Key Takeaways
Leukemia is a cancer of the blood and bone marrow caused by genetic changes in blood-forming stem cells, which lead to uncontrolled growth of abnormal cells called blasts [1,2].
- Classifications ▾: The four main types of leukemia are acute lymphoblastic leukemia (ALL), acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), and chronic myeloid leukemia (CML). Acute types progress within weeks. Chronic types develop over months to years.
- Signs and symptoms ▾: Common signs of leukemia include persistent fatigue, easy bruising or bleeding, frequent infections, swollen lymph nodes, bone pain, and unexplained weight loss.
- Diagnosis ▾:Diagnosis rests on a complete blood count, peripheral blood smear, and a bone marