Key Takeaways
DVT is a blood clot that forms in a deep vein, usually in the calf or thigh. Left untreated, it can travel to the lungs and cause a life-threatening pulmonary embolism (PE).
- Causes ▾: Three forces drive DVT — vessel wall injury, slow blood flow, and a clot-prone state. This is Virchow's triad.
- Symptoms ▾: Pain, swelling, redness, warmth in the affected leg due to blood clot in the leg (may be absent).
- Diagnosis ▾: The Wells' score guides diagnosis. Patients unlikely to have a DVT can often be cleared with a D-dimer; those likely to have one go straight to compression ultrasound [1,7]
- Treatment ▾: DOACs are now first-line treatment for most adults with DVT [1]. Warfarin and heparins are reserved for specific scenarios such as mechanical heart valves, pregnancy, and antiphospholipid syndrome.
- Prevention ▾: Prevention matters at every stage — early walking after surgery, hydration on long trips, weight management, and not smoking all reduce DVT risk.
*Click ▾ for more information
Introduction
Deep vein thrombosis, commonly shortened to DVT, is one of the most clinically important diagnoses you will meet in hematology and on hospital wards. A clot lodged in a deep leg vein may seem straightforward, but it sits at the crossroads of three major specialties, the internal medicine, surgery, and emergency care because of one outcome it can cause: pulmonary embolism. Together, DVT and PE form venous thromboembolism (VTE).
VTE affects roughly 1 to 2 people per 1,000 each year in developed countries, totaling around 300,000 to 600,000 events annually in the United States [2]. Risk climbs steeply with age, surgery, immobility, cancer, pregnancy, and inherited clotting disorders. This guide walks you through DVT from pathophysiology to current evidence-based management, with an emphasis on what an undergraduate student or informed caregiver actually needs to know.
Pathophysiology of DVT
Virchow's Triad
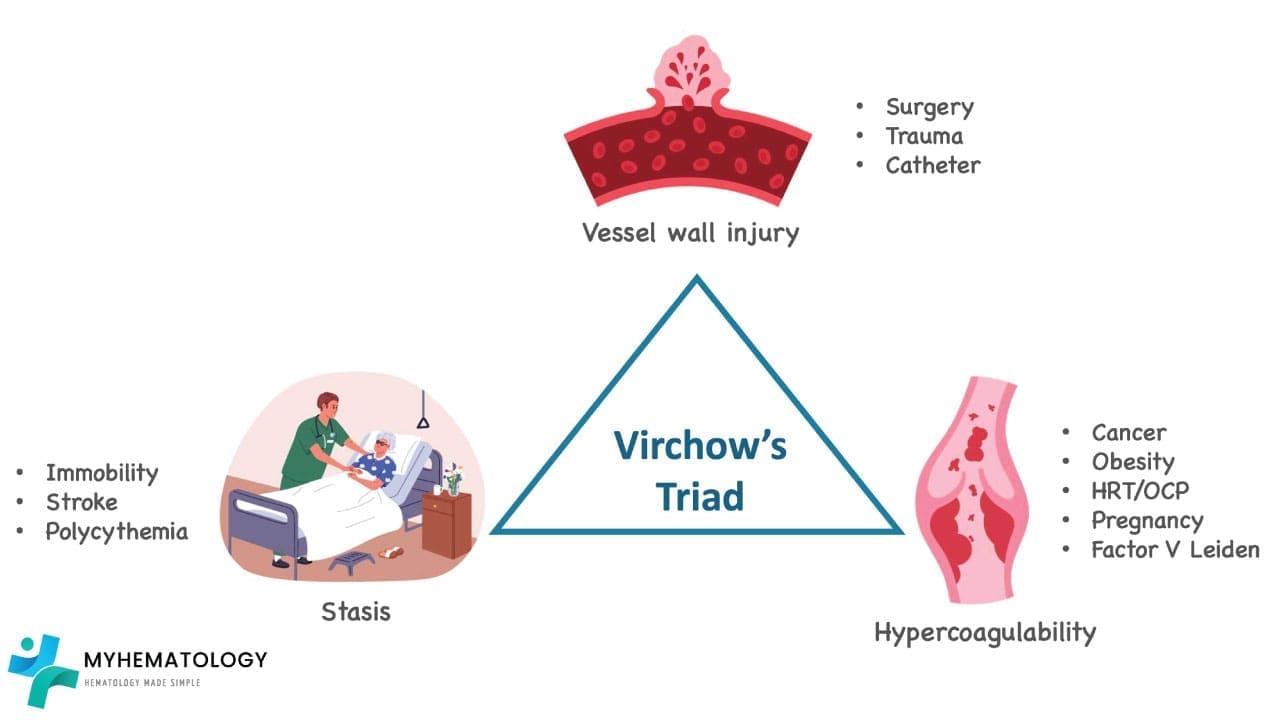
In 1856, Rudolf Virchow described the three forces that, alone or in combination, set the stage for venous clotting. They still anchor every modern textbook.
1. Endothelial injury. The endothelium is the smooth, single-cell lining of every blood vessel. A healthy endothelium actively prevents clotting. Damage from surgery, trauma, an indwelling catheter, or chronic inflammation exposes pro-thrombotic tissue underneath, kicking off the coagulation cascade.
2. Stasis (slow blood flow). When blood pools, clotting factors accumulate locally, oxygen drops, and the clotting balance tips toward thrombus formation. Common triggers include long-haul flights, post-operative bed rest, congestive heart failure, and external compression from tight clothing.
