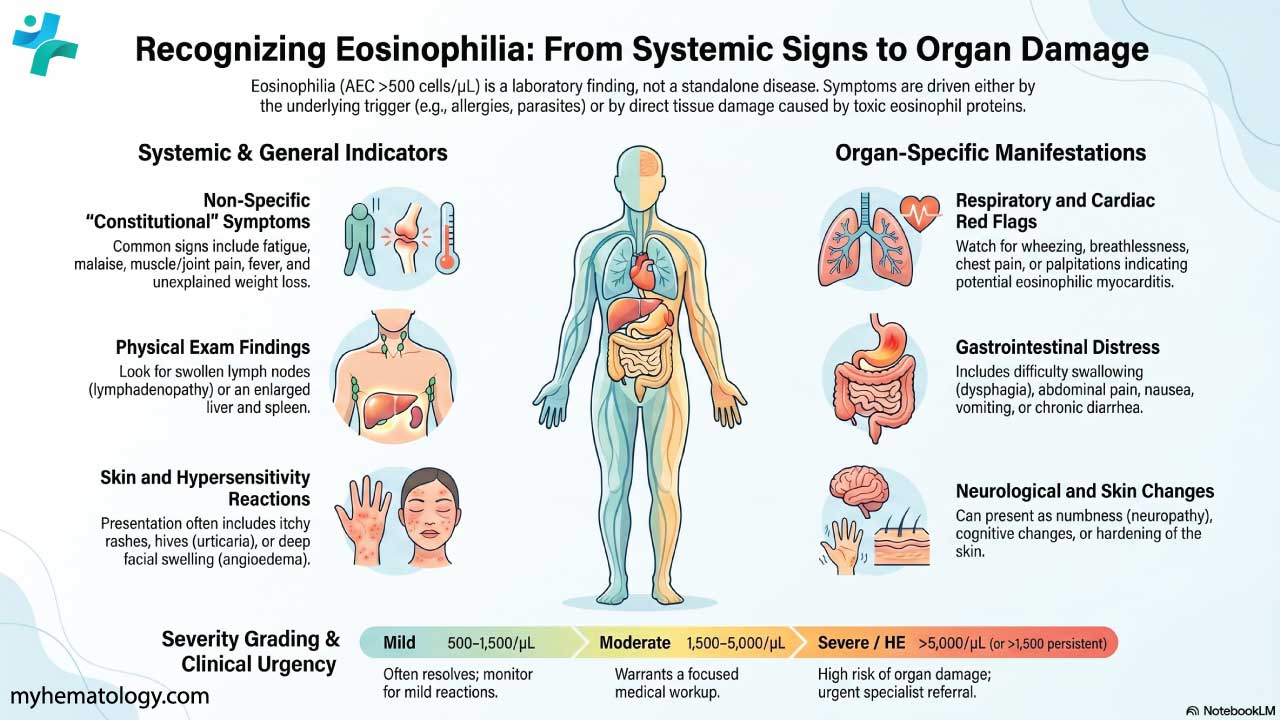
Eosinophilia itself produces no symptoms. The clinical picture comes from the underlying cause and from any organ damage the eosinophils have done.
General symptoms
These are non-specific and overlap with many conditions: fatigue, malaise, muscle aches (myalgia), joint pain (arthralgia), weight loss, fever, and night sweats.
Systemic features
These point to more widespread involvement:
- Lymphadenopathy — swollen lymph nodes.
- Hepatomegaly or splenomegaly — enlarged liver or spleen, common in HES and lymphomas.
- Skin rashes — urticaria, eczema-like patches, or nodules.
- Angioedema — deeper swelling of the face, lips, or throat in allergic reactions.
Organ-specific symptoms
These reflect where eosinophils have actually accumulated.
Respiratory: cough, wheezing, breathlessness, chest tightness, occasionally hemoptysis (coughing up blood).
Gastrointestinal: dysphagia (difficulty swallowing) and food impaction in EoE; abdominal pain, nausea, vomiting, and diarrhea in EoG; reflux symptoms.
