Key Takeaways
Hypersensitivity is an exaggerated or inappropriate immune response to an antigen, which may be a harmless substance, an allergen, a self-antigen, or a pathogen, causing tissue damage instead of protection. The Gell and Coombs system sorts hypersensitivity into four types: Type I (immediate, IgE-mediated), Type II (antibody-mediated), Type III (immune complex), and Type IV (delayed, T-cell-mediated).
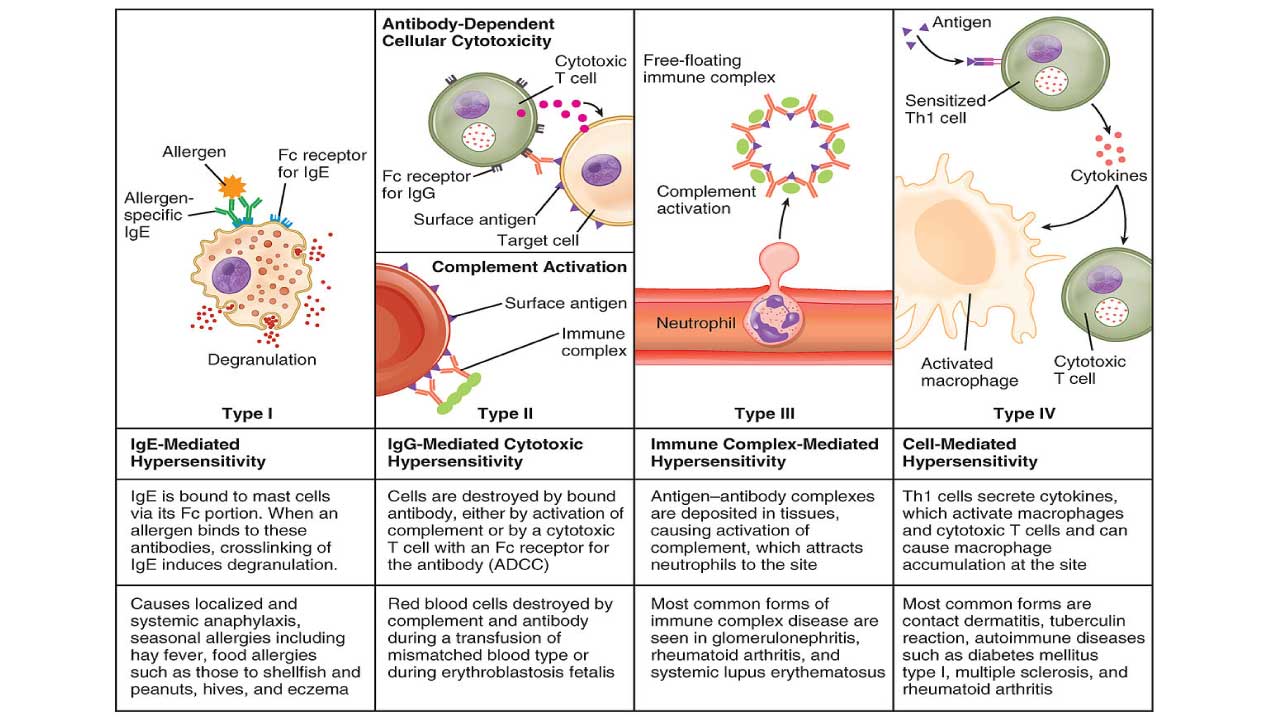
- Type I (Immediate (IgE-mediated) Hypersensitivity) ▾: This is an immediate, IgE-mediated reaction where allergen re-exposure causes mast cells and basophils to rapidly release inflammatory mediators, leading to allergic conditions or anaphylaxis.
- Type II (Antibody-mediated Hypersensitivity) ▾: This involves IgG or IgM antibodies binding directly to host cell surfaces, triggering targeted cell destruction via complement activation or phagocytosis (as seen in hemolytic reactions) or alter how they function.
- Type III (Immune Complex-mediated Hypersensitivity) ▾: This occurs when circulating antigen-antibody complexes deposit in tissues like blood vessels or kidneys, triggering complement activation and localized inflammatory damage over several hours to days.