3. Hypercoagulability. Some people clot more readily than others. This may be inherited for example Factor V Leiden, prothrombin gene mutation, or deficiencies of antithrombin, protein C, or protein S or acquired through cancer, pregnancy, oral contraceptives, hormone therapy, or antiphospholipid syndrome.
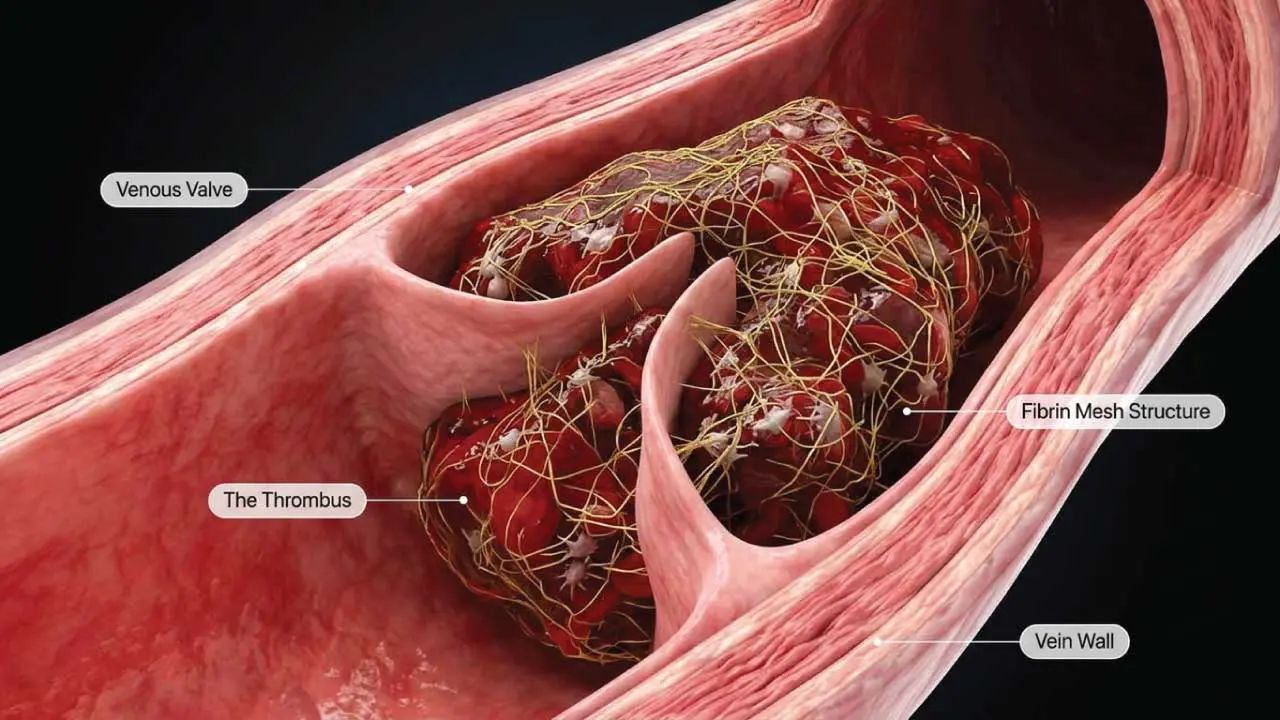
When these three factors coincide, the body's natural anticoagulant defenses are overwhelmed, and a fibrin-rich clot forms in the low-pressure pockets of deep veins, especially behind valve cusps.
Mechanism of DVT

Most DVTs begin in the calf veins. They can stay there or extend (propagate) upward into the popliteal, femoral, or iliac veins. This anatomy matters clinically:
- Distal DVT — clot below the popliteal vein. Less likely to cause PE on its own but can extend.
- Proximal DVT — clot in or above the popliteal vein. Higher PE risk and always treated with anticoagulation.
Less commonly, DVT occurs in the upper limbs (often catheter-related), the splanchnic veins, the cerebral venous sinuses, or the portal vein. Each location carries its own risk-factor profile and presentation.
Risk Factors
Non-Modifiable
- Age — risk rises sharply after 60.
- Genetics — Factor V Leiden, prothrombin gene mutation, deficiencies of protein C, protein S, or antithrombin.
- Underlying conditions — active cancer, inflammatory bowel disease, heart failure, antiphospholipid syndrome.
- Anatomical variants — May-Thurner syndrome (left iliac vein compression) and Paget-Schroetter syndrome (effort-induced upper-limb DVT).
Modifiable
- Recent surgery (especially orthopedic, abdominal, or pelvic) and prolonged immobility.
- Pregnancy and the postpartum period.
- Estrogen-containing contraceptives and hormone replacement therapy.
- Obesity, smoking, and dehydration.
- Long-haul travel of 6 hours or more.
The presence of one risk factor does not guarantee a DVT will form. The risk multiplies when several stack together.