Cardiac: chest pain, palpitations, breathlessness on exertion, leg swelling — all red flags for eosinophilic myocarditis.
Skin: itching, varied rashes, hardening or swelling of the skin.
Nervous system: numbness, tingling, or weakness (peripheral neuropathy). Severe cases in HES or EGPA can cause cognitive changes or seizures.
Red flags that warrant urgent specialist referral
AEC persistently above 1500/µL (> 1.5 x 10⁹/L), any cardiac or neurological symptoms, fever with weight loss, or rapidly rising counts [1,2].
Laboratory Investigations
The workup follows a logical sequence: confirm the count, look for reactive causes first, then investigate for clonal disease if eosinophilia persists [2,4].
Step 1 — Confirm and characterize
- Complete blood count (CBC) with differential. Confirms AEC and severity.
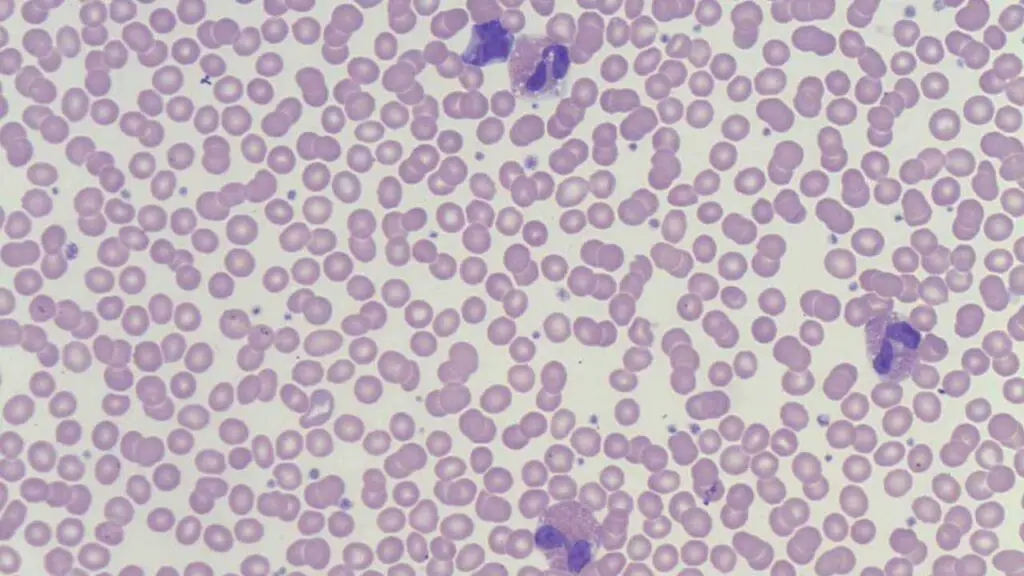
- Peripheral blood smear. Looks for dysplastic eosinophils, immature cells, or other abnormalities suggesting a marrow disorder. Occasionally reveals circulating microfilariae from parasitic infections.
- Inflammatory markers (ESR, CRP). Non-specific but flag systemic inflammation.
- Serum total IgE. Elevated in allergic conditions and some parasitic infections.
Step 2 — Look for reactive causes
- Detailed history and examination. Travel, diet, drug list, atopic history, occupational exposure.
- Stool examination for ova and parasites (O&P). Serial samples improve yield.
- Allergy testing — skin prick tests and specific IgE (RAST).
- Strongyloides serology in anyone with relevant exposure, especially before steroids [3].
- Organ-specific imaging and biopsy guided by symptoms: chest imaging and bronchoalveolar lavage for lung disease, endoscopy with biopsy for gut symptoms, echocardiogram and cardiac MRI for cardiac concerns, skin biopsy for dermatologic disease.
Step 3 — Investigate for clonal or systemic disease
When eosinophilia is persistent and reactive causes have been excluded:
- Serum tryptase and vitamin B12. An elevated serum tryptase strongly points toward systemic mastocytosis or the FIP1L1::PDGFRA fusion, rapidly identifying patients who are highly likely to have a dramatic response to imatinib [8].