- Type IV (Delayed-Type (Cell-mediated) Hypersensitivity) ▾: This is a delayed, antibody-independent response where sensitized T-cells release cytokines to activate macrophages, causing localized tissue damage 24 to 72 hours after antigen exposure.
*Click ▾ for more information
Introduction
Your immune system is built to protect you. Sometimes it overreacts. A hypersensitivity reaction is an exaggerated or inappropriate immune response to an antigen. That antigen isn't always a harmless substance. It can be an allergen, a self-antigen the body mistakes for foreign, or even a genuine pathogen that provokes a disproportionate response. Instead of defending the body, the response damages tissue and causes disease [1].
These reactions matter in everyday medicine. They explain why one person needs an EpiPen near peanuts, why mismatched blood is dangerous, and why a TB skin test is read two days later.
The Gell and Coombs classification is the standard framework for organizing hypersensitivity. It divides these immune responses into four types based on the mechanism involved and the speed of the reaction [5]. We will walk through each type using the same structure, so you can compare them directly.
The Two-Phase Pattern: Sensitization and Effector Phase
Before looking at the four types individually, it helps to know that all of them share the same basic timeline. The sensitization phase happens on first exposure to the antigen, when the immune system becomes primed. There are usually no symptoms during this phase; the person simply becomes "sensitized" without knowing it. The effector phase happens on a later exposure, once the primed immune response is triggered again (or, in Types II and III, once enough antibody has built up). This is when clinical symptoms and tissue damage actually appear. Keep this pattern in mind as you read each section below.
| Type | Mediator | Onset | Core mechanism | Key hematology/clinical example | Main diagnostic test |
|---|---|---|---|---|---|
| Type I | IgE | Minutes | Mast cell and basophil degranulation | Anaphylaxis, hay fever | Skin prick, specific IgE |
| Type II | IgG/IgM | Minutes–hours | Antibody binds cell-surface or membrane antigen, causing destruction or a functional change (stimulation or blockade) | Hemolytic transfusion reaction, autoimmune hemolytic anemia; Graves' disease and myasthenia gravis (functional change without destruction) | Direct/indirect Coombs test |
| Type III | IgG/IgM | Hours–weeks | Immune complexes deposit in tissue | Serum sickness, lupus | Complement levels, biopsy |
| Type IV | T cells | 24–72 hours | T-cell and macrophage inflammation | Contact dermatitis, TB skin test | Patch test, tuberculin test |
Factors Influencing Hypersensitivity Reactions
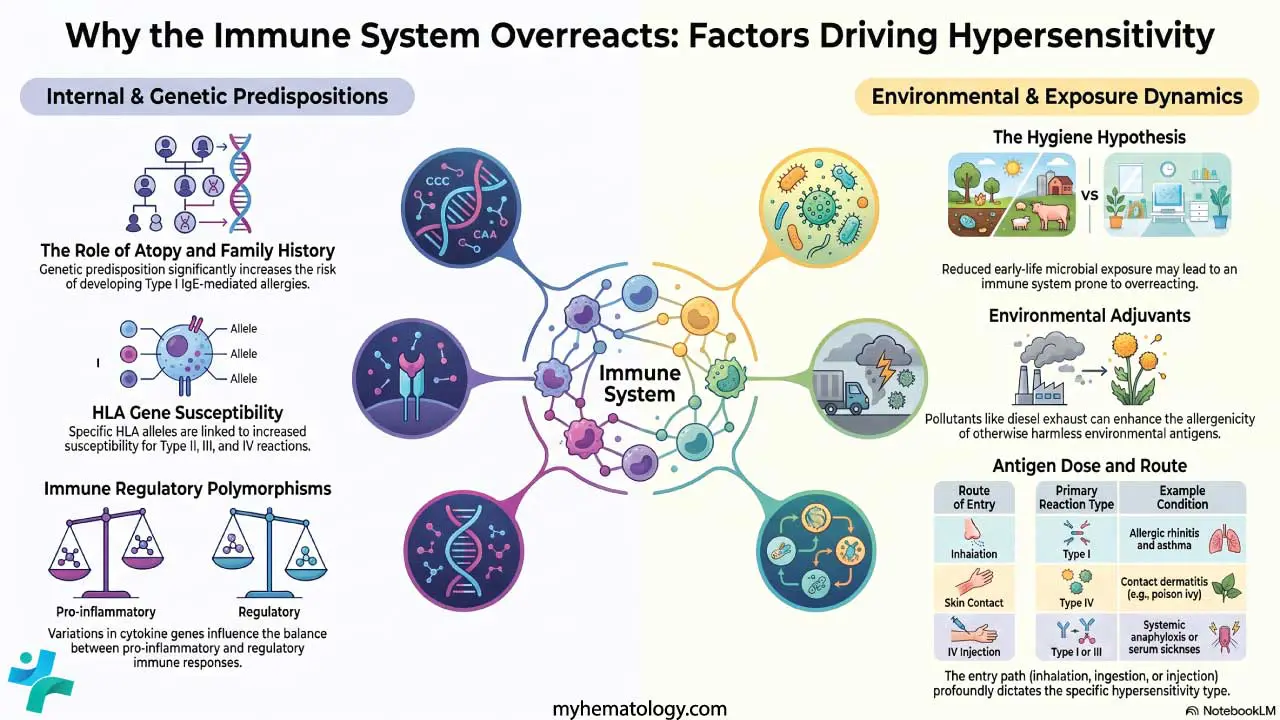
Why do some people react and others do not? Hypersensitivity is multifactorial. It arises from the interplay of a person's genes, their lifelong environmental exposures, and the nature of the antigen itself.