Clinical Presentation of Deep Vein Thrombosis
Classic Signs
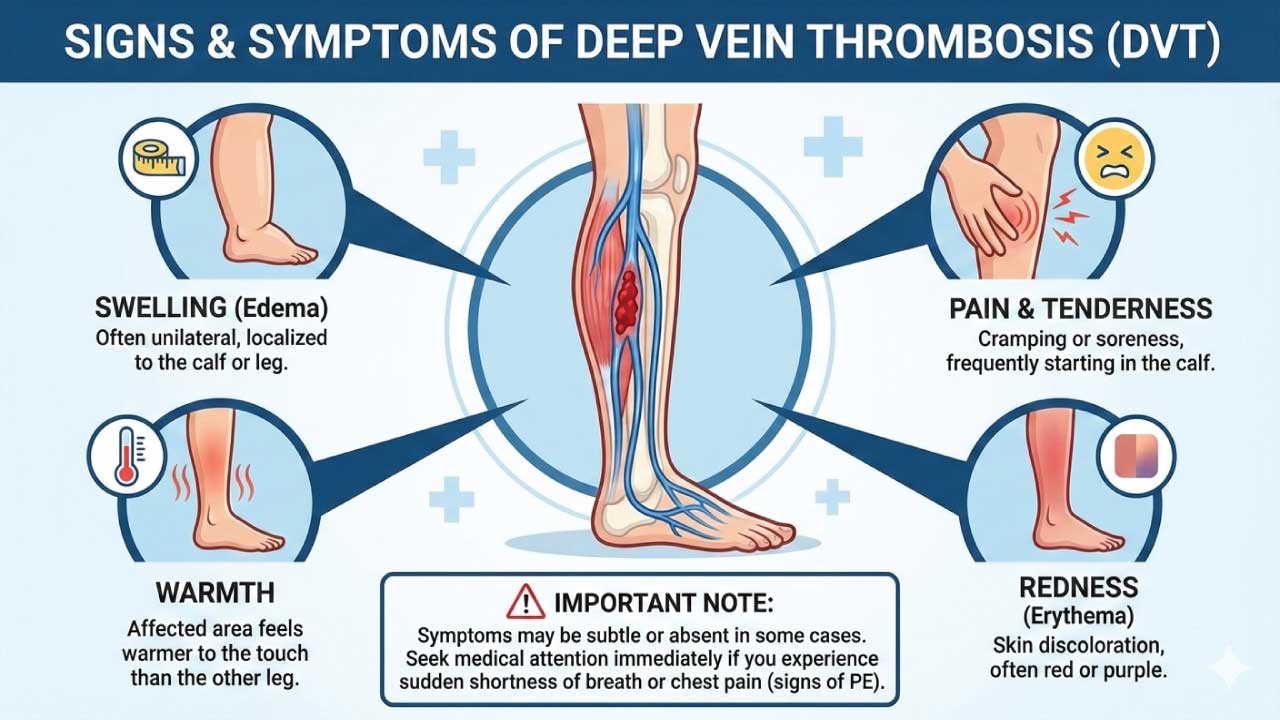
The textbook leg DVT presents with:
- Pain — usually a deep aching or throbbing in the calf or thigh, often worse with standing or walking.
- Unilateral swelling — one leg looks visibly larger than the other.
- Warmth over the affected area.
- Redness or skin discoloration, especially on lighter skin tones.
- Tenderness along the deep venous tract.

Atypical and Silent Presentations
Up to 30% of DVTs are clinically silent. Others present in ways that can throw clinicians off:
- Isolated calf pain mimicking a muscle strain.
- Swelling without pain (more common in older adults or in diabetes, where pain perception is dulled).
- Skin changes alone — a brownish hue or a non-healing ulcer.
- Upper-limb DVT presenting only as arm heaviness or hand discoloration.
The take-home point: maintain a high index of suspicion in anyone with risk factors and unilateral leg symptoms, even when the picture is incomplete.
Red Flags for Pulmonary Embolism
If a patient with possible DVT develops sudden shortness of breath, sharp chest pain that worsens with breathing, coughing up blood, a racing heart, or fainting, they need emergency evaluation. PE is the single most dangerous complication of DVT.
Differential Diagnosis
Several conditions mimic DVT and must be considered:
- Musculoskeletal — muscle strain or tear, tendonitis, ruptured Baker's cyst.
- Other vascular — superficial thrombophlebitis, varicose veins, lymphedema, peripheral artery disease.
- Skin and soft tissue — cellulitis, abscess.
- Trauma — fracture, hematoma.
- Other — lipedema, congestive heart failure with bilateral edema.
A unilateral, progressive leg swelling in a patient with risk factors should always prompt DVT testing.
Diagnosis of DVT
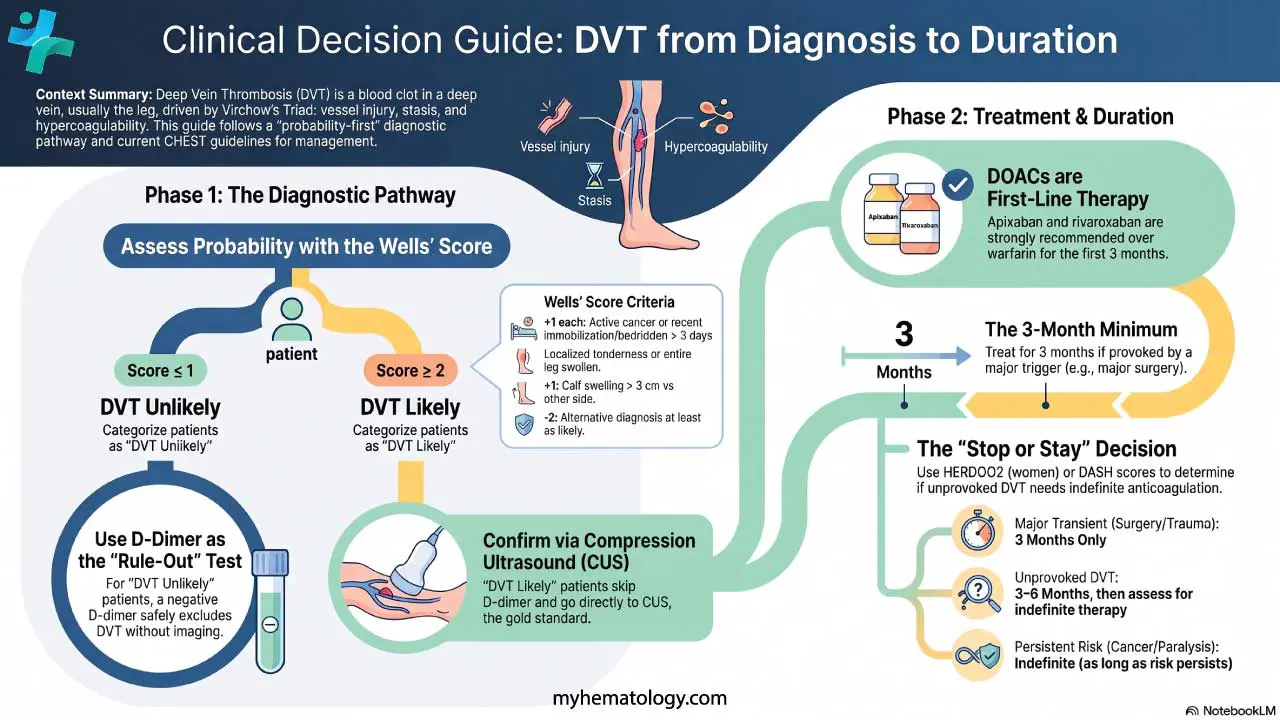
The goal is to confirm or exclude DVT efficiently, balancing sensitivity (don't miss a clot) with specificity (don't anticoagulate someone who doesn't need it). Modern practice follows a "probability-first" pathway [1,7].
