Key Takeaways
Acute myeloid leukemia or AML is an aggressive blood cancer in which the bone marrow makes too many immature myeloid cells (blasts) that cannot mature into working red cells, white cells, or platelets.
- Predisposing factors ▾: DNA damaging agents e.g. radiotherapy, chemotherapy, Iinherited DNA repair mutations, smoking, toxins e.g. benzene & MPN/MDS
- Signs and symptoms ▾: Triad of bone marrow failure; Anemia (Fatigue and pallor), Neutropenia (Recurrent, severe infections/fevers), & Thrombocytopenia (Petechiae, bruising, and gum bleeding).
- Laboratory Investigations ▾: Diagnosis combines four lab pillars: morphology (blasts and Auer rods), flow cytometry (CD13, CD33, CD117, MPO), cytogenetics, and next-generation sequencing for NPM1, FLT3, IDH1/2, TP53, and KMT2A [1,2].
- Treatment and Management ▾: "7+3" intensive chemotherapy for fit patients, venetoclax plus azacitidine for older or unfit patients, and ATRA plus arsenic trioxide for acute promyelocytic leukemia (APL) [1,5,6].
- Emergency Complications ▾: Neutropenic Sepsis (overwhelming infection) and Leukostasis (blood becoming too "thick" with blasts, causing strokes or lung issues).
*Click ▾ for more information
Introduction
AML is a fast-growing cancer of the bone marrow. It usually announces itself over weeks rather than months: someone who felt well in March is suddenly bruising for no reason, running fevers, and unable to climb stairs without resting. By the time a complete blood count is checked, the marrow may already be packed with blasts.
Acute myeloid leukemia is not one disease. It is a family of disorders that share a single visible feature, the build-up of immature myeloid cells in the bone marrow, but differ profoundly at the genetic level [4]. That genetic diversity is why two patients with identical-looking blood films can have very different outcomes, and why modern AML care has shifted from "what does the cell look like?" to "what mutations does it carry?"
This article walks through how AML develops, how it presents, how it is diagnosed under the 2022 WHO classification, and how it is treated in 2026.
How AML Develops: Pathogenesis
AML rarely happens in a single step. It is a layered process in which a stem cell picks up several genetic and epigenetic hits, each pushing the cell further from normal behavior.
The "Multi-Hit" Model
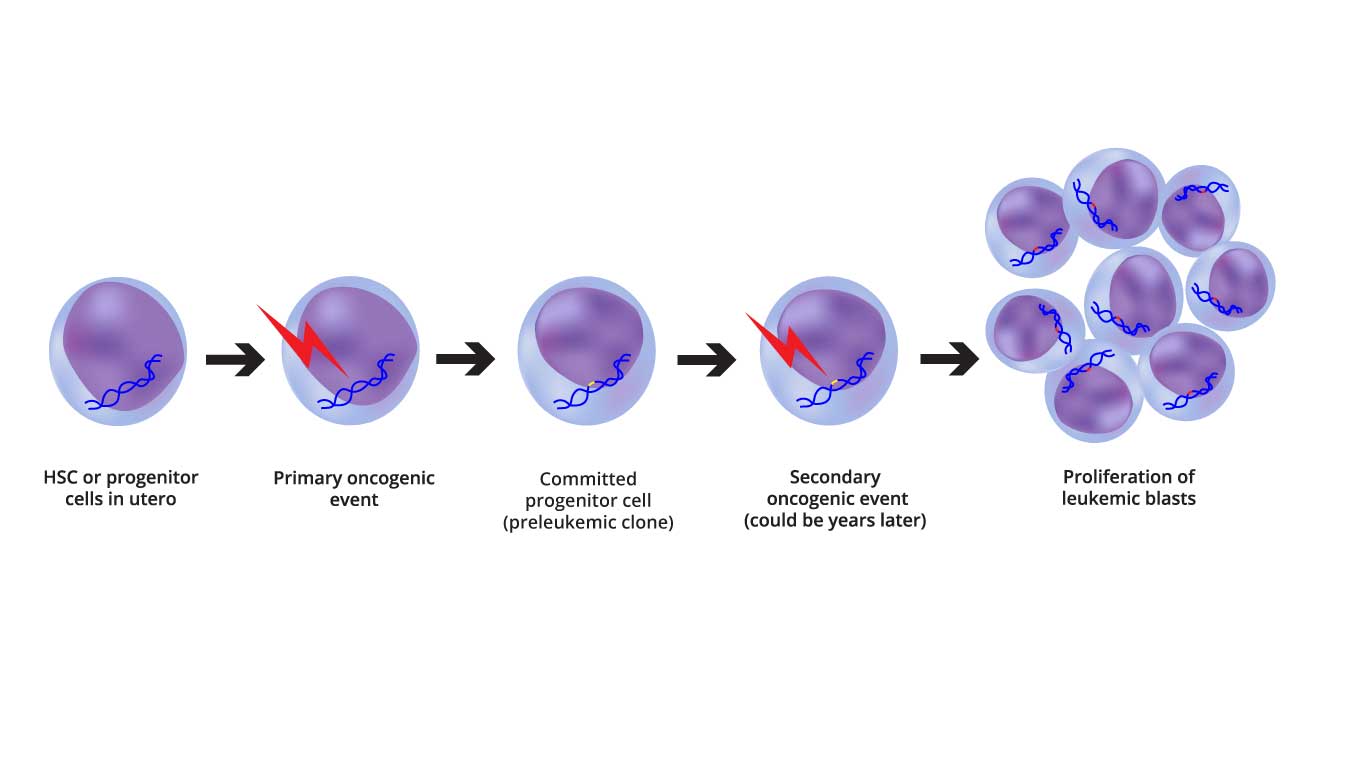
Image depicting the two-step oncogenic model of AML pathogenesis, highlighting the initial genetic alterations and the subsequent epigenetic and transcriptional changes.
Hematologists group AML mutations into three functional categories, sometimes called "gas pedals," "brakes," and "architects."
- Class I — proliferation drivers. Mutations in FLT3, KIT, or RAS tell the cell to divide constantly. They are the gas pedal.
- Class II — differentiation blockers. Mutations or translocations involving NPM1, t(8;21), or inv(16) freeze the cell at the blast stage. They are the broken brake on maturation.
- Epigenetic regulators. Mutations in DNMT3A, TET2, IDH1, and IDH2 change which genes are read without altering the DNA sequence itself. They are the architect, often laying the foundation years before AML appears.