- Serological tests for connective tissue disease, including ANCA for EGPA.
- Bone marrow aspiration and biopsy. Examines marrow cellularity and morphology.
- Cytogenetics, FISH, and next-generation sequencing. Looks for FIP1L1::PDGFRA and other tyrosine-kinase fusions in the MLN-eo-TK category [2,4].
- Flow cytometry and T-cell receptor (TCR) clonality studies. Identifies lymphocyte-variant HE.
Treatment and Management
The first principle is straightforward: treat the cause. Direct suppression of eosinophils is reserved for when the cause cannot be removed, or when the eosinophilia is itself damaging organs [1,2].
Treat the underlying cause
- Parasitic infections — antiparasitics chosen by organism: albendazole, mebendazole, ivermectin, or praziquantel. Repeat stool testing confirms eradication.
- Allergic conditions — allergen avoidance, antihistamines, topical or inhaled corticosteroids, leukotriene modifiers, and epinephrine auto-injectors for anaphylaxis.
- Drug hypersensitivity — stop the offending drug immediately. Support as needed for severe reactions like DRESS.
- Hematologic disorders — guided by subtype. FIP1L1::PDGFRA-positive disease responds to imatinib, often dramatically. Other MLN-eo-TK subtypes may also respond to tyrosine kinase inhibitors [2,4].
- Hodgkin lymphoma — chemotherapy and/or radiotherapy. Treating the lymphoma resolves the reactive eosinophilia.
- Organ-specific eosinophilic diseases:
- EoE — dietary elimination, topical swallowed corticosteroids (fluticasone, budesonide), proton pump inhibitors, esophageal dilation, and dupilumab (FDA-approved for adults in 2022, and expanded in early 2024 to include children aged 1 year and older weighing at least 15 kg) [6].
- EoG — corticosteroids and dietary modifications.
- Eosinophilic asthma — inhaled corticosteroids plus anti-IL-5 biologics (mepolizumab, reslizumab, benralizumab) or dupilumab for severe cases.
- Eosinophilic myocarditis — corticosteroids and heart failure management.
- EGPA — corticosteroids plus immunosuppressants (cyclophosphamide, azathioprine, methotrexate). Mepolizumab has been approved since 2017, and benralizumab was FDA-approved for EGPA in September 2024 based on the MANDARA trial [5].
Direct treatment of eosinophilia
When the cause cannot be removed or eosinophils are doing real organ damage:
- Systemic corticosteroids (e.g., prednisone) — still the workhorse first-line drug. Effective but with the usual long-term side-effect burden, so the goal is the lowest dose for the shortest time.
- Anti-IL-5 biologics — mepolizumab and reslizumab. Bind IL-5 itself. Approved for severe eosinophilic asthma and HES (mepolizumab) [1].
- Anti-IL-5 receptor biologic — benralizumab. Binds the IL-5 receptor on eosinophils and depletes them. Approved for severe eosinophilic asthma, EGPA (2024), and most recently HES (FDA approval in 2026) based on the NATRON Phase III trial, which showed a 65% reduction in HES flares [5]. For HES, benralizumab is administered every 4 weeks, distinguishing it from the 8-week maintenance interval used in severe asthma [7].
- Anti-IL-4/IL-13 biologic — dupilumab. Blocks signaling rather than depleting eosinophils. Approved for atopic dermatitis, eosinophilic asthma, EoE, and other Th2-driven conditions.
- Other immunosuppressants — hydroxyurea, azathioprine, methotrexate, interferon-alpha. Often used as steroid-sparing agents in HES.
- Tyrosine kinase inhibitors — imatinib for FIP1L1::PDGFRA-positive disease, sometimes nilotinib or other TKIs for related fusions [2].
Monitoring
Follow-up is built around three checks: serial AECs to track response, organ-specific monitoring (echocardiograms, pulmonary function tests, endoscopy where relevant), and watching for treatment side effects, especially with chronic steroid or immunosuppressant use.