Step 1: Calculate the Wells' Score
The Wells' Score for DVT calculator can be accessed here.
| Clinical feature | Points |
|---|---|
| Active cancer (treatment ongoing, within 6 months, or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of the lower extremity | +1 |
| Recently bedridden > 3 days, or major surgery within 12 weeks | +1 |
| Localized tenderness along the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling ≥ 3 cm vs. the other side (measured 10 cm below the tibial tuberosity) | +1 |
| Pitting edema confined to the symptomatic leg | +1 |
| Collateral non-varicose superficial veins | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely | −2 |
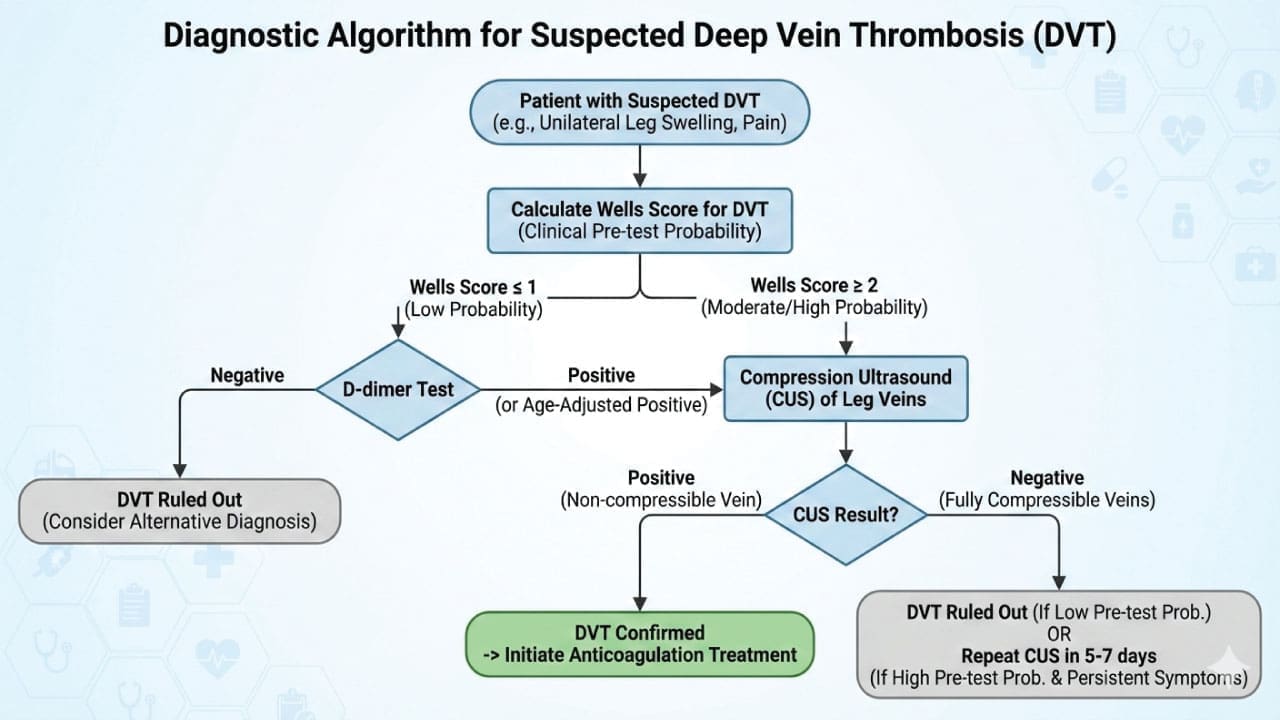
Two-level interpretation:
- Score ≤ 1 → DVT unlikely → check D-dimer first.
- Score ≥ 2 → DVT likely → go straight to compression ultrasound.
Step 2: D-Dimer (the "Rule-Out" Test)
D-dimer is a fibrin breakdown product. It is highly sensitive but not specific as many conditions raise it (infection, surgery, pregnancy, cancer). Its strength is its negative predictive value: a normal D-dimer in a low-probability patient effectively rules out DVT. Additionally, modern diagnostic protocols adjust the D-dimer threshold based on clinical probability. Algorithms like the YEARS criteria allow for a higher D-dimer cutoff (e.g., 1000 µg/L) to safely rule out venous thromboembolism in patients who lack specific high-risk clinical features, significantly reducing unnecessary ultrasounds [9].