A leukemia usually requires hits from more than one class. A FLT3 mutation alone makes a cell divide; an NPM1 mutation alone leaves it stuck. Combine them, and you have a clone that divides quickly and never matures.
From CHIP to Pre-Leukemia to AML
One of the most important ideas in modern hematology is that AML often begins quietly, decades before symptoms.
- Clonal hematopoiesis of indeterminate potential (CHIP). A single hematopoietic stem cell picks up a mutation, often in DNMT3A. Its descendants form a "clone" that looks normal but is genetically different. CHIP is common, especially after age 60.
- Pre-leukemic evolution. The clone gathers more mutations. It still produces functional blood cells but slowly out-competes its neighbors.
- The transformation. A final, aggressive hit, often FLT3-ITD or a chromosomal translocation, tips the balance. The clone now divides faster than healthy cells, fails to mature, and crowds the marrow.
The marrow itself helps the leukemia grow. AML cells reshape the local environment (the "niche") to favor their own survival and learn to ignore the apoptosis (cell-suicide) signals that would normally remove them.
Risk Factors for AML
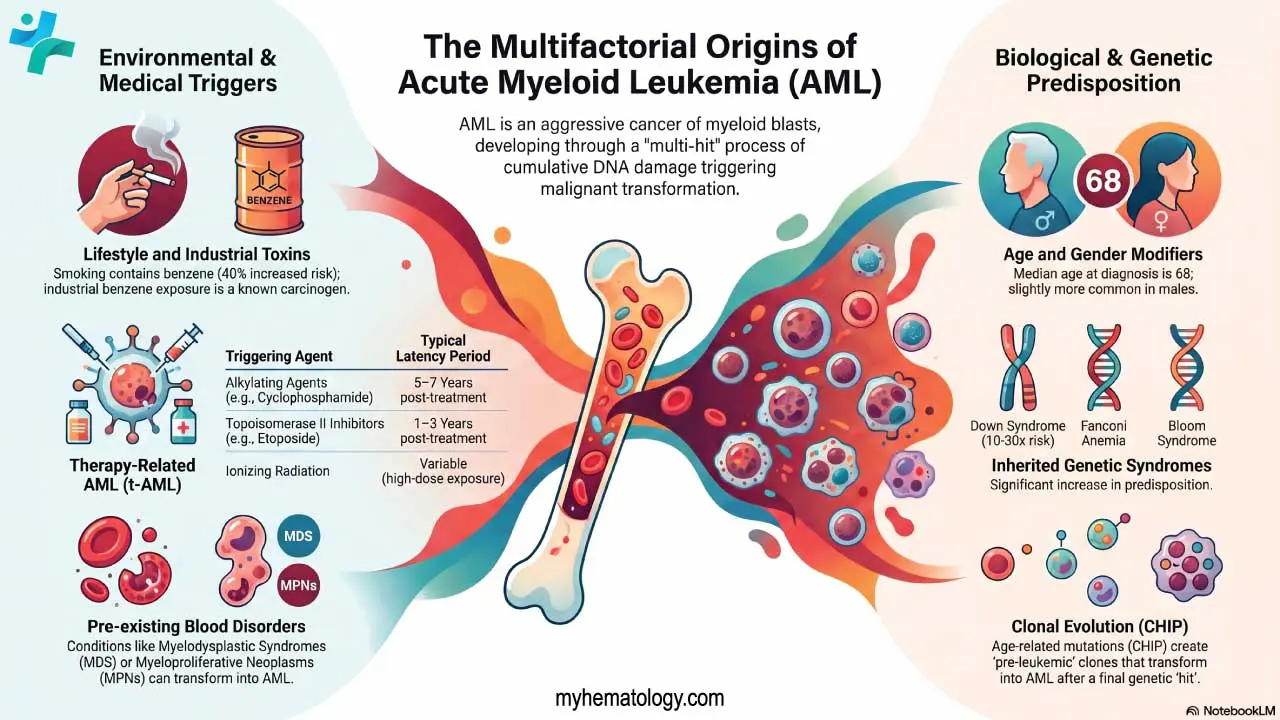
Environmental and Lifestyle Factors
- Smoking. Tobacco smoke contains benzene, a recognized human carcinogen. Heavy smokers carry roughly a 1.4-fold increased risk of AML compared with never-smokers.
- Benzene exposure. Beyond cigarettes, benzene is used in petroleum refining, chemical manufacturing, and rubber production. Painters and printers may face elevated risk with prolonged exposure.
- Ionizing radiation. Atomic-bomb survivors and patients who received high-dose therapeutic radiation have a clearly increased risk. The dose from routine diagnostic X-rays or CT scans is far too low to cause AML.
Medical History and Prior Treatments
AML that follows previous cancer treatment is called therapy-related AML (t-AML).
- Alkylating agents (cyclophosphamide, melphalan) typically lead to AML 5–7 years after exposure.
- Topoisomerase II inhibitors (etoposide, anthracyclines) act faster, often within 1–3 years.
- Pre-existing blood disorders can transform into AML. The main culprits are myelodysplastic syndromes (MDS), myeloproliferative neoplasms (MPNs) such as polycythemia vera, and aplastic anemia.
Genetic and Congenital Factors
Most AML is sporadic, but a small group of patients has an inherited predisposition.
- DNA-repair and bone-marrow-failure syndromes: Fanconi anemia, Bloom syndrome, Li-Fraumeni syndrome.
- Down syndrome: Children with Down syndrome have roughly a 20-fold increased risk of leukemia, especially acute megakaryoblastic leukemia (AML-M7) under age 5.
- Inherited gene mutations: Germline variants in RUNX1, CEBPA, DDX41, GATA2, ETV6, and ANKRD26 now have their own WHO 2022 category and warrant referral to genetic counseling [2].
Demographics
- Age is the single largest non-modifiable risk factor; the median age at diagnosis is approximately 68 years [10].
- Sex: AML is slightly more common in men, possibly due to occupational exposures.
Acute Myeloid Leukemia (AML) Symptoms
The symptoms of AML are a direct read-out of marrow failure. As blasts crowd out healthy cells, three lineages collapse together.