Frequently Asked Questions (FAQs)
Should I worry about mild eosinophilia?
Mild eosinophilia (500–1500/µL) is common and often resolves on its own. It can reflect a mild allergic reaction, a resolving infection, or a recent medication. That said, persistent mild eosinophilia, or any eosinophilia paired with new symptoms, deserves a closer look because it can be the early signal of something more significant.
What medications cause eosinophilia?
Many drugs can trigger eosinophilia through hypersensitivity. The most common culprits are antibiotics (penicillins, cephalosporins, sulfonamides, nitrofurantoin, vancomycin, minocycline), NSAIDs (aspirin, ibuprofen, naproxen), anticonvulsants (phenytoin, carbamazepine, lamotrigine), allopurinol, ACE inhibitors, antiretrovirals (abacavir, nevirapine), thiazide diuretics, and some chemotherapy agents. Severity varies from a mild blood-count blip to full DRESS syndrome.
Can COVID-19 cause high eosinophils?
The acute phase of COVID-19 more often produces low eosinophils (eosinopenia). While heavily monitored early in the pandemic, it is now recognized that eosinopenia is a general marker of acute viral stress (also seen in RSV and influenza) rather than a feature strictly unique to COVID-19 [9].
How long should eosinophilia persist before more testing?
A single mildly elevated reading in someone who feels well is usually repeated in a few weeks rather than worked up immediately. Counts above 1500/µL confirmed on two readings at least one month apart meet the definition of hypereosinophilia and warrant a structured specialist workup, regardless of symptoms [2].
What parasites cause high eosinophils?
Tissue-invading helminths (worms) are the classic cause. Key examples include:
- Roundworms (nematodes): Ascaris lumbricoides, Strongyloides stercoralis, hookworms (Ancylostoma, Necator), Toxocara, Trichinella spiralis, filarial worms (Wuchereria, Brugia, Onchocerca, Loa loa), Angiostrongylus cantonensis (eosinophilic meningitis), and Paragonimus lung flukes.
- Flukes (trematodes): Schistosoma, Fasciola hepatica, Clonorchis sinensis, Opisthorchis.
- Tapeworms (cestodes): Echinococcus (especially with cyst leakage), Taenia solium (cysticercosis).
Protozoa rarely cause marked eosinophilia. Scabies (Sarcoptes scabiei) can produce mild eosinophilia from skin inflammation.
Glossary of Related Medical Terms
- Eosinophil — A type of white blood cell with bright red/pink granules that helps fight parasites and drives allergic inflammation.
- Absolute eosinophil count (AEC) — The actual number of eosinophils per microliter of blood. Calculated from the white cell count and the eosinophil percentage on the differential.
- Eosinophilia — An AEC above 500 cells/µL.
- Hypereosinophilia (HE) — A more severe and sustained elevation, with AEC above 1500 cells/µL on two readings at least one month apart, or marked tissue infiltration.
- Hypereosinophilic syndrome (HES) — Hypereosinophilia plus eosinophil-driven organ damage.
- Granulocyte — A white cell with granules in its cytoplasm. Eosinophils, neutrophils, and basophils are the three types.
- Th2 response — An immune pattern driven by helper T cells that releases IL-4, IL-5, and IL-13. Central to allergy and anti-parasite defense.
- Interleukin-5 (IL-5) — A signaling protein that grows, recruits, and keeps eosinophils alive. The target of mepolizumab, reslizumab, and (via its receptor) benralizumab.
- MLN-eo-TK — Myeloid/lymphoid neoplasms with eosinophilia and tyrosine-kinase gene fusions. A WHO 2022 category covering PDGFRA, PDGFRB, FGFR1, JAK2, and FLT3 rearrangements.
- DRESS syndrome — Drug Reaction with Eosinophilia and Systemic Symptoms. A severe delayed drug reaction with fever, rash, swollen nodes, and organ involvement.