Genetic Predisposition
- Atopy: Atopy is an inherited tendency to develop Type I allergies. People with a family history of asthma, eczema, or hay fever are more likely to become allergic themselves. This is not simple single-gene inheritance. It is a complex trait shaped by many genes.
- HLA genes (human leukocyte antigen): For Types II, III, and IV, specific HLA alleles raise susceptibility. HLA molecules present antigens to T cells, so certain HLA types make a person more likely to mount a reaction against self-antigens (autoimmunity) or drug antigens. Specific HLA-B alleles, for example, are strongly linked to severe delayed drug reactions [4].
- Immune regulatory genes: Variations in genes for cytokines, their receptors, and signaling molecules tip the balance between inflammatory and regulatory responses. Variations affecting the Th1/Th2 balance can push someone toward allergic (Th2) or cell-mediated (Th1) reactions.
- Enzyme variations: Differences in drug-metabolizing enzymes can let reactive drug breakdown products build up. These can act as haptens, small molecules that become immunogenic after binding a body protein, and trigger a reaction.
Environmental Factors
- Allergen exposure: The type, frequency, and amount of exposure to allergens like pollen, dust mites, dander, mold, and certain foods all shape Type I risk. Early-life exposure patterns are especially influential.
- The "old friends" update to the hygiene hypothesis: The classic hygiene hypothesis proposed that fewer childhood infections leave the immune system prone to overreacting to harmless substances. Current thinking reframes this around microbial diversity. Reduced contact with a broad range of microbes, rather than cleanliness alone, appears to impair immune tolerance. The reframing is widely accepted but the original "hygiene hypothesis" label is now considered an oversimplification.
- Air pollution: Pollutants such as diesel exhaust particles and ozone act as adjuvants, boosting an antigen's allergenicity, and they irritate airways directly.
- Diet and microbiome: Researchers are studying how the timing of food introduction in infancy, food additives, and the gut and airway microbiome shape allergy risk. A disrupted microbiome can weaken immune tolerance.
- Infections and chemicals: Some infections prime the immune system toward, or away from, hypersensitivity. Occupational and environmental chemicals can act as sensitizers, especially for contact dermatitis (Type IV).
Dose and Route of Antigen Exposure
Both how much antigen enters the body and how it gets in shape the response.
Dose. High doses can sometimes induce tolerance, or instead overwhelm clearance and drive excess immune-complex formation (Type III). Low doses may not trigger a response, though repeated low doses can sensitize. Intermediate doses are often the most effective at causing sensitization.