Age-adjusted cutoff
For patients over 50, an age-adjusted cutoff (age × 10 µg/L) reduces false positives without missing clots [7].
Step 3: Compression Ultrasound (CUS)
CUS is the gold standard non-invasive test. The key finding is a vein that fails to compress under probe pressure where it normally would.
- Positive CUS → DVT confirmed; start anticoagulation.
- Negative CUS in a "DVT likely" patient → don't fully exclude DVT. Repeat in 5–7 days, or perform a whole-leg ultrasound that includes the calf veins.
When to Look Beyond Ultrasound
- Suspected pelvic or iliac DVT with massive whole-limb swelling but a normal CUS → CT or MR venography.
- Upper-extremity suspicion → duplex ultrasound of the subclavian and axillary veins. The Wells' score is for lower limbs only.
Treatment and Management of DVT
General Principles
The goals of DVT therapy are to stop clot growth, prevent PE, reduce recurrence, and limit long-term complications like PTS. Most patients with uncomplicated DVT can be treated at home rather than admitted [2]. Hospitalization is reserved for severe DVT, hemodynamic instability, high bleeding risk, or social barriers to outpatient care.
Anticoagulation: The Mainstay
The 2021 CHEST guideline gives a strong recommendation for direct oral anticoagulants (DOACs) over warfarin for the first 3 months of treatment in most adults with DVT or PE [1].
DOACs (apixaban, rivaroxaban, edoxaban, dabigatran) — first-line for most patients. Oral, fixed-dose, no routine monitoring, fewer dietary and drug interactions.
Low-molecular-weight heparin (LMWH; e.g., enoxaparin, dalteparin) — preferred during pregnancy, in many patients with cancer (although DOACs are now also acceptable for many CAT patients [1,8]), and as a bridge when starting warfarin.
Unfractionated heparin (UFH) — used IV when rapid action and reversibility are needed (e.g., in patients with severe renal failure or before invasive procedures).
Warfarin — still essential for patients with mechanical heart valves and antiphospholipid syndrome (APS). DOACs are actively contraindicated in APS (especially in triple-positive patients) due to unacceptably high rates of recurrent arterial and venous thrombosis on DOAC therapy [10]. Warfarin requires INR monitoring (target 2.0–3.0) and "bridging" with a heparin during initiation, since warfarin transiently lowers proteins C and S before its full effect.
Comparison: DOACs vs. Warfarin vs. Heparin
| Feature | DOACs | Warfarin | Heparin (UFH/LMWH) |
|---|---|---|---|
| Mechanism | Direct factor Xa or thrombin inhibition | Vitamin K antagonist (factors II, VII, IX, X) | Activates antithrombin |
| Route | Oral | Oral | IV (UFH) or subcutaneous (LMWH) |
| Onset | Hours | 3–5 days | Immediate (IV) / hours (SC) |
| Monitoring | Not routinely needed | PT/INR | aPTT (UFH) or anti-Xa (LMWH) |
| Reversal | Andexanet alfa (Xa) or idarucizumab (IIa) | Vitamin K, 4-factor PCC | Protamine sulfate |
| Diet/drug interactions | Minimal | Significant | Few |
| First-line for | Most adult VTE | Mechanical valves, APS | Acute VTE in hospital, pregnancy |
Distal vs. Proximal DVT
A practical update many older articles miss: for isolated distal (calf) DVT without severe symptoms or high-risk features, current guidance suggests serial ultrasound for 2 weeks instead of immediate anticoagulation [1]. However, immediate anticoagulation is required if the patient has high-risk features for clot extension, such as active cancer, a prior history of VTE, an unprovoked clot, or a thrombus located close to the popliteal vein [1]. If managed conservatively with serial imaging and the clot extends, treatment begins. If it stays put or resolves, anticoagulation is avoided altogether.
Catheter-Directed Thrombolysis and Mechanical Treatments
Most patients do not need clot removal. Catheter-directed thrombolysis is reserved for:
- Phlegmasia cerulea dolens — a limb-threatening DVT with massive swelling and cyanosis.
- Severe iliofemoral DVT in young, low-bleeding-risk patients with significant symptoms.
IVC filters are placed only when anticoagulation is contraindicated, typically because of active bleeding. Retrievable filters are strongly preferred and should be removed when anticoagulation can resume.
Compression Stockings: An Important Update
The article you may have read elsewhere likely treats graduated compression stockings as a routine PTS prevention tool. Following the SOX trial [6], the 2021 CHEST guideline now suggests against routine use of compression stockings to prevent PTS [1]. Stockings remain reasonable for symptomatic relief for swelling, heaviness, aching but they should be offered for symptoms, not as automatic PTS prophylaxis.
Special Populations
- Pregnancy — LMWH is the agent of choice. Warfarin is teratogenic in the first trimester. DOACs are avoided because they cross the placenta and have insufficient safety data.
- Cancer-associated thrombosis — oral factor Xa inhibitors (apixaban, edoxaban, rivaroxaban) are first-line for most patients [1,8]. However, because DOACs carry a statistically significant increased risk of major mucosal bleeding in certain malignancies, LMWH remains the preferred agent specifically for patients with intact luminal gastrointestinal (GI) or genitourinary (GU) cancers [11].
- Severe renal impairment — DOACs need dose adjustment or are avoided; warfarin or UFH may be preferred.