- Eosinophilic esophagitis (EoE) — Chronic immune-driven inflammation of the esophagus packed with eosinophils, often triggered by food.
- Helminth — A parasitic worm. The most common infectious cause of marked eosinophilia worldwide.
- Tyrosine kinase inhibitor (TKI) — A drug that blocks abnormal signaling proteins inside cancer cells. Imatinib is the example for FIP1L1::PDGFRA-positive disease.
- Bone marrow aspiration — A procedure that samples cells from inside the bone to look for blood cancers or production problems.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Valent, P., Klion, A. D., Roufosse, F., Simon, D., Metzgeroth, G., Leiferman, K. M., Schwaab, J., Butterfield, J. H., Sperr, W. R., Sotlar, K., Vandenberghe, P., Hoermann, G., Haferlach, T., Moriggl, R., George, T. I., Akin, C., Bochner, B. S., Gotlib, J., Reiter, A., Horny, H. P., … Gleich, G. J. (2023). Proposed refined diagnostic criteria and classification of eosinophil disorders and related syndromes. Allergy, 78(1), 47–59. https://doi.org/10.1111/all.15544
- Shomali, W., & Gotlib, J. (2024). World Health Organization and International Consensus Classification of eosinophilic disorders: 2024 update on diagnosis, risk stratification, and management. American journal of hematology, 99(5), 946–968. https://doi.org/10.1002/ajh.27287
- Kanuru S, Sapra A. Eosinophilia. [Updated 2023 Jun 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560929/
- Weaver, M. D., Glass, B., Aplanalp, C., Patel, G., Mazhil, J., Wang, I., & Dalia, S. (2024). Review of Peripheral Blood Eosinophilia: Workup and Differential Diagnosis. Hemato, 5(1), 81-108. https://doi.org/10.3390/hemato5010008
- Wechsler, M. E., Nair, P., Terrier, B., Walz, B., Bourdin, A., Jayne, D. R. W., Jackson, D. J., Roufosse, F., Börjesson Sjö, L., Fan, Y., Jison, M., McCrae, C., Necander, S., Shavit, A., Walton, C., Merkel, P. A., & MANDARA Study Group (2024). Benralizumab versus Mepolizumab for Eosinophilic Granulomatosis with Polyangiitis. The New England journal of medicine, 390(10), 911–921. https://doi.org/10.1056/NEJMoa2311155
- https://globalgenes.org/raredaily/fda-expands-use-of-dupixent-to-include-kids-with-eoe-1-year-and-older/
- Ogbogu, P. U., Roufosse, F., Akuthota, P., Kuna, P., Groh, M., Reiter, A., Yokota, A., Siddiqui, S. H., Mutsaers, P. G. N. J., Li, B., Khoury, P., Bahadori, L. M., Bednarczyk, A., Bouma, G., Brooks, L. G., Ferreira, J., Grindebacke, H., Ho, C. N., Jain, P., Palmer, R. L., … NATRON study group (2026). Benralizumab versus placebo for hypereosinophilic syndrome: a randomized, placebo-controlled phase 3 trial. Nature medicine, 10.1038/s41591-026-04315-8. Advance online publication. https://doi.org/10.1038/s41591-026-04315-8
- Klion, A. D., Noel, P., Akin, C., Law, M. A., Gilliland, D. G., Cools, J., Metcalfe, D. D., & Nutman, T. B. (2003). Elevated serum tryptase levels identify a subset of patients with a myeloproliferative variant of idiopathic hypereosinophilic syndrome associated with tissue fibrosis, poor prognosis, and imatinib responsiveness. Blood, 101(12), 4660–4666. https://doi.org/10.1182/blood-2003-01-0006
- Macchia, I., La Sorsa, V., Urbani, F., Moretti, S., Antonucci, C., Afferni, C., & Schiavoni, G. (2023). Eosinophils as potential biomarkers in respiratory viral infections. Frontiers in immunology, 14, 1170035. https://doi.org/10.3389/fimmu.2023.1170035