Route. Inhaled antigens favor Type I airway reactions like allergic rhinitis and asthma. Ingested antigens cause food allergies. Skin contact is the classic route for Type IV contact dermatitis. Intravenous antigens are most likely to cause systemic reactions such as anaphylaxis or serum sickness. Repeated injection into a sensitized person can produce a localized Arthus reaction (a Type III reaction discussed later).
Adjuvants
Adjuvants are substances that increase an antigen's immunogenicity. They prolong how long an antigen lingers, stimulate innate immune cells, and boost antigen presentation. They are mainly used in vaccines, but they can also influence hypersensitivity. Some pollutants act as environmental adjuvants and promote IgE production. In allergen immunotherapy, adjuvants are being studied to nudge the immune response away from a harmful Th2 pattern toward tolerance.
Type I Hypersensitivity
Type I is the classic allergy. It is IgE-mediated and develops within minutes of exposure to an allergen [1].
Why it matters: This is the type behind hay fever, most food allergies, and anaphylaxis, the reactions encountered most often.

Causes and Allergens
Common triggers include pollen, dust mites, animal dander, foods (nuts, eggs, shellfish), insect venom, latex, and drugs such as penicillin.
Mechanism
The reaction unfolds in two phases.
Sensitization phase. The first exposure prompts B cells to make IgE antibodies. These IgE molecules coat the surface of mast cells and basophils.
Effector phase. On re-exposure, the allergen links neighboring mast cell- and basophil-bound IgE molecules together. This cross-linking triggers rapid degranulation, releasing preformed mediators that were already stored in the granules, including histamine, tryptase, and heparin. The activated cell also rapidly manufactures new mediators from its membrane lipids, chiefly prostaglandins and leukotrienes, over the following minutes to hours. Together these mediators widen blood vessels, make them leaky, tighten smooth muscle, and drive inflammation. The result is an immediate early-phase reaction and sometimes a late-phase reaction hours later as inflammatory cells move in.
Clinical Features
Local reactions include allergic rhinitis (hay fever), allergic conjunctivitis, asthma, hives (urticaria), eczema, and angioedema. The systemic emergency is anaphylaxis, a severe, potentially fatal reaction with airway swelling, breathing difficulty, low blood pressure, and shock.
Diagnosis
Diagnosis starts with clinical history and examination. Skin prick tests introduce tiny amounts of allergen to watch for a wheal-and-flare response. Specific IgE blood tests (such as ImmunoCAP) measure antibody levels to particular allergens.
Management
- Avoid the allergen wherever possible. This is the foundation.
- Epinephrine (adrenaline) is first-line for anaphylaxis. It is the only drug that reverses the life-threatening features, opening the airway and restoring blood pressure within minutes [7]. In August 2024, the FDA approved neffy, a needle-free epinephrine nasal spray delivered as a 2-milligram dose into a single nostril, for people weighing at least 66 pounds. Clinical data demonstrates that its pharmacokinetic profile specifically how quickly it enters the bloodstream and raises blood pressure is highly comparable to traditional intramuscular injections like the EpiPen, offering a highly effective option for those who fear injections [7,8,10].
- Antihistamines, corticosteroids, and bronchodilators are adjuncts. They ease secondary symptoms but do not replace epinephrine in anaphylaxis.
- Immunotherapy (desensitization) gradually exposes the patient to rising allergen doses to reduce sensitivity over time.
Type II Hypersensitivity
Type II reactions are driven by IgG or IgM antibodies that bind antigens on the surface of the body's own cells or tissue membranes such as basement membranes [2]. This binding often destroys the target cell, but not always. In some cases the antibody instead changes how the cell functions, without killing it, by overstimulating a receptor or blocking one. Because cell destruction is the most common outcome, this type has traditionally been called "cytotoxic," though that label doesn't capture the full picture.
Why it matters: This is the most hematology-relevant type. It explains transfusion reactions, hemolytic disease of the newborn, and several immune anemias, and it also explains two well-known non-hematologic diseases through a very different route: functional change rather than destruction.

Causes and Antigens
The target antigens are usually part of the cell surface (self-antigens) or foreign molecules like drugs that stick to cell membranes. Penicillin, for example, can bind red blood cells and make them targets for antibody attack.