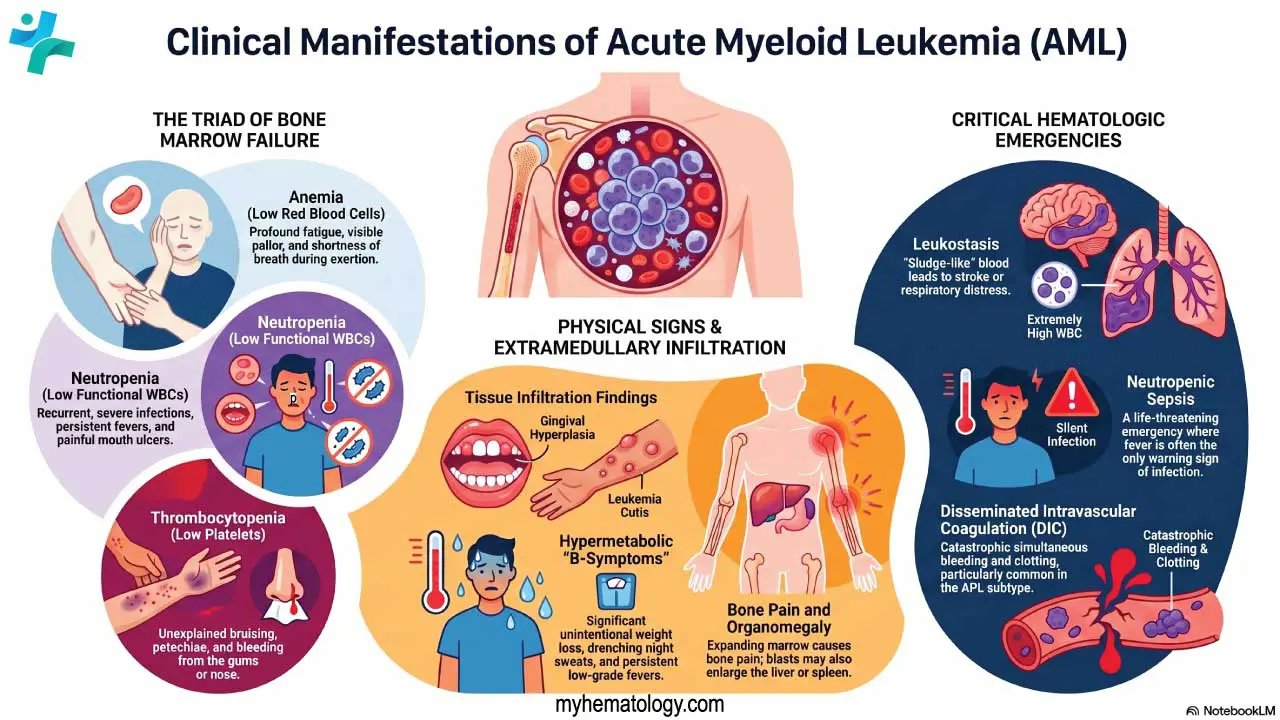
Bone Marrow Failure
- Anemia (low red cells) causes fatigue, pallor, and breathlessness on exertion.
- Neutropenia (low functional white cells) brings recurrent infections, mouth ulcers, and unexplained fevers.
- Thrombocytopenia (low platelets) produces bleeding gums, nosebleeds, petechiae (pinpoint red spots that do not blanch), and large unexplained bruises.
A patient who has all three at the same time (pancytopenia) should always be evaluated for an acute leukemia.
Extramedullary Spread (Blasts Outside the Marrow)
- Gingival hyperplasia. Swollen, painful gums that overgrow the teeth are classic for monocytic AML subtypes (FAB M4 and M5).
- Leukemia cutis. Firm, painless, skin-colored to purple skin nodules.
- Hepatomegaly and splenomegaly. More modest than in chronic leukemias but possible.
- Bone pain. The marrow cavity is under pressure from rapidly expanding blasts; the long bones and sternum hurt.
Hypermetabolic and "B" Symptoms
Rapidly dividing leukemia consumes energy. Patients may report unintentional weight loss, drenching night sweats, and persistent low-grade fever. If the blast count rises very fast, tumor lysis syndrome can appear even before treatment begins.
Hematologic Emergencies
These are time-critical and worth recognizing on first contact.
- Disseminated intravascular coagulation (DIC). Especially common in acute promyelocytic leukemia (APL), where leukemic granules spill pro-coagulant material into the blood. Patients can bleed and clot at the same time.
- Leukostasis. Typically occurs when the white-cell count exceeds about 100,000/µL, making the blood sludge-like and plugging small vessels in the lungs (causing breathlessness) and brain (causing confusion). However, in monocytic leukemias (FAB M4 and M5), leukostasis can occur at much lower counts (e.g., 40,000–50,000/µL) because the blasts are physically larger and more adherent.
- Neutropenic sepsis. The leading cause of treatment-related death in AML. Because there are too few neutrophils to mount inflammation, fever may be the only sign of a life-threatening infection. The "Golden Hour" rule applies: empirical broad-spectrum IV antibiotics within one hour of recognition, regardless of how stable the patient looks [1].
Modern Laboratory Diagnosis
AML diagnosis has moved from a microscope-only craft to an integrated workflow that combines morphology, immunophenotyping, cytogenetics, and molecular testing [1,2]. All four matter.
