Key Takeaways
Atypical lymphocytes, also called reactive lymphocytes, are normal immune cells (mostly activated T cells) that have changed size and shape while fighting an infection. They signal an active immune response, not usually cancer.
- Common Causes ▾: The most common triggers are viral infections, including EBV (glandular fever), CMV, and COVID-19. Bacterial and parasitic infections, drug reactions, and some autoimmune diseases can also cause them.
- Key Challenge ▾: The key clinical challenge is telling benign reactive cells apart from cancerous lymphoid cells seen in some leukemias and lymphomas. This relies on a careful blood smear and, when needed, flow cytometry.
- Symptoms ▾: Symptoms reflect the underlying illness: fever, sore throat, swollen glands, fatigue, and sometimes an enlarged spleen.
- Management ▾: Most cases are self-limiting. Treatment targets the cause, and supportive care is enough for common viral infections.
*Click ▾ for more information
Introduction
What are Atypical Lymphocytes (Reactive Lymphocytes)?
Atypical lymphocytes, also known as reactive or activated lymphocytes, are lymphocytes that have changed their appearance in response to an immune signal. The word "atypical" describes how they look, not what they mean. It tells you the cell departs from the calm, resting shape of a normal lymphocyte. It does not tell you the cell is cancerous.
Most of the time, these cells are good news. They show that the immune system is awake and working, usually against a virus. Their presence is a cue for clinicians to ask a simple question: what set this off? That question guides the next tests, such as serology for EBV or CMV.
Older texts use "atypical," "reactive," "variant," and "activated" almost interchangeably. However, modern laboratory standardization guidance recommends phasing out the term "atypical" entirely on official reporting to prevent unnecessary patient anxiety. The strict preference is now "reactive lymphocyte" for cells with a benign, infectious cause, and "abnormal lymphocyte" for cells suspected to be malignant. Keeping that distinction in mind makes the rest of this topic far easier.
Brief Review of Normal Lymphocyte Function and Morphology

Lymphocytes are core players in adaptive immunity, the part of your defense system that targets specific threats. They come in two main families.
B lymphocytes (B cells) handle humoral immunity. When activated, they become plasma cells that pump out antibodies. Those antibodies travel through blood and lymph to tag and neutralize specific invaders.
T lymphocytes (T cells) handle cell-mediated immunity and come in several types. Helper T cells (CD4+) coordinate the response and switch on other immune cells. Cytotoxic T cells (CD8+) kill infected or cancerous cells directly. Regulatory T cells (Tregs) put the brakes on, preventing the immune system from attacking the body itself [2].
Under the microscope, a normal mature lymphocyte is small, roughly 7 to 10 μm, about the size of a red blood cell. It has a round, dark nucleus that fills most of the cell, with only a thin sky-blue rim of cytoplasm around it. The nuclear-to-cytoplasmic (N:C) ratio is high, often 4:1.
What Reactive Lymphocytes Look Like

When a lymphocyte activates, its job changes, and so does its appearance. The shift is dramatic enough that you can often spot it on a smear.
Reactive lymphocytes are bigger, sometimes 10 to 30 μm, and can even dwarf a monocyte. The nucleus loses its tidy round shape and may look oval, kidney-shaped, indented, or lobed, with chromatin that appears finer and nucleoli that may become visible. The cytoplasm grows abundant and turns deep blue, a sign the cell is busy making proteins. A classic clue in glandular fever is a "scalloped" cytoplasm that seems to wrap around or hug nearby red blood cells [9]. The N:C ratio drops compared with resting cells, because there is now much more cytoplasm.
These changes are simply activation made visible. When the immune system meets a pathogen, the right lymphocytes switch on, multiply fast, and ramp up their metabolism. In glandular fever, for example, cytotoxic T cells proliferate to attack virus-infected cells, and that surge of activity is exactly what you see as "atypical" morphology [9].
You may also encounter the term Downey cells, an older morphologic grading (types I–III) for reactive lymphocytes. It is worth recognizing, but bear in mind that subclassifying reactive lymphocytes this way is not routine in modern labs [9].