Mechanism
Once antibody binds the cell surface, damage follows through several routes:
- Complement activation. The antibody-antigen pair switches on the classical complement pathway, building the membrane attack complex that punches holes in the cell and causes it to burst. Complement also releases anaphylatoxins (C3a, C5a) that recruit inflammatory cells and opsonins (C3b) that flag cells for engulfment.
- ADCC (antibody-dependent cell-mediated cytotoxicity). NK cells, macrophages, and eosinophils latch onto the tail of the coating antibodies and release toxic granules that kill the target.
- Opsonization and phagocytosis. Antibody and complement coat the cell, and phagocytes recognize and swallow it.
- Cellular dysfunction without destruction. Sometimes antibody doesn't destroy the cell at all. It simply jams or triggers a receptor. In Graves' disease, antibody overstimulates the thyroid-stimulating hormone receptor, driving excess thyroid hormone production. In myasthenia gravis, antibody blocks the acetylcholine receptor at the neuromuscular junction, weakening muscle contraction. Both are Type II reactions, but neither one kills the target cell.
In the modern refinement described below, these last receptor-targeting examples are reclassified as Type IIb.
Clinical Features
- Hemolytic transfusion reactions: fever, chills, back pain, hemoglobin in the urine, and kidney failure as transfused red cells are destroyed.
- Hemolytic disease of the newborn: maternal antibodies cross the placenta and destroy fetal red cells, causing anemia, jaundice, and in severe cases hydrops fetalis.
- Autoimmune hemolytic anemia: the immune system attacks its own red cells.
- Drug-induced cytopenias: low platelets or low white cells from drug-antibody complexes.
- Goodpasture's syndrome, myasthenia gravis, and Graves' disease are non-hematologic examples, with the latter two illustrating the functional-change pattern above.
Diagnosis
- Direct Coombs test (DAT): detects antibody or complement already stuck to red cells. Essential for autoimmune hemolytic anemia and hemolytic disease of the newborn.
- Indirect Coombs test (IAT): detects free antibody in serum, used for crossmatching and screening pregnant patients for anti-Rh antibodies.
- Specific autoantibody tests and biopsy with immunofluorescence confirm conditions like Goodpasture's.
Management
Stop the offending agent first. Then suppress the immune response with corticosteroids or other immunosuppressants. Plasma exchange removes circulating antibody in severe cases, and IVIg blocks phagocyte receptors to slow destruction. Supportive care includes transfusion for severe anemia and dialysis for kidney failure. Splenectomy can help in some autoimmune hemolytic anemia, since the spleen is a major site of red-cell destruction.
Type III Hypersensitivity
Type III reactions are caused by antigen-antibody immune complexes that form in the blood and then deposit in tissues, where they trigger inflammation [3].
Why it matters: The key difference from Type II is where the antibody meets its target. In Type II, antibody binds an antigen that is fixed to a cell surface or a membrane, such as a basement membrane. In Type III, antibody binds a soluble antigen while both are circulating in the blood, forming immune complexes that then lodge in small blood vessels and other tissues.

Causes and Antigens
Triggers include persistent infections (chronic hepatitis, malaria), self-antigens in autoimmune diseases such as lupus and rheumatoid arthritis, repeatedly inhaled antigens (farmer's lung), and drugs acting as haptens (serum sickness from antivenom).
Mechanism
- Immune complex formation. Soluble antigen binds IgG or IgM to form circulating complexes. Size is critical: large complexes are quickly flagged and cleared by macrophages in the spleen and liver, while small complexes remain soluble and are filtered out harmlessly by the kidneys. Intermediate-sized complexes are the most dangerous because they evade the mononuclear phagocyte system, yet are large enough to precipitate out of the blood and get trapped in the basement membranes of turbulent or high-filtration areas, like joints and glomeruli [3,11].
- Deposition. Complexes settle in small vessels and filtering membranes, especially kidney glomeruli, joint linings, and vessel walls.
- Complement activation. Deposited complexes switch on complement, releasing anaphylatoxins (C3a, C5a) that recruit neutrophils.