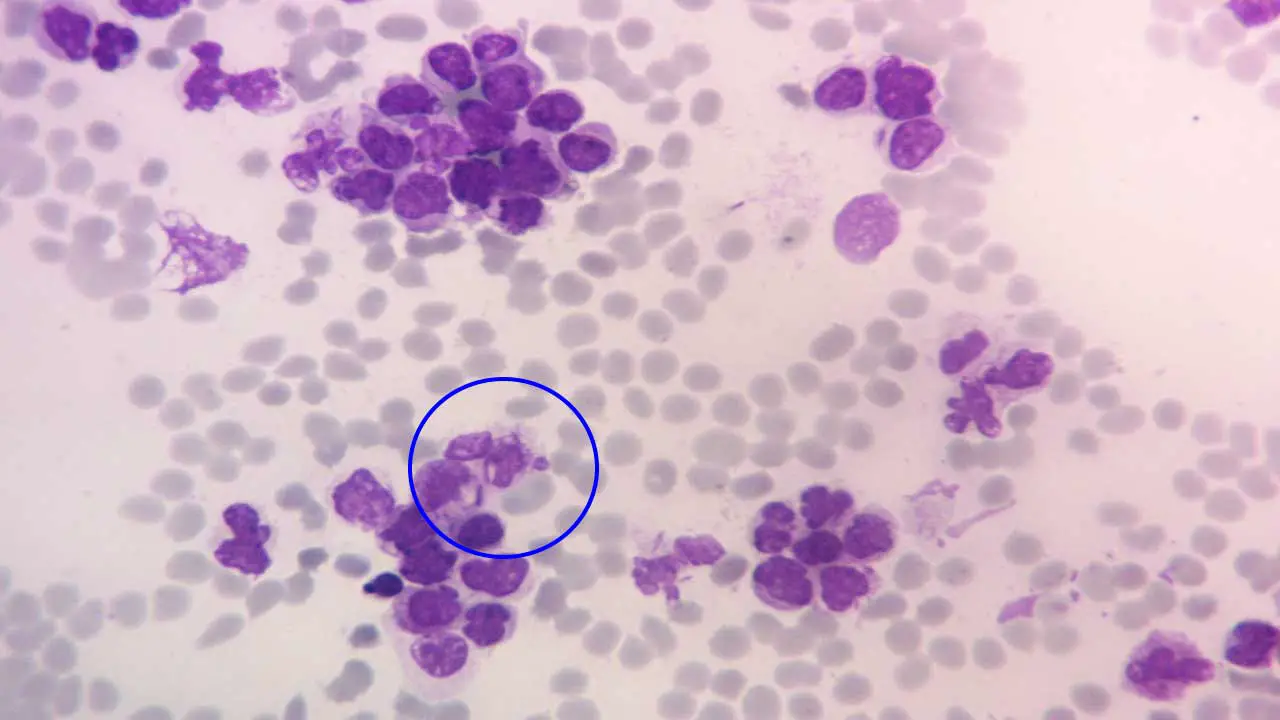
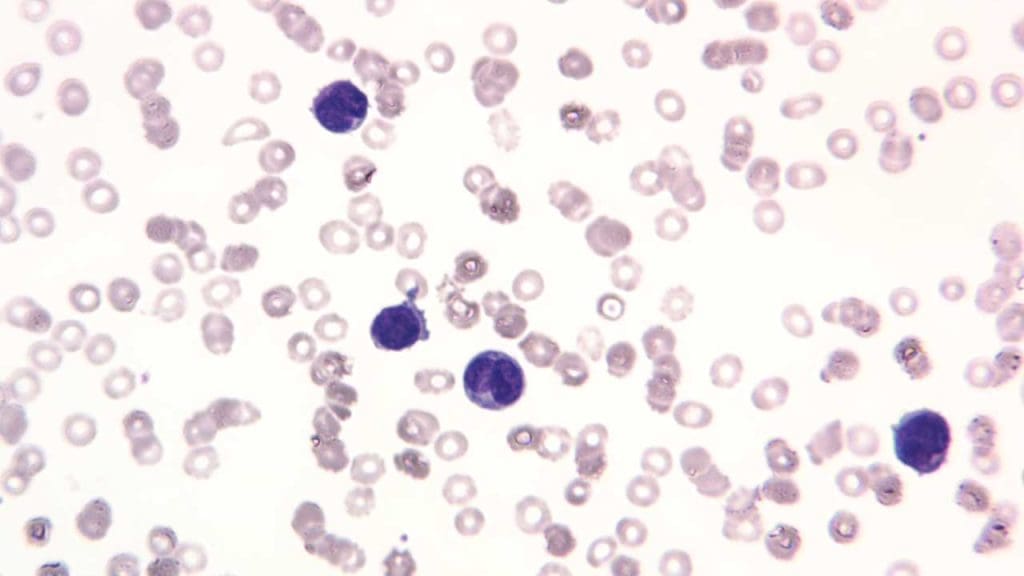
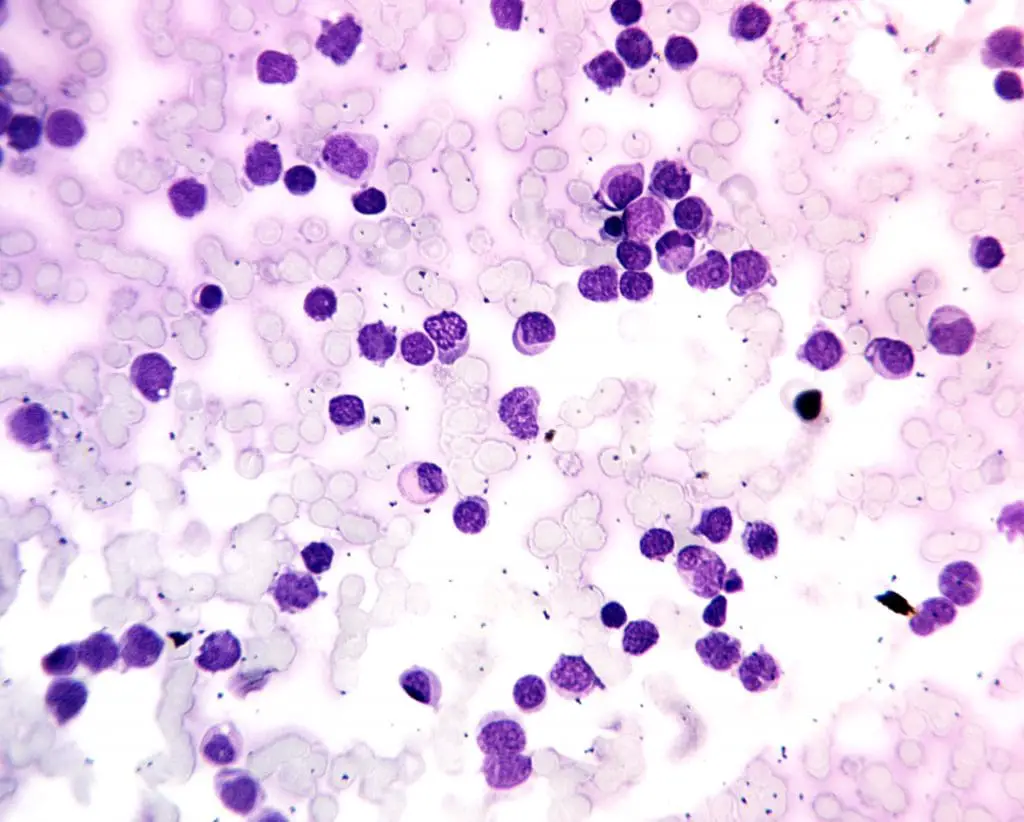
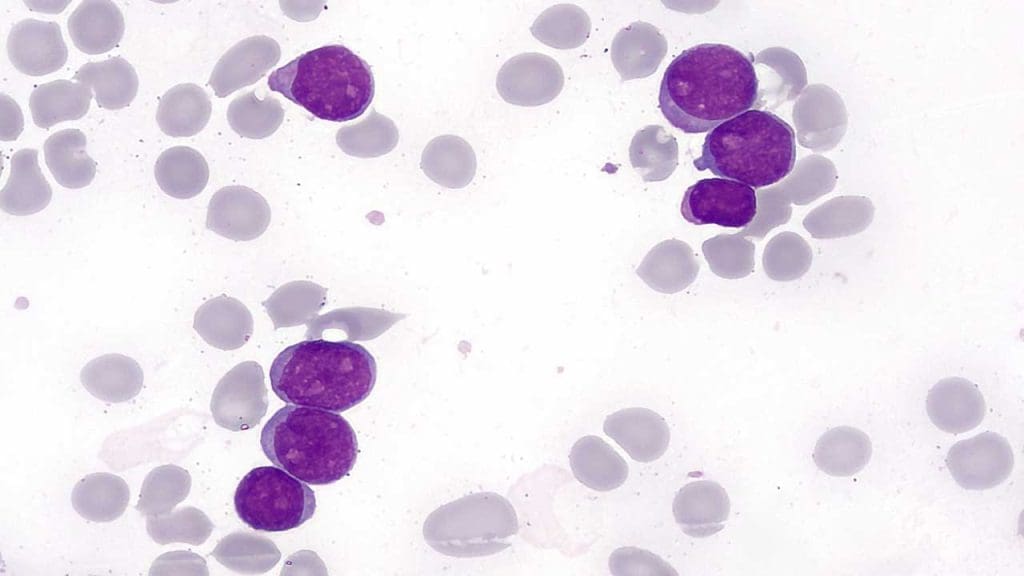
Peripheral Blood: The First Look
A complete blood count (CBC) usually shows pancytopenia. The white-cell count is unpredictable: it can be low, normal, or extreme (>100,000/µL).