- Pediatric VTE — guided by separate ASH/ISTH recommendations [3]. Two major recent shifts include the approval and integration of DOACs (specifically rivaroxaban and dabigatran) into pediatric care, and a shortened anticoagulation duration of just 6 weeks for select children with a provoked VTE [12].
Provoked Vs Unprovoked DVT
The single most useful classification when deciding how long to anticoagulate is whether the DVT was provoked.
Provoked by a major transient factor (surgery > 30 minutes under general anesthesia, major trauma, hospitalization > 3 days for acute illness): 3 months of anticoagulation is enough. Annual recurrence after stopping is roughly 1% [5].
Provoked by a minor transient factor (pregnancy/postpartum, hormone use, long-haul travel, minor leg injury): typically 3 months, with shared decision-making about extension.
Unprovoked DVT: roughly 10% recurrence in the first year and 30% within five years after stopping anticoagulation [5]. These patients are often candidates for indefinite anticoagulation, provided their bleeding risk is acceptable.
Persistent provocations (active cancer, chronic inflammatory disease, permanent paralysis): treat as long as the risk factor persists.
For unprovoked VTE patients who cannot or choose not to continue anticoagulation, low-dose aspirin is a reasonable secondary-prevention option (it is less effective than anticoagulation, but better than nothing) [1].
Tools to Help the "Stop or Stay" Decision
- HERDOO2 rule (women only, score 0–1 → safe to stop): Hyperpigmentation, Edema, or Redness of either leg; D-dimer ≥ 250 µg/L on therapy; Obesity (BMI ≥ 30); Older age (≥ 65). Men with unprovoked VTE are considered high recurrence risk by default.
- DASH score — measured 1 month after stopping anticoagulation, using D-dimer, age, sex, and hormone use.
These are decision aids, not algorithms. The final decisions rest on the patient's bleeding risk and preferences.
The Clinical Decision Guide: DVT from Diagnosis to Duration
Phase 1: Diagnosis (The Wells’ Pathway)
Goal: Determine if the patient has a clot right now.
- Assess Pre-Test Probability: Apply the Wells’ Score.
- Low/Unlikely (Score < 2): Order a high-sensitivity D-dimer.
- Negative: DVT excluded.
- Positive: Proceed to Compression Ultrasound (CUS).
- High/Likely (Score ≥ 2): Skip D-dimer; proceed directly to Compression Ultrasound.
- Low/Unlikely (Score < 2): Order a high-sensitivity D-dimer.
- Verify via Imaging:
- If CUS is positive: Diagnosis confirmed.
- If CUS is negative but clinical suspicion remains high: Repeat CUS in 5–7 days.
Phase 2: Initial Treatment (The 3-Month Minimum)
Goal: Prevent immediate extension or Pulmonary Embolism (PE).
- Provoked (Major Trigger): Treat for 3 months only.
- Unprovoked or Persistent Risk: Treat for 3–6 months, then reassess using recurrence scores.
- Choice of Agent: DOACs (Apixaban/Rivaroxaban) are first-line for most; Warfarin for mechanical valves/APS; LMWH for pregnancy.
Phase 3: Extended Therapy (The "Stop or Stay" Decision)
Goal: Balance the 10% annual recurrence risk of unprovoked DVT against the 1–2% major bleeding risk of anticoagulants.
Tool 1: HERDOO2 (The Women’s Rule)
Best used 5–12 months into therapy while the patient is still on medication.
- Criteria: Post-thrombotic signs (Hyperpigmentation-Edema-Redness), D-dimer ≥ 250 µg/L, Obesity, Age ≥ 65.
- Result: * Score 0–1 (Women): Low risk --> Stop therapy.
- Score ≥ 2 (Women): High risk --> Stay on therapy.
- Men: Always considered high risk; stay on therapy.
Tool 2: DASH Score (The Gender-Neutral Rule)
Best used by measuring D-dimer 1 month after stopping anticoagulation.
- Criteria: Abnormal D-dimer (+2), Age ≤ 50 (+1), Male (+1), Hormone use (-2).
- Result:
- Score ≤ 1: Low risk --> Keep therapy off.
- Score ≥ 2: High risk --> Restart indefinite therapy.
Complications and Prognosis
Pulmonary Embolism (PE)
The most dangerous complication. A clot fragments off the leg vein, travels through the right heart, and lodges in the pulmonary arteries. Symptoms include sudden dyspnea, pleuritic chest pain, hemoptysis, syncope, and tachycardia. Untreated PE can be fatal; with prompt treatment, most patients recover well.
Post-Thrombotic Syndrome (PTS)
PTS develops in roughly 20–50% of DVT patients, depending on definition, and reflects damage to the venous valves and persistent venous hypertension. Symptoms include chronic leg pain, swelling, skin pigmentation, and in severe cases, venous ulcers. Risk is higher with proximal DVT, recurrent ipsilateral DVT, and obesity.
Chronic Venous Insufficiency
A long-term consequence of valvular damage marked by persistent edema, varicose veins, skin changes, and reduced quality of life.
Prognosis
With prompt diagnosis and modern anticoagulation, all-cause 3-month mortality after a treated DVT is around 3–6%, with most deaths driven by underlying conditions like cancer rather than DVT itself. PE carries higher short-term mortality but still responds well to early treatment.
DVT Preventive Strategies
Prevention is multi-layered.

Pharmacological Prophylaxis
Used in hospitalized patients at increased risk (post-surgery, acutely ill medical patients, cancer, pregnancy with prior VTE). Common agents:
- LMWH — workhorse of inpatient prophylaxis.
- DOACs (apixaban, rivaroxaban) — increasingly used after major orthopedic surgery and for extended outpatient prophylaxis.