Table 1: Morphological Differences in Lymphocytes
| Feature | Normal Lymphocyte | Reactive (Benign) Lymphocyte | Abnormal (Malignant/Blast) |
| Size | Small (7 to 10 μm) | Large (10 to 30 μm) | Variable, often large |
| Cytoplasm | Scant, pale blue | Abundant, deep blue, "scalloped" edges | Scant to moderate, lacks scalloping |
| Nucleus | Round, dense chromatin | Irregular, indented, or stretched | Uniformly immature, fine chromatin |
| Nucleoli | Not usually visible | Occasionally visible | Prominent and multiple |
| Clonality | Polyclonal | Polyclonal (mixed B and T cells) | Monoclonal (clonal expansion) |
Common Misconceptions About Atypical Lymphocytes
A few myths cause real confusion, so it is worth clearing them up directly.
"Atypical means cancer." This is the big one. While some malignant cells look atypical, the vast majority of atypical lymphocytes in routine practice are reactive and benign, usually from a virus. They reflect a working immune system, not a disease in themselves.
"It's always glandular fever." EBV is the classic and most common cause of marked atypical lymphocytosis, but it is far from the only one. CMV, HIV, viral hepatitis, certain bacterial and parasitic infections, drug reactions, and some autoimmune conditions all qualify.
"More atypical cells means a sicker patient." Not reliably. A higher percentage may reflect a vigorous immune response, but it does not track neatly with symptom severity or prognosis. A very sick patient may show only modest numbers, and the reverse happens too.
"They point to one specific diagnosis." They do not. Atypical lymphocytes are a nonspecific finding. They flag immune activation, then clinical history, examination, and further tests pin down the cause.
"They mean you need antibiotics." Since most causes are viral, antibiotics usually do nothing and can cause harm, including driving antibiotic resistance.
Causes of Atypical Lymphocytosis
The presence of atypical lymphocytes (reactive lymphocytes) in the peripheral blood is a strong indicator of an active immune response.

Infectious Causes
Infections, especially viral ones, are the leading triggers. The body mounts a robust defense, and the activated cells show up on the smear.
Viral Infections (Most Common)
These are by far the leading cause. The atypical cells are usually activated CD8+ cytotoxic T cells multiplying to clear virus-infected cells.
Epstein-Barr Virus (EBV), the cause of infectious mononucleosis. EBV infects B cells, and the body answers with a strong proliferation of CD8+ T cells that take on reactive morphology. Patients classically show the triad of fever, severe sore throat (often with exudates), and swollen neck lymph nodes. The spleen often enlarges, and fatigue can be deep and long-lasting. On bloodwork, atypical lymphocytes often exceed 10–20% of white cells and can climb much higher.
Cytomegalovirus (CMV). CMV causes a mono-like illness with fever, malaise, swollen glands, and significant atypical lymphocytosis. It usually lacks the severe sore throat of EBV. Diagnosis uses CMV serology (IgM) or PCR for CMV DNA.
HIV (acute seroconversion). Early HIV can produce a mono-like illness with fever, rash, and widespread swollen glands. Atypical lymphocytosis is a common finding as the immune system reacts to the initial viral surge. Testing for HIV matters here, because early diagnosis changes outcomes.
COVID-19 (SARS-CoV-2). COVID-19 commonly produces reactive lymphocytes, and they often look different from the classic forms. Many have a plasmacytoid appearance rather than the typical Downey shapes. In one early case series, reactive lymphocytes with predominantly lymphoplasmacytoid morphology appeared in 72% of patients [7]. Interestingly, their appearance has been linked to a more favorable disease course in hospitalized patients, likely reflecting a strong virus-specific T-cell response [8]. However, with the emergence of new variants, widespread vaccination, and hybrid immunity, profound reactive lymphocytosis is now much less frequently observed in routine outpatient breakthrough cases compared to the primary or severe infections seen during early pandemic waves [12].
Viral hepatitis (A, B, C). Acute hepatitis can trigger reactive atypical lymphocytosis alongside raised liver enzymes.
Other viruses. Adenovirus (often respiratory, with pharyngitis and conjunctivitis), varicella-zoster (chickenpox and shingles), HHV-6 (roseola in young children), and dengue can all produce atypical lymphocytes. Dengue is worth flagging in tropical regions, where its mix of atypical lymphocytosis and low platelets can mimic other febrile illnesses.
Bacterial Infections
Less common than viruses, but some bacteria provoke a reactive lymphocytic response. Mycobacterium tuberculosis, especially in extrapulmonary or disseminated disease, can do so. Bartonella henselae (cat scratch disease) causes regional swollen glands and occasionally reactive cells. Secondary syphilis, with its widespread glands and systemic symptoms, can too. Bordetella pertussis (whooping cough) causes marked lymphocytosis, though usually not predominantly atypical forms [10].