- Tissue damage. Neutrophils try to engulf complexes stuck to surfaces but cannot. Frustrated, they spill enzymes and reactive oxygen species into the tissue, causing inflammation, vasculitis, and necrosis.
Clinical Features
Systemic. Serum sickness is the classic example, appearing 1 to 3 weeks after a large dose of foreign protein with the triad of fever, rash, and joint pain. Lupus deposits DNA-containing complexes across many organs. Rheumatoid arthritis deposits complexes in joints. Post-streptococcal glomerulonephritis follows a strep infection with complexes in the kidney.
Localized. The Arthus reaction is a local skin reaction in an already-sensitized person, with redness, swelling, and sometimes necrosis within hours of an intradermal injection.
Diagnosis
Clinical history guides everything. Labs may show low complement (C3, C4) as it is consumed, raised ESR and CRP, and specific autoantibodies like anti-dsDNA in lupus. Biopsy with immunofluorescence reveals granular immune-complex deposits.
Management
Remove the antigen if known. Corticosteroids are the mainstay, with NSAIDs for joint pain and stronger immunosuppressants (azathioprine, cyclophosphamide, mycophenolate) for severe disease. Plasma exchange clears complexes quickly in emergencies, and biologics (TNF inhibitors, B-cell depletion) target specific autoimmune conditions. Supportive care addresses organ complications.
Type IV Hypersensitivity
Type IV stands apart. It is not antibody-mediated. Instead, T cells drive it, which is why it is delayed, typically appearing 24 to 72 hours after exposure [4].
Why it matters: This is the mechanism behind poison ivy, the TB skin test, contact dermatitis, and chronic transplant rejection.

Causes and Antigens
Triggers include intracellular pathogens (Mycobacterium tuberculosis, Mycobacterium leprae, some fungi and viruses), contact haptens (nickel, urushiol from poison ivy, chromate), self-antigens in autoimmune disease, and donor tissue antigens in transplant rejection.
Mechanism
The reaction has two phases.
Sensitization. An antigen-presenting cell such as a dendritic cell captures the antigen, processes it, and presents it to naive T cells in the lymph nodes, generating memory T cells.
Effector. On re-exposure, sensitized memory T cells activate at the site. Th1 cells release cytokines, above all interferon-gamma, which activates macrophages into aggressive inflammatory cells. CD8+ cytotoxic T cells directly kill antigen-bearing cells. The recruited macrophages cause most of the tissue damage. If the antigen persists, chronic activation walls it off into a granuloma.
Modern Refinement: The Subtypes You Should Know
The classic model treats Type IV as a single Th1/CTL process, but current immunology recognizes four subtypes [5]:
- IVa: Th1-driven with macrophage activation (granulomas, tuberculin reaction).
- IVb: Th2-driven with eosinophils (persistent asthma, some drug rashes).
- IVc: CD8+ cytotoxic T cells using perforin and granzyme B (Stevens-Johnson syndrome, toxic epidermal necrolysis).
- IVd: T-cell-driven neutrophil inflammation (acute generalized exanthematous pustulosis).
A parallel update splits Type II into IIa (cell destruction) and IIb (receptor stimulation or blockade, like Graves' disease and myasthenia gravis). More recently, the European Academy of Allergy and Clinical Immunology (EAACI) proposed an expanded 2023 classification to account for modern environmental and metabolic factors. It keeps Types I–III, broadens Type IV, and introduces three new categories: Type V (epithelial barrier defects that prime the immune system, such as a 'leaky' skin barrier in eczema), Type VI (metabolically induced immune dysregulation, often tied to obesity or microbiome shifts), and Type VII (direct cellular and inflammatory responses to environmental chemicals, bypassing traditional antigen presentation) [9].
Clinical Features
The most common form is contact dermatitis, an itchy, red, blistering rash where an allergen touched the skin. The tuberculin (Mantoux) reaction produces a hard, raised area peaking at 48 to 72 hours. Granulomatous reactions wall off persistent antigens in TB and sarcoidosis. Chronic transplant rejection and parts of Type 1 diabetes, multiple sclerosis, and Hashimoto's thyroiditis are also T-cell-driven.
Diagnosis
- Patch testing for contact dermatitis: suspected allergens stay on the skin for 48 hours, read for a delayed eczematous reaction.
- Tuberculin skin test (PPD/Mantoux) for prior TB exposure. Note that modern diagnostics increasingly rely on specific cytokine measurements, such as Interferon-Gamma Release Assays (IGRAs). IGRAs have largely replaced the TB skin test in many developed nations because they offer higher specificity and do not cross-react with the BCG vaccine [4,12].
- Biopsy showing lymphocytes and macrophages around vessels, and granulomas in chronic cases.
Management
Identify and avoid the antigen, the most effective step for contact dermatitis. Topical corticosteroids treat most contact dermatitis, with systemic steroids for severe cases. Immunosuppressants (azathioprine, cyclosporine, methotrexate) manage chronic autoimmune Type IV disease and transplant rejection, and biologics can block key cytokines. Supportive care includes wound care and symptom relief.
Frequently Asked Questions (FAQs)
What are the four types of hypersensitivity reactions?
Hypersensitivity is grouped by the Gell and Coombs system into four types. Type I is immediate, IgE-mediated allergy such as hay fever and anaphylaxis. Type II is antibody-mediated reaction to cell-surface or membrane antigen, such as hemolytic transfusion reactions. Type III is caused by immune complexes depositing in tissue, as in serum sickness and lupus. Type IV is delayed, T-cell-mediated reaction appearing 1 to 3 days later, such as poison ivy and the TB skin test.
What is the difference between a hypersensitivity reaction and an allergy?
A hypersensitivity reaction is any harmful, exaggerated, or inappropriate immune response that occurs following prior sensitization to an antigen and results in tissue damage. It covers all four types. An allergy is the narrower term, usually meaning a Type I, IgE-mediated reaction. Every allergy is a hypersensitivity reaction, but not every hypersensitivity reaction is an allergy. Lupus and contact dermatitis are hypersensitivity reactions that are not called allergies.
Why is epinephrine the first treatment for anaphylaxis?
Epinephrine is the only treatment that reverses the life-threatening features of anaphylaxis, opening the airways and supporting blood pressure within minutes. Antihistamines and steroids only ease secondary symptoms and act too slowly to save a life. In 2024 the FDA approved a needle-free epinephrine nasal spray (neffy) for people weighing at least 66 pounds.
Which hypersensitivity reactions matter most in hematology and transfusion?
Type II reactions are central to blood medicine. They explain hemolytic transfusion reactions from mismatched blood, hemolytic disease of the newborn from Rh incompatibility, autoimmune hemolytic anemia, and some drug-induced low blood counts. The direct and indirect Coombs (antiglobulin) tests detect the responsible antibodies.
Why does a Type IV reaction take days to appear?
Type IV reactions are driven by T cells rather than antibodies. After re-exposure, T cells need time to travel to the site, multiply, and recruit macrophages before visible inflammation develops, usually 24 to 72 hours. That delay is why a poison ivy rash or a positive TB skin test does not show up immediately.
What causes serum sickness?
Serum sickness is a Type III reaction to foreign proteins, historically from animal antiserum and today more often from certain antibiotics or monoclonal antibody drugs. Antigen-antibody complexes form in the blood and deposit in vessels, joints, and kidneys, causing fever, rash, and joint pain. Symptoms usually appear 1 to 3 weeks after exposure and settle once the trigger is stopped.
Glossary of Related Medical Terms
- Hypersensitivity: An exaggerated or inappropriate immune response to an antigen, causing tissue damage instead of protection.
- Antigen: Any molecule the immune system can recognize and respond to.
- Allergen: An antigen that triggers an allergic (Type I) reaction.
- Atopy: An inherited tendency to develop IgE-mediated allergies such as asthma, eczema, and hay fever.
- IgE / IgG / IgM: Classes of antibody. IgE drives allergy; IgG and IgM drive Types II and III.
- Mast cells and basophils: Immune cells loaded with histamine-filled granules that release their contents during allergic reactions.
- Degranulation: The sudden release of stored chemicals (like histamine) from these granules.
- Hapten: A molecule too small to trigger immunity alone, but which becomes immunogenic after binding a body protein (relevant to many drug reactions).