- Unfractionated heparin — used when LMWH is contraindicated or in severe renal failure.
The choice depends on the procedure, bleeding risk, and renal function.
Mechanical Measures
- Intermittent pneumatic compression devices in hospital, especially when bleeding risk prevents pharmacological prophylaxis.
- Graduated compression stockings — for symptom relief and selected high-risk situations like long-haul travel.
- Early ambulation after surgery is one of the simplest and most effective preventive measures.
Patient-Level Measures
- Maintain a healthy weight.
- Stay hydrated, especially on flights longer than 4–6 hours.
- Avoid smoking.
- On long journeys, walk every hour, do calf exercises in your seat, and consider compression socks if you have risk factors.
- Manage chronic conditions (heart failure, diabetes, hypertension) actively.
- After surgery, follow your team's mobilization plan.
Thrombophilia Testing
Routine thrombophilia testing after every unprovoked DVT is not recommended. Testing rarely changes the duration of treatment in the average patient and can cause anxiety and insurance issues. Consider it selectively for example in young patients, those with a strong family history, or unusual clot locations
Frequently Asked Questions (FAQs)
What is deep vein thrombosis?
DVT is a blood clot that forms inside one of the deep veins of the body, most often in the calf or thigh. It can block normal blood return and, more dangerously, break loose and travel to the lungs as a pulmonary embolism. The recognized causes group neatly under Virchow's triad of vessel injury, slow blood flow, and a clot-prone state.
What are the warning signs of a leg clot?
Look for pain or aching in one calf or thigh, swelling on one side, warmth, redness, and tenderness. Up to 30% of cases are silent, so anyone with risk factors who develops new unilateral leg symptoms should be evaluated promptly. If sudden breathlessness, chest pain, or fainting follows, treat it as a possible pulmonary embolism and seek emergency care.
How is DVT diagnosed?
Doctors first calculate a Wells' score from your history and exam. A "DVT unlikely" score combined with a normal D-dimer effectively rules out a clot. A "DVT likely" score sends you straight to a compression ultrasound, which is the gold standard test. CT or MR venography is used when iliac or pelvic clots are suspected [1,7].
How long do you need to take blood thinners after a DVT?
For most adults with a clot triggered by a clear, temporary cause (like recent surgery), 3 months of anticoagulation is enough. For unprovoked clots or those linked to ongoing risks like cancer, treatment often continues longer, sometimes indefinitely, balanced against the risk of bleeding [1,5].
Are DOACs better than warfarin for DVT?
For most adults with DVT, DOACs (apixaban, rivaroxaban, edoxaban, dabigatran) are now first-line and are strongly recommended over warfarin in the 2021 CHEST guideline [1]. They work as well, cause less serious bleeding, do not require INR monitoring, and have far fewer food interactions. Warfarin remains preferred in mechanical heart valves and antiphospholipid syndrome.
How can I prevent DVT during a long flight or after surgery?
On flights and long drives, walk and flex your calves every hour, stay hydrated, and avoid alcohol and tight clothing. After surgery, follow your team's mobilization plan and take any prescribed prophylactic injections or DOACs exactly as directed. People with prior DVT, active cancer, or pregnancy should ask their doctor about extra precautions before travel or surgery [1,2].
Glossary of Related Medical Terms
- Anticoagulant — a medication that slows clotting (e.g., DOACs, warfarin, heparin).
- D-dimer — a fibrin breakdown product; a normal level helps rule out DVT in low-risk patients.
- DOAC (Direct Oral Anticoagulant) — newer oral blood thinners (apixaban, rivaroxaban, edoxaban, dabigatran) that block specific clotting factors and don't need routine monitoring.
- Distal DVT — a clot in the calf veins, below the popliteal vein.
- Endothelium — the inner lining of blood vessels; healthy endothelium prevents clotting, damaged endothelium triggers it.
- Heparin (UFH and LMWH) — injected anticoagulants. UFH is given IV; LMWH (e.g., enoxaparin) is given subcutaneously.
- Hypercoagulability — increased clotting tendency, inherited or acquired.
- IVC filter — a mesh device placed in the inferior vena cava to catch clots when anticoagulation isn't possible.
- May-Thurner syndrome — compression of the left iliac vein by the right iliac artery, predisposing to left-leg DVT.
- Phlegmasia cerulea dolens — a severe, limb-threatening DVT with massive swelling and bluish skin.
- Post-thrombotic syndrome (PTS) — a chronic complication of DVT marked by leg pain, swelling, skin changes, and sometimes ulcers.
- Proximal DVT — a clot in the popliteal vein or higher; always treated with anticoagulation.
- Pulmonary embolism (PE) — a clot lodged in the lung's blood supply; the most dangerous complication of DVT.
- Thrombolysis — the use of clot-dissolving drugs; reserved for severe cases.
- Venous thromboembolism (VTE) — collective term for DVT and PE.
- Virchow's triad — the three drivers of clotting: vessel injury, stasis, hypercoagulability.