Parasitic Infections
Toxoplasma gondii can closely mimic glandular fever, with fever, non-tender swollen glands, and sometimes an enlarged liver and spleen, confirmed by serology. Acute malaria may show atypical lymphocytes alongside low platelets, again resembling dengue. In endemic areas, examining blood for parasites is essential.
Non-Infectious Causes
Infections dominate, but several other conditions can produce reactive lymphocytes.
Drug Reactions
Some drugs trigger a hypersensitivity reaction that includes immune activation and atypical lymphocytes, usually as part of a wider syndrome.
DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms) is the key example. It is a severe, sometimes life-threatening reaction with fever, widespread rash, swollen glands, eosinophilia, and internal organ involvement. Atypical lymphocytes are a common finding. Frequent culprits include anticonvulsants (phenytoin, carbamazepine, phenobarbital), sulfonamides, dapsone, and allopurinol. The critical step here is recognizing the syndrome and stopping the offending drug.
Autoimmune Diseases
In autoimmune conditions, a reactive lymphocytosis with atypical forms can occasionally appear. Systemic lupus erythematosus more often causes low lymphocytes, but reactive forms can show up during flares or with treatment. Rheumatoid arthritis is a less common association, where chronic inflammation drives reactive changes.
Physiological Stress and Splenectomy
Major physical stress, trauma, or recent surgery can cause a transient, mild reactive lymphocytosis with a few atypical forms. After splenectomy (removal of the spleen), lymphocyte counts often run mildly high, and a small fraction may look atypical, since the spleen's usual filtering role is gone.
Reactive or Malignant? Telling Them Apart
This is the heart of the topic. The conditions below are not causes of reactive atypical lymphocytosis. They matter because their cancerous cells can be mistaken for reactive ones on a smear. Careful evaluation is what keeps these apart.
Acute lymphoblastic leukemia (ALL). Malignant lymphoblasts are immature cells that can resemble highly reactive lymphocytes. The tell is that blasts look uniform and immature, with prominent nucleoli, fine chromatin, and a lack of mature cytoplasmic features. Flow cytometry is essential to confirm.
Chronic lymphocytic leukemia (CLL). Classic CLL cells are small and mature, but a prolymphocytic shift can produce cells with prominent nucleoli and abundant cytoplasm that look atypical. The key is the underlying clonal population.
Lymphoma. Some lymphomas with a leukemic phase, such as Sézary syndrome or mantle cell lymphoma, release malignant cells into the blood that can look transformed or atypical.
Myelodysplastic syndromes (MDS). Mainly a myeloid problem, but some subtypes show reactive lymphocytosis as part of disordered blood cell production.
The single most reliable way to separate reactive from malignant is to look at clonality. Reactive cells are polyclonal, a healthy mix of T and B cells. Malignant cells are monoclonal, all descended from one rogue cell. Flow cytometry is the tool that reveals this. Furthermore, when flow cytometry yields ambiguous results, advanced molecular clonality testing using Next-Generation Sequencing (NGS) for T-cell receptor (TCR) or immunoglobulin heavy chain (IGH) gene rearrangements is now routinely employed to definitively track clonal populations and distinguish them from a polyclonal, reactive background [11].
General Signs and Symptoms

When atypical lymphocytes appear, the patient's symptoms are usually those of the illness that triggered them. Since viral infections are the most common cause, the picture often looks like a bad cold, the flu, or a glandular-fever-like syndrome. The pattern of symptoms, plus context like recent travel or contacts, helps narrow the cause.
Common features include fever, the earliest and most frequent sign; fatigue and malaise, which can be profound and lasting in glandular fever; and sore throat, especially with EBV or adenovirus. Swollen lymph nodes are a classic marker of immune activation. An enlarged spleen is common in EBV and CMV, and it carries a real risk of rupture, particularly with trauma, so it is never ignored.
Rashes can offer clues. A generalized maculopapular rash may appear in acute HIV or drug reactions. Specific rashes point to specific causes, such as roseola in HHV-6 or a petechial rash in severe dengue. One association is worth memorizing: patients with glandular fever who are given amoxicillin or ampicillin often develop a widespread rash, a near-classic clue. Muscle and joint aches round out the systemic picture.