The peripheral blood smear typically shows circulating myeloblasts: large cells with a high nuclear-to-cytoplasmic ratio and prominent nucleoli. The pathognomonic finding is the Auer rod, a needle-like pink inclusion in the cytoplasm. If you see Auer rods, you are looking at a myeloid leukemia.
Bone Marrow Studies: The Confirmation
Marrow aspiration and trephine biopsy remain the gold standard. The marrow is usually hypercellular and, by traditional WHO criteria, contains ≥20% blasts. Cytochemical stains such as myeloperoxidase (MPO) or Sudan Black B confirm myeloid lineage and help distinguish AML from acute lymphoblastic leukemia (ALL).
Flow Cytometry (Immunophenotyping)
This laser-based test reads the proteins on each blast's surface, giving the leukemia an "ID badge." AML blasts typically express CD13, CD33, CD117, and MPO, while lacking lymphoid markers like CD3 and CD19.
Cytogenetics and FISH
Cytogenetics looks at the chromosomes themselves.
- Favorable findings: t(8;21), inv(16), t(15;17) (the latter defines APL).
- Adverse findings: loss of chromosome 5 or 7 (-5, -7) and complex karyotypes.
Molecular Testing: Next-Generation Sequencing (NGS)
NGS reads the DNA letter by letter and is now indispensable.
- FLT3-ITD: aggressive disease, high relapse risk; targetable with midostaurin or quizartinib [8,9].
- NPM1: generally favorable when FLT3 is wild-type; now also targetable with revumenib in the relapsed setting [7].
- IDH1/IDH2: targeted by ivosidenib, olutasidenib, and enasidenib.
- TP53: the most adverse mutation; remains an unmet need.
While a bone marrow biopsy remains the gold standard, high-sensitivity NGS on peripheral blood is becoming a highly reliable, fast alternative. In older, frail patients or when a marrow aspiration results in a "dry tap," peripheral blood molecular testing is heavily relied upon to rapidly identify targetable mutations (such as FLT3 or IDH1/2) so treatment can begin without delay.
Diagnostic Criteria at a Glance
| Investigation | Key Expected Finding in AML |
|---|---|
| Morphology | ≥20% blasts; Auer rods |
| Flow Cytometry | CD13+, CD33+, CD117+, MPO+ |
| Cytogenetics | Recurrent translocations (e.g., t(8;21), inv(16), t(15;17)) |
| Molecular (NGS) | NPM1, FLT3, IDH1/2, DNMT3A, TP53 mutations |
A lumbar puncture is added when central nervous system involvement is suspected, and CT or PET imaging when extramedullary disease (e.g., myeloid sarcoma) is on the differential.
WHO 2022 Classification of AML
The 5th Edition of the WHO Classification of Haematolymphoid Tumours (2022) marks the most significant shift in AML nomenclature in a generation [2]. It moves the field from a morphology-led system to a genetics-led one.
A parallel framework, the International Consensus Classification (ICC) 2022, was published in the same year. The two largely agree but differ on a few points, including the blast threshold for myelodysplasia-related AML and how to handle TP53-mutated disease [3].
AML with Defining Genetic Abnormalities
Under WHO 2022, certain genetic findings are diagnostic of AML regardless of blast percentage (with two exceptions: BCR::ABL1 and CEBPA, which still require ≥20%).
- Established entities: t(8;21) (RUNX1::RUNX1T1), inv(16), t(15;17) (APL with PML::RARA).
- Newer entities: KMT2A rearrangement (formerly MLL), MECOM rearrangement, NUP98 rearrangement.
- NPM1 mutation: AML can be diagnosed below 20% blasts.
- CEBPA mutation: requires in-frame bZIP variants.
AML Defined by Differentiation
This category replaces "AML, NOS" and is reserved for cases lacking the defining genetic findings above. The ≥20% blast threshold still applies, and subtypes are still based on appearance (minimal differentiation, without maturation, with maturation, myelomonocytic, monocytic, basophilic, and pure erythroid).
AML, Myelodysplasia-Related (AML-MR)
This category replaces "AML with myelodysplasia-related changes." Diagnosis no longer requires a prior MDS history; instead, AML-MR is defined by a specific set of mutations (ASXL1, BCOR, EZH2, SF3B1, SRSF2, STAG2, U2AF1, ZRSR2) or characteristic cytogenetic findings such as complex karyotypes or -7 [2].
Blast Threshold Summary
The FAB Classification: A Historical Map
The French-American-British (FAB) system, developed in the 1970s, was the first widely adopted AML classification. It split AML into morphological subtypes M0 to M7 based on what cells look like under the microscope and how they stain. Although WHO has largely replaced it, the FAB language survives at the bedside ("This looks like an M5") and helps trainees connect appearance to underlying biology.