- Wells' score — a clinical tool for estimating the pre-test probability of DVT.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Stevens, S. M., Woller, S. C., Kreuziger, L. B., Bounameaux, H., Doerschug, K., Geersing, G. J., Huisman, M. V., Kearon, C., King, C. S., Knighton, A. J., Lake, E., Murin, S., Vintch, J. R. E., Wells, P. S., & Moores, L. K. (2021). Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest, 160(6), e545–e608. https://doi.org/10.1016/j.chest.2021.07.055
- Ortel, T. L., Neumann, I., Ageno, W., Beyth, R., Clark, N. P., Cuker, A., Hutten, B. A., Jaff, M. R., Manja, V., Schulman, S., Thurston, C., Vedantham, S., Verhamme, P., Witt, D. M., D Florez, I., Izcovich, A., Nieuwlaat, R., Ross, S., J Schünemann, H., Wiercioch, W., … Zhang, Y. (2020). American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood advances, 4(19), 4693–4738. https://doi.org/10.1182/bloodadvances.2020001830
- Monagle, P., Azzam, M., Bercovitz, R., Betensky, M., Bhat, R., Biss, T., Branchford, B., Brandão, L. R., Chan, A. K. C., Faustino, E. V. S., Jaffray, J., Jones, S., Kawtharany, H., Kerlin, B. A., Kucine, N., Kumar, R., Male, C., Pelland-Marcotte, M. C., Raffini, L., Raulji, C., … Mustafa, R. A. (2025). American Society of Hematology/International Society on Thrombosis and Haemostasis 2024 updated guidelines for treatment of venous thromboembolism in pediatric patients. Blood advances, 9(10), 2587–2636. https://doi.org/10.1182/bloodadvances.2024015328
- Wells, P. S., Anderson, D. R., Rodger, M., Forgie, M., Kearon, C., Dreyer, J., Kovacs, G., Mitchell, M., Lewandowski, B., & Kovacs, M. J. (2003). Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. The New England journal of medicine, 349(13), 1227–1235. https://doi.org/10.1056/NEJMoa023153
- Kearon, C., Ageno, W., Cannegieter, S. C., Cosmi, B., Geersing, G. J., Kyrle, P. A., & Subcommittees on Control of Anticoagulation, and Predictive and Diagnostic Variables in Thrombotic Disease (2016). Categorization of patients as having provoked or unprovoked venous thromboembolism: guidance from the SSC of ISTH. Journal of thrombosis and haemostasis : JTH, 14(7), 1480–1483. https://doi.org/10.1111/jth.13336
- Kahn, S. R., Shapiro, S., Wells, P. S., Rodger, M. A., Kovacs, M. J., Anderson, D. R., Tagalakis, V., Houweling, A. H., Ducruet, T., Holcroft, C., Johri, M., Solymoss, S., Miron, M. J., Yeo, E., Smith, R., Schulman, S., Kassis, J., Kearon, C., Chagnon, I., Wong, T., … SOX trial investigators (2014). Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial. Lancet (London, England), 383(9920), 880–888. https://doi.org/10.1016/S0140-6736(13)61902-9
- Kearon, C., de Wit, K., Parpia, S., et al. (2022). Diagnosis of deep vein thrombosis with D-dimer adjusted to clinical probability: Prospective diagnostic management study. BMJ, 376, e067378. https://doi.org/10.1136/bmj-2021-067378
- Agnelli, G., Becattini, C., Meyer, G., Muñoz, A., Huisman, M. V., Connors, J. M., Cohen, A., Bauersachs, R., Brenner, B., Torbicki, A., Sueiro, M. R., Lambert, C., Gussoni, G., Campanini, M., Fontanella, A., Vescovo, G., Verso, M., & Caravaggio Investigators (2020). Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. The New England journal of medicine, 382(17), 1599–1607. https://doi.org/10.1056/NEJMoa1915103
- van der Hulle, T., Cheung, W. Y., Kooij, S., Beenen, L. F. M., van Bemmel, T., van Es, J., Faber, L. M., Hazelaar, G. M., Heringhaus, C., Hofstee, H., Hovens, M. M. C., Kaasjager, K. A. H., van Klink, R. C. J., Kruip, M. J. H. A., Loeffen, R. F., Mairuhu, A. T. A., Middeldorp, S., Nijkeuter, M., van der Pol, L. M., Schol-Gelok, S., … YEARS study group (2017). Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet (London, England), 390(10091), 289–297. https://doi.org/10.1016/S0140-6736(17)30885-1
- Pengo, V., Denas, G., Zoppellaro, G., Jose, S. P., Hoxha, A., Ruffatti, A., Andreoli, L., Tincani, A., Cenci, C., Prisco, D., Fierro, T., Gresele, P., Cafolla, A., De Micheli, V., Ghirarduzzi, A., Tosetto, A., Falanga, A., Martinelli, I., Testa, S., Barcellona, D., … Banzato, A. (2018). Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood, 132(13), 1365–1371. https://doi.org/10.1182/blood-2018-04-848333
- Key, N. S., Khorana, A. A., Kuderer, N. M., Bohlke, K., Lee, A. Y. Y., Arcelus, J. I., Wong, S. L., Balaban, E. P., Flowers, C. R., Francis, C. W., Gates, L. E., Kakkar, A. K., Levine, M. N., Liebman, H. A., Tempero, M. A., Lyman, G. H., & Falanga, A. (2020). Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 38(5), 496–520. https://doi.org/10.1200/JCO.19.01461
- Goldenberg, N. A., Kittelson, J. M., Abshire, T. C., Bonaca, M., Casella, J. F., Dale, R. A., Halperin, J. L., Hamblin, F., Kessler, C. M., Manco-Johnson, M. J., Sidonio, R. F., Spyropoulos, A. C., Steg, P. G., Turpie, A. G. G., Schulman, S., & Kids-DOTT Trial Investigators and the ATLAS Group (2022). Effect of Anticoagulant Therapy for 6 Weeks vs 3 Months on Recurrence and Bleeding Events in Patients Younger Than 21 Years of Age With Provoked Venous Thromboembolism: The Kids-DOTT Randomized Clinical Trial. JAMA, 327(2), 129–137. https://doi.org/10.1001/jama.2021.23182