Laboratory Investigations in Atypical Lymphocytosis
Finding atypical lymphocytes on a routine blood count immediately prompts further testing. The goal is to separate benign reactive causes, which are most common, from more serious ones, and to identify the specific trigger. A simple way to picture the workup is a sequence: blood count, then smear, then targeted tests based on suspicion, then flow cytometry if cancer needs ruling out.
Complete Blood Count (CBC) with Differential
This is usually the test that flags the cells. It typically shows a raised total white cell count driven by lymphocytosis. Automated analyzers can flag "atypical" or "variant" lymphocytes, but a human looking down a microscope is still essential for accurate counting and assessment.
As a rule of thumb, atypical lymphocytes above 10% are significant. The likelihood of glandular fever rises sharply with the percentage: above 10% the positive likelihood ratio is about 9, above 20% it is about 28, and above 40% it reaches roughly 50 [3]. Anemia or low platelets can appear in more severe infections and may raise concern for a marrow problem if marked.
Peripheral Blood Smear Review (Crucial Step)
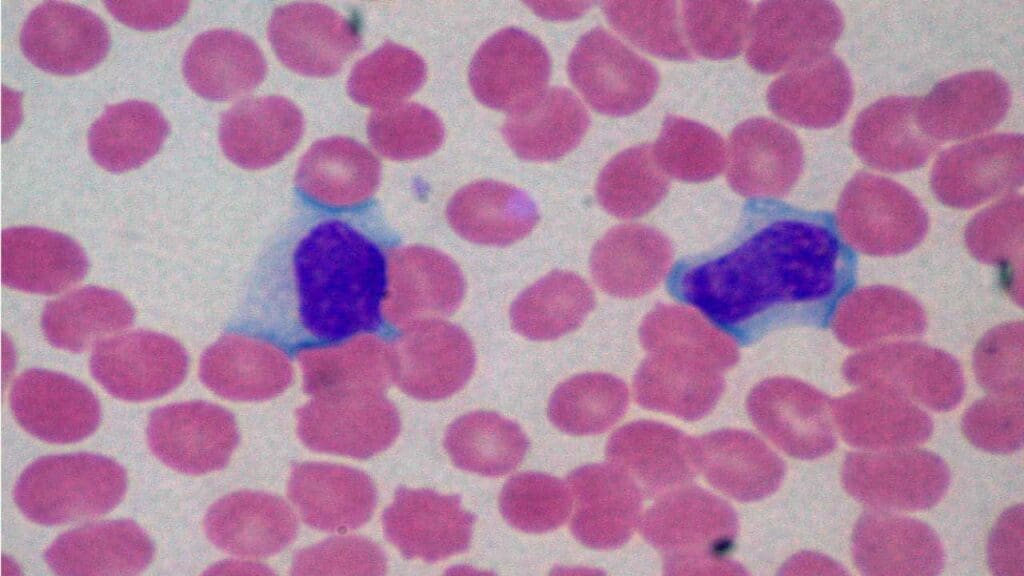
This is the most important test after the CBC, because it lets you see the cells directly. Reactive lymphocytes appear large, with irregular nuclei (kidney-shaped, indented, or lobed), sometimes visible nucleoli, and abundant deep-blue cytoplasm that may be vacuolated. The "scalloped" cytoplasm hugging nearby red cells is highly suggestive of a reactive cause, especially in glandular fever [9].
The smear is also where reactive cells are separated from blasts. Blasts look uniformly immature, with fine chromatin and prominent nucleoli, and they lack the scalloped cytoplasm. Telling these apart takes expertise and often further testing.
Targeted Tests Based on Suspicion
For suspected glandular fever, the heterophile antibody (Monospot) test is a common first step. It is useful but imperfect, with a sensitivity around 87% and specificity around 91%, and it can be falsely negative early in the illness and in young children [3]. Major guidance now cautions against relying on it alone, since it can produce both false positives and false negatives [4]. The practical rule: if the Monospot is negative but glandular fever still fits, move on to EBV-specific serology (VCA IgM and IgG, early antigen, and EBNA) [5]. Up to 10% of genuine cases are heterophile-negative [5].
Other tests follow the clinical clues: CMV serology or PCR, HIV testing, liver function tests (often raised in hepatitis, EBV, and CMV), inflammatory markers like CRP and ESR, autoimmune markers such as ANA if lupus is suspected, and a careful drug history when a reaction is possible.