FAB Subtypes in Brief
- M0 — minimally differentiated AML. Blasts lack clear maturation; cytochemistry (MPO, Sudan Black B) is negative; CD13+, CD33+.
- M1 — without maturation. Blasts may show Auer rods; MPO+, CD13+, CD33+, CD117+.
- M2 — with maturation. Maturing neutrophils plus blasts; often carries t(8;21).
- M3 — acute promyelocytic leukemia (APL). Hypergranular promyelocytes, "buttock" cells with bilobed nuclei; CD13+, CD33+, HLA-DR–, CD34–. A medical emergency due to DIC risk.
- M4 — myelomonocytic. Mixed myeloid and monocytic cells; high WBC counts.
- M5 — monocytic. Subdivided into M5a (monoblastic) and M5b (monocytic). Most common AML in younger adults; often shows gingival infiltration.
- M6 — erythroleukemia. Dysplastic erythroid precursors dominate; reclassified under WHO 2022 as pure erythroid leukemia.
- M7 — megakaryocytic. Megakaryoblasts with platelet-membrane antigens (CD41, CD42b, CD61); strongly associated with Down syndrome in young children.
Limitations of FAB Classification
FAB relied on morphology alone, which is inherently subjective and ignored the genetic drivers we now know matter most for prognosis and treatment. It could not distinguish AMLs with very different outcomes, which is why WHO supplanted it from 2001 onward.
Mapping FAB to WHO 2022
Treatment and Management of AML
AML treatment is no longer one-size-fits-all. Therapy is shaped by two questions: what does the genetic profile look like, and how fit is the patient?
Risk Stratification First
Before starting therapy, rapid NGS is essential. The European LeukemiaNet (ELN) 2022 recommendations sort patients into Favorable, Intermediate, and Adverse risk groups based on cytogenetics and mutations [1].
| ELN 2022 Risk | Representative Findings |
|---|---|
| Favorable | t(8;21); inv(16); NPM1-mutated without FLT3-ITD; in-frame bZIP CEBPA |
| Intermediate | NPM1-mutated with FLT3-ITD; NPM1-wildtype with FLT3-ITD; t(9;11); other findings not classified elsewhere |
| Adverse | -5, -7; complex or monosomal karyotype; TP53 mutation; ASXL1, BCOR, EZH2, RUNX1, SF3B1, SRSF2, STAG2, U2AF1, or ZRSR2 mutations; KMT2A rearrangement (most partners) |
TP53-mutated AML
This is currently the most challenging subgroup. Response rates to standard therapy are low, and newer agents have failed to improve outcomes. Notably, the clinical development program for magrolimab (an anti-CD47 immunotherapy) was permanently discontinued by the FDA and the sponsor in early 2024 due to increased patient mortality and futility [11]. Allogeneic transplant in first remission remains the usual recommendation for fit patients.
Phase I: Induction Therapy
The goal of induction is complete remission (CR): <5% blasts in the marrow with recovered counts.
A. Intensive induction ("7+3" backbone). Fit, younger patients receive 7 days of cytarabine plus 3 days of an anthracycline (usually daunorubicin). The backbone is now augmented by mutation status [1,8,9]:
- FLT3-mutated AML: add midostaurin (RATIFY trial) [8] or quizartinib (QuANTUM-First, frontline approval July 2023) [9].
- CD33-positive AML: add gemtuzumab ozogamicin, an antibody-drug conjugate.
- Therapy-related or AML-MR in fit older patients: substitute CPX-351 (Vyxeos), a liposomal cytarabine-daunorubicin formulation.
B. Non-intensive induction (VenAza). For patients ≥75 or those with significant comorbidities, venetoclax (a BCL-2 inhibitor) plus a hypomethylating agent (azacitidine or decitabine) is the standard. The VIALE-A trial showed this combination produces response rates approaching intensive chemotherapy [5]. However, because the regimen causes profound myelosuppression, modern practice requires an early bone marrow evaluation (e.g., Day 14 or 21 of Cycle 1). If the marrow is cleared of leukemia, the venetoclax duration in subsequent cycles is frequently reduced from 28 days to 14 or 7 days to allow normal blood counts to recover.
C. Acute promyelocytic leukemia (APL). APL is treated as a separate disease. The standard of care is the chemotherapy-free regimen of all-trans retinoic acid (ATRA) plus arsenic trioxide (ATO), which cures more than 95% of low-to-intermediate-risk patients [6]. Differentiation syndrome and DIC are the main early hazards.
Targeted Therapies
Specific oral inhibitors are increasingly used both upfront and at relapse.
- FLT3 inhibitors: Gilteritinib is the established, FDA-approved standard of care for relapsed or refractory FLT3-mutated AML, given as a highly potent, single-agent oral therapy based on the ADMIRAL trial [12].
- IDH inhibitors: Ivosidenib (IDH1, including frontline with azacitidine in unfit patients), olutasidenib (IDH1, R/R), and enasidenib (IDH2, R/R). They release the differentiation block in mutated cells.
- Menin inhibitors: Revumenib was approved for relapsed/refractory AML with KMT2A rearrangements and NPM1 mutations [7]. Furthermore, ziftomenib, another oral menin inhibitor, has shown remarkable efficacy and manageable toxicity specifically in heavily pretreated NPM1-mutated and KMT2A-rearranged AML in the KOMET-001 trial [13].
Phase II: Consolidation and Maintenance
Once CR is reached, consolidation is needed to clear measurable residual disease (MRD).
- High-dose cytarabine (HiDAC): standard for favorable-risk patients.
- Allogeneic stem cell transplant (allo-HCT): the definitive curative option for intermediate- and adverse-risk patients fit enough to tolerate it. Benefits come both from high-dose conditioning and from the donor immune cells' graft-versus-leukemia effect.
- Maintenance with oral azacitidine (CC-486): Standard for patients who achieved complete remission following intensive chemotherapy but are not candidates for a stem cell transplant, extending overall survival [1].
- Post-transplant targeted maintenance: It is now standard practice to administer targeted therapies following an allogeneic stem cell transplant to prevent relapse. Most notably, the MORPHO trial demonstrated that post-transplant maintenance with the FLT3 inhibitor gilteritinib significantly improves relapse-free survival in patients who have detectable FLT3-ITD measurable residual disease (MRD) [14].