- Opsonization: Coating a cell or microbe with antibodies or complement so phagocytes can recognize and engulf it.
- Complement system: A cascade of blood proteins that helps antibodies destroy target cells, including by forming the membrane attack complex.
- Anaphylatoxins (C3a, C5a): Complement fragments that recruit inflammatory cells and trigger mast cell release.
- ADCC (antibody-dependent cell-mediated cytotoxicity): Killing of antibody-coated cells by NK cells and other effectors.
- Immune complex: A clump of antigen bound to antibody; harmful when it deposits in tissues (Type III).
- Anaphylaxis: A severe, rapid, whole-body allergic reaction that can be fatal without prompt epinephrine.
- Granuloma: A walled-off nodule of immune cells that forms when the body cannot clear a persistent antigen (Type IV).
- DAT/IAT (direct/indirect antiglobulin or Coombs test): Blood tests that detect antibodies on red cells (DAT) or in serum (IAT).
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Abbas M, Goldin J. Type I Hypersensitivity Reaction. [Updated 2025 Aug 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560561/
- Saavedra Torres JS, Goldin J. Type II Hypersensitivity Reaction. [Updated 2025 Nov 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563264/
- Saavedra Torres JS, Annamaraju P. Type III Hypersensitivity Reaction. [Updated 2025 Sep 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559122/
- Marwa K, Goldin J, Kondamudi NP. Type IV Hypersensitivity Reaction. [Updated 2025 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562228/
- Uzzaman, A., & Cho, S. H. (2012). Chapter 28: Classification of hypersensitivity reactions. Allergy and asthma proceedings, 33 Suppl 1, 96–99. https://doi.org/10.2500/aap.2012.33.3561
- Dispenza M. C. (2019). Classification of hypersensitivity reactions. Allergy and asthma proceedings, 40(6), 470–473. https://doi.org/10.2500/aap.2019.40.4274
- Golden, D. B. K., Wang, J., Waserman, S., Akin, C., Campbell, R. L., Ellis, A. K., Greenhawt, M., Lang, D. M., Ledford, D. K., Lieberman, J., Oppenheimer, J., Shaker, M. S., Wallace, D. V., Abrams, E. M., Bernstein, J. A., Chu, D. K., Horner, C. C., Rank, M. A., Stukus, D. R., Collaborators, … Wang, J. (2024). Anaphylaxis: A 2023 practice parameter update. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology, 132(2), 124–176. https://doi.org/10.1016/j.anai.2023.09.015
- Casale, T. B., Ellis, A. K., Nowak-Wegrzyn, A., Kaliner, M., Lowenthal, R., & Tanimoto, S. (2023). Pharmacokinetics/pharmacodynamics of epinephrine after single and repeat administration of neffy, EpiPen, and manual intramuscular injection. The Journal of allergy and clinical immunology, 152(6), 1587–1596. https://doi.org/10.1016/j.jaci.2023.08.007
- Jutel, M., Agache, I., Zemelka-Wiacek, M., Akdis, M., Chivato, T., Del Giacco, S., Gajdanowicz, P., Gracia, I. E., Klimek, L., Lauerma, A., Ollert, M., O'Mahony, L., Schwarze, J., Shamji, M. H., Skypala, I., Palomares, O., Pfaar, O., Torres, M. J., Bernstein, J. A., Cruz, A. A., … Akdis, C. A. (2023). Nomenclature of allergic diseases and hypersensitivity reactions: Adapted to modern needs: An EAACI position paper. Allergy, 78(11), 2851–2874. https://doi.org/10.1111/all.15889
- U.S. Food and Drug Administration (FDA). (2024, August 9). FDA Approves First Nasal Spray for Treatment of Anaphylaxis. FDA.gov.
- Kumar, V., Abbas, A. K., Aster, J. C., Debnath, J., & Das A. (2025). Robbins & Cotran Pathologic Basis of Disease (11th ed.). Elsevier.
- Centers for Disease Control and Prevention (CDC). (2024). Interferon-Gamma Release Assays (IGRAs) – Blood Tests for TB Infection. CDC.gov.