Flow Cytometry
This specialized test is reserved for when a blood cancer is suspected, or when atypical cells persist, increase, or look ambiguous. It reads the markers on cell surfaces. Reactive cells show a polyclonal pattern with normal markers. Malignant cells show a monoclonal pattern with aberrant markers, which helps diagnose leukemia or lymphoma.
Treatment and Management of Atypical Lymphocytosis
Management depends entirely on the underlying cause, and for the most common triggers it is refreshingly simple. Most viral causes are self-limiting, meaning the body clears them on its own with time. The plan, then, follows a few clear principles.
Treat the cause, support the patient. For common viral infections like EBV and CMV, supportive care is usually all that is needed: rest, fluids, and medicines to bring down fever and ease pain. There is no specific antiviral for routine glandular fever.
Avoid unnecessary antibiotics. Because most causes are viral, antibiotics do not help and can do harm. In glandular fever specifically, amoxicillin and ampicillin commonly trigger a rash and should be avoided unless there is a clear bacterial reason.
Protect the enlarged spleen. When the spleen is enlarged, as it often is in glandular fever, it becomes fragile and can rupture. Patients are typically advised to avoid contact sports and heavy lifting for several weeks until a clinician confirms it is safe. This single piece of advice prevents a rare but dangerous emergency.
Stop the trigger in drug reactions. In DRESS syndrome, the priority is recognizing the reaction and stopping the responsible drug promptly, with specialist care for organ involvement.
Escalate when needed. Persistent, worsening, or ambiguous findings, or features that suggest a blood cancer, warrant referral and further testing such as flow cytometry.
Frequently Asked Questions (FAQs)
What are atypical lymphocytes, in simple terms?
Atypical lymphocytes, also called reactive lymphocytes, are normal immune cells that have grown larger and changed shape because they are actively fighting an infection. They are most often a sign of a viral illness and a healthy immune response, not cancer. They are common in infections like glandular fever (EBV), CMV, and COVID-19.
Do atypical lymphocytes mean I have cancer?
Usually no. The large majority of atypical lymphocytes seen in everyday practice are reactive and harmless, caused by infections. They can occasionally be confused with cancerous cells under the microscope, which is why doctors review a blood smear carefully and, if anything looks unusual or persists, order flow cytometry to be sure.
Does COVID-19 cause atypical lymphocytes?
Yes. COVID-19 commonly produces atypical (reactive) lymphocytes, often with a distinctive plasmacytoid appearance that differs from the classic forms seen in glandular fever. Their presence reflects the body producing virus-specific T cells, and in hospitalized patients it has been linked to a more favorable disease course [8].
How do doctors find the cause of atypical lymphocytes?
The process usually starts with a complete blood count and a blood smear. From there, doctors choose targeted tests based on symptoms: a heterophile (Monospot) test or EBV serology for suspected glandular fever, serology or PCR for CMV, HIV or hepatitis testing where relevant, and flow cytometry if a blood cancer needs ruling out.
Are antibiotics used to treat atypical lymphocytes?
Generally not. Because most cases are caused by viruses, antibiotics do not help and can cause harm, including antibiotic resistance. In glandular fever, the antibiotics amoxicillin and ampicillin often trigger a rash. Treatment usually focuses on rest, fluids, and managing symptoms while the body clears the infection.
Why is an enlarged spleen a concern with glandular fever?
The spleen can swell during infections like EBV mono, and a swollen spleen is more fragile and can rupture, which is a medical emergency. This is why people recovering from glandular fever are usually advised to avoid contact sports and heavy lifting for several weeks until cleared by their clinician.
Glossary of Related Medical Terms
- Atypical lymphocyte (reactive lymphocyte): A normal lymphocyte that has changed size and shape because it has been activated by an immune challenge, usually a virus. "Atypical" means it looks unusual, not that it is cancerous.
- Adaptive immune system: The part of the immune system that learns to recognize specific germs and remembers them for next time.
- B lymphocyte (B cell): A white blood cell that makes antibodies, the proteins that tag and neutralize invaders.
- T lymphocyte (T cell): A white blood cell that directs the immune response or kills infected cells directly.
- CD8+ cytotoxic T cell: A T cell that destroys virus-infected or cancerous cells. These are the cells that usually turn "atypical" in viral infections.