Supportive Care: Treating the Side Effects
Managing complications is as important as the chemotherapy itself.
Tumor lysis syndrome (TLS). Aggressive IV hydration (around 3 L/m²/day) and allopurinol for prophylaxis; rasburicase for high-risk patients. Venetoclax carries a notoriously high risk for TLS; therefore, a strict "dose ramp-up" schedule and close laboratory monitoring are mandatory during the first week of treatment.
Differentiation syndrome. A potentially fatal complication of ATRA, ATO, IDH inhibitors, and menin inhibitors. Watch for fever, weight gain, breathlessness, and pulmonary infiltrates. Start dexamethasone 10 mg twice daily at the first suspicion. Do not wait for confirmation [6].
Neutropenic sepsis. Empirical broad-spectrum antibiotics within an hour. Patients and caregivers should treat any fever ≥38.0 °C as an emergency.
Monitoring: The Role of MRD
Modern AML management is MRD-driven [1]. Sensitive techniques can detect 1 leukemia cell in 10,000 to 1,000,000 — far below what a microscope can see. The morphologic CR is only the tip of the iceberg; MRD reveals the rest.
- MRD-negative correlates with significantly longer survival.
- MRD-positive after induction is a warning that the leukemia will likely return; it often triggers a switch in therapy or escalation to transplant before clinical relapse.
- MRD status increasingly dictates the intensity of transplant conditioning. An MRD-positive patient will typically require a myeloablative (heavy) conditioning regimen to clear the residual disease prior to transplant, whereas an MRD-negative patient may safely receive a reduced-intensity conditioning regimen, sparing them significant toxicity [15].
Living With AML
For families supporting a patient through induction, three practical themes come up over and over.
Infection prevention. During the neutropenic window (typically days 7–21 after induction), even a single fever above 38.0 °C is treated as an emergency. Keep a thermometer at home, encourage hand hygiene, avoid sick contacts, and ask the team about food safety (no raw fish, soft cheeses, or unwashed produce in some centers).
Mouth and skin care. Mucositis is one of the most uncomfortable side effects of intensive chemotherapy. Soft toothbrushes, alcohol-free rinses, and reporting mouth pain early all help.
Conversations to have early. Fertility preservation should be discussed before induction in younger patients. So should psychological support, return-to-work timelines for survivors, and goals of care for older or frailer patients facing high-risk disease.
Frequently Asked Questions (FAQs)
What is the life expectancy of someone with acute myeloid leukemia?
According to the National Cancer Institute SEER program, the 5-year relative survival rate for AML is approximately 32%, and roughly 22,010 new cases are estimated in the United States in 2025 [10]. Survival depends heavily on age and genetics: young adults with favorable-risk AML can have long-term survival above 60%, while patients over 70 or those with TP53 mutations remain in the single digits.
Is AML curable?
Around 60–70% of fit adults achieve complete remission after induction. Among those, more than a quarter survive at least three years and many are functionally cured, particularly if they reach allogeneic transplant in first remission. APL, treated with ATRA and arsenic trioxide, has cure rates above 95% [6].
What causes AML?
Most AML arises from acquired DNA changes in a single bone marrow stem cell that accumulate over a lifetime — often starting silently as CHIP. Risk factors include smoking, benzene exposure, prior chemotherapy or radiation, pre-existing MDS or MPN, and inherited conditions like Down syndrome, Fanconi anemia, and RUNX1 or DDX41 germline mutations. In most patients, no single cause is found.
What are the warning signs of leukemia?
The most common signs reflect bone marrow failure: persistent fatigue, recurrent or unusually severe infections, easy bruising and bleeding, unexplained fevers, weight loss, breathlessness, pale skin, and, less commonly, bone pain or swollen lymph nodes. None of these is specific, but their combination over a few weeks should prompt a complete blood count.
Does AML have stages?
AML does not use a TNM staging system because it does not form solid tumors. Clinicians describe it instead as untreated, in active disease, in complete remission, MRD-positive or MRD-negative, or relapsed.
Can AML be diagnosed without a bone marrow biopsy?
Sometimes the peripheral blood is so abnormal that AML is obvious on a smear, but a bone marrow biopsy is still required for the cytogenetic and molecular workup that drives risk stratification and treatment choice [1,2].
What is the role of stem cell transplant?
Allogeneic stem cell transplant is typically used during consolidation for intermediate- and adverse-risk AML in patients fit enough to tolerate it. It works through both high-dose conditioning and the donor immune system's graft-versus-leukemia effect [1].
Glossary of Related Medical Terms
- Auer rods: Pink, needle-shaped clumps inside leukemia cells; almost specific to AML.
- Blast: An immature, non-functional young blood cell. Normally rare in blood; piles up in AML.
- CHIP (clonal hematopoiesis of indeterminate potential): An age-related state in which a single mutated stem cell produces a clone of identical blood cells. Often a silent first step toward AML.
- Complete remission (CR): Less than 5% blasts in the marrow with recovered blood counts.
- Cytogenetics: Lab analysis of chromosome structure (translocations, deletions).
- Differentiation arrest: AML's hallmark — cells stop maturing and stay as blasts.
- ELN (European LeukemiaNet): International expert group whose guidelines define AML risk groups and treatment recommendations.
- Flow cytometry: Laser-based test that reads the proteins on a cell's surface, giving each leukemia an "ID badge."
- Leukostasis: Emergency in which blasts are so numerous they sludge in lung and brain vessels.
- Measurable residual disease (MRD): Tiny amounts of leukemia detectable below the microscope's limit; the best modern predictor of relapse.
- Menin inhibitor: New oral drug class (revumenib) that releases the differentiation block in NPM1- and KMT2A-driven AML.
- Neutropenic sepsis: Bloodstream infection in a patient with very low neutrophils. Fever may be the only warning.
- Pancytopenia: Low red cells, white cells, and platelets together.
- Tumor lysis syndrome (TLS): Metabolic emergency caused by rapid cancer cell death.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Döhner, H., Wei, A. H., Appelbaum, F. R., Craddock, C., DiNardo, C. D., Dombret, H., Ebert, B. L., Fenaux, P., Godley, L. A., Hasserjian, R. P., Larson, R. A., Levine, R. L., Miyazaki, Y., Niederwieser, D., Ossenkoppele, G., Röllig, C., Sierra, J., Stein, E. M., Tallman, M. S., Tien, H. F., … Löwenberg, B. (2022). Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood, 140(12), 1345–1377. https://doi.org/10.1182/blood.2022016867
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Kantarjian, H., Kadia, T., DiNardo, C., Daver, N., Borthakur, G., Jabbour, E., Garcia-Manero, G., Konopleva, M., & Ravandi, F. (2021). Acute myeloid leukemia: current progress and future directions. Blood cancer journal, 11(2), 41. https://doi.org/10.1038/s41408-021-00425-3
- DiNardo, C. D., Jonas, B. A., Pullarkat, V., Thirman, M. J., Garcia, J. S., Wei, A. H., Konopleva, M., Döhner, H., Letai, A., Fenaux, P., Koller, E., Havelange, V., Leber, B., Esteve, J., Wang, J., Pejsa, V., Hájek, R., Porkka, K., Illés, Á., Lavie, D., … Pratz, K. W. (2020). Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. The New England journal of medicine, 383(7), 617–629. https://doi.org/10.1056/NEJMoa2012971
- Lo-Coco, F., Avvisati, G., Vignetti, M., Thiede, C., Orlando, S. M., Iacobelli, S., Ferrara, F., Fazi, P., Cicconi, L., Di Bona, E., Specchia, G., Sica, S., Divona, M., Levis, A., Fiedler, W., Cerqui, E., Breccia, M., Fioritoni, G., Salih, H. R., Cazzola, M., … Study Alliance Leukemia (2013). Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. The New England journal of medicine, 369(2), 111–121. https://doi.org/10.1056/NEJMoa1300874
- Issa, G. C., Aldoss, I., Thirman, M. J., DiPersio, J., Arellano, M., Blachly, J. S., Mannis, G. N., Perl, A., Dickens, D. S., McMahon, C. M., Traer, E., Zwaan, C. M., Grove, C. S., Stone, R., Shami, P. J., Mantzaris, I., Greenwood, M., Shukla, N., Cuglievan, B., Kovacsovics, T., … Stein, E. M. (2025). Menin Inhibition With Revumenib for KMT2A-Rearranged Relapsed or Refractory Acute Leukemia (AUGMENT-101). Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 43(1), 75–84. https://doi.org/10.1200/JCO.24.00826
- Stone, R. M., Mandrekar, S. J., Sanford, B. L., Laumann, K., Geyer, S., Bloomfield, C. D., Thiede, C., Prior, T. W., Döhner, K., Marcucci, G., Lo-Coco, F., Klisovic, R. B., Wei, A., Sierra, J., Sanz, M. A., Brandwein, J. M., de Witte, T., Niederwieser, D., Appelbaum, F. R., Medeiros, B. C., … Döhner, H. (2017). Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. The New England journal of medicine, 377(5), 454–464. https://doi.org/10.1056/NEJMoa1614359
- Erba, H. P., Montesinos, P., Kim, H. J., Patkowska, E., Vrhovac, R., Žák, P., Wang, P. N., Mitov, T., Hanyok, J., Kamel, Y. M., Rohrbach, J. E. C., Liu, L., Benzohra, A., Lesegretain, A., Cortes, J., Perl, A. E., Sekeres, M. A., Dombret, H., Amadori, S., Wang, J., … QuANTUM-First Study Group (2023). Quizartinib plus chemotherapy in newly diagnosed patients with FLT3-internal-tandem-duplication-positive acute myeloid leukaemia (QuANTUM-First): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet (London, England), 401(10388), 1571–1583. https://doi.org/10.1016/S0140-6736(23)00464-6
- National Cancer Institute. (2025). Cancer stat facts: Leukemia — Acute myeloid leukemia (AML). Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/statfacts/html/amyl.html
- Gilead Sciences. (2024, February 15). Gilead Statement on Magrolimab Studies in Solid Tumors [Press release]. (Follows the 2023 discontinuation of the ENHANCE Phase 3 trials in MDS and AML due to futility). https://www.gilead.com/company/company-statements/2024/gilead-statement-on-magrolimab-studies-in-solid-tumors
- Perl, A. E., Martinelli, G., Cortes, J. E., Neubauer, A., Berman, E., Paolini, S., Montesinos, P., Baer, M. R., Larson, R. A., Ustun, C., Fabbiano, F., Erba, H. P., Di Stasi, A., Stuart, R., Olin, R., Kasner, M., Ciceri, F., Chou, W. C., Podoltsev, N., Recher, C., … Levis, M. J. (2019). Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. The New England journal of medicine, 381(18), 1728–1740. https://doi.org/10.1056/NEJMoa1902688
- Wang, E. S., Issa, G. C., Erba, H. P., Altman, J. K., Montesinos, P., DeBotton, S., Walter, R. B., Pettit, K., Savona, M. R., Shah, M. V., Kremyanskaya, M., Baer, M. R., Foran, J. M., Schiller, G., Adès, L., Heiblig, M., Berthon, C., Peterlin, P., Rodríguez-Arbolí, E., Salamero, O., … Fathi, A. T. (2024). Ziftomenib in relapsed or refractory acute myeloid leukaemia (KOMET-001): a multicentre, open-label, multi-cohort, phase 1 trial. The Lancet. Oncology, 25(10), 1310–1324. https://doi.org/10.1016/S1470-2045(24)00386-3
- Levis, M. J., Hamadani, M., Logan, B., Jones, R. J., Singh, A. K., Litzow, M., Wingard, J. R., Papadopoulos, E. B., Perl, A. E., Soiffer, R. J., Ustun, C., Ueda Oshima, M., Uy, G. L., Waller, E. K., Vasu, S., Solh, M., Mishra, A., Muffly, L., Kim, H. J., Mikesch, J. H., … BMT-CTN 1506/MORPHO Study Investigators (2024). Gilteritinib as Post-Transplant Maintenance for AML With Internal Tandem Duplication Mutation of FLT3. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 42(15), 1766–1775. https://doi.org/10.1200/JCO.23.02474
- Hourigan, C. S., Dillon, L. W., Gui, G., Logan, B. R., Fei, M., Ghannam, J., Li, Y., Licon, A., Alyea, E. P., Bashey, A., Deeg, H. J., Devine, S. M., Fernandez, H. F., Giralt, S., Hamadani, M., Howard, A., Maziarz, R. T., Porter, D. L., Scott, B. L., Warlick, E. D., … Horwitz, M. E. (2020). Impact of Conditioning Intensity of Allogeneic Transplantation for Acute Myeloid Leukemia With Genomic Evidence of Residual Disease. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 38(12), 1273–1283. https://doi.org/10.1200/JCO.19.03011