- Polyclonal vs. monoclonal: Polyclonal means many different immune cells responding together (a normal reaction). Monoclonal means one cell type multiplying out of control (a warning sign for cancer).
- Heterophile antibody (Monospot) test: A quick blood test for glandular fever (EBV mono). Useful but imperfect, since it can miss early cases and give false results.
- Flow cytometry: A lab technique that uses lasers to read markers on the surface of cells, helping tell reactive cells from cancerous ones.
- Lymphocytosis: A higher-than-normal number of lymphocytes in the blood.
- Lymphadenopathy: Swollen lymph nodes.
- Splenomegaly: An enlarged spleen.
- DRESS syndrome: Drug Reaction with Eosinophilia and Systemic Symptoms, a serious drug allergy that can include atypical lymphocytes.
- Peripheral blood smear: A drop of blood spread thin on a glass slide and stained so the cells can be examined under a microscope.
- N:C ratio (nuclear-to-cytoplasmic ratio): How much of a cell is taken up by its nucleus versus its surrounding cytoplasm.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Palmer, L., Briggs, C., McFadden, S., Zini, G., Burthem, J., Rozenberg, G., Proytcheva, M., & Machin, S. J. (2015). ICSH recommendations for the standardization of nomenclature and grading of peripheral blood cell morphological features. International journal of laboratory hematology, 37(3), 287–303. https://doi.org/10.1111/ijlh.12327
- Cano RLE, Lopera HDE. Introduction to T and B lymphocytes. In: Anaya JM, Shoenfeld Y, Rojas-Villarraga A, et al., editors. Autoimmunity: From Bench to Bedside [Internet]. Bogota (Colombia): El Rosario University Press; 2013 Jul 18. Chapter 5. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459471/
- Sylvester, J. E., et al. (2023). Infectious mononucleosis: Rapid evidence review. American Family Physician, 107(1), 71–78.
- Centers for Disease Control and Prevention. (2024). Laboratory testing for Epstein-Barr virus (EBV).
- Cunha, B. A., Connolly, J. J., & Irshad, N. (2016). Are atypical lymphocytes present with viral influenza-like illnesses (ILIs) in hospitalized adults?. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology, 35(9), 1399–1401. https://doi.org/10.1007/s10096-016-2675-z
- Weinberg, S. E., Behdad, A., & Ji, P. (2020). Atypical lymphocytes in peripheral blood of patients with COVID-19. British journal of haematology, 190(1), 36–39. https://doi.org/10.1111/bjh.16848
- Pozdnyakova, O., Connell, N. T., Battinelli, E. M., Connors, J. M., Fell, G., & Kim, A. S. (2021). Clinical Significance of CBC and WBC Morphology in the Diagnosis and Clinical Course of COVID-19 Infection. American journal of clinical pathology, 155(3), 364–375. https://doi.org/10.1093/ajcp/aqaa231
- Sugihara, J., Shibata, S., Doi, M., Shimmura, T., Inoue, S., Matsumoto, O., Suzuki, H., Makino, A., & Miyazaki, Y. (2021). Atypical lymphocytes in the peripheral blood of COVID-19 patients: A prognostic factor for the clinical course of COVID-19. PloS one, 16(11), e0259910. https://doi.org/10.1371/journal.pone.0259910
- Sumida, M. P., & Smith, M. A. (2025). A hematopathologist's approach to atypical lymphocytosis. The Hematologist, 22(2). American Society of Hematology. https://doi.org/10.1182/hem.V22.2.2025210
- Hamad H, Mangla A. Lymphocytosis. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549819/
- Donelli, R., Gazzola, A., Mannu, C., Etebari, M., Navari, M., & Piccaluga, P. P. (2024). Conventional PCR-based versus next-generation sequencing-based approach for T-cell receptor γ gene clonality assessment in mature T-cell lymphomas: A phase 3 diagnostic accuracy study. Journal of biological methods, 11(2), e99010013. https://doi.org/10.14440/jbm.2024.0002
- Oliveira, C. B. S., Andrade, J. M. A., & Oliveira, J. I. N. (2022). Are atypical lymphocytes a new predictive factor in the development of COVID-19?. Revista da Sociedade Brasileira de Medicina Tropical, 55, e0154. https://doi.org/10.1590/0037-8682-0154-2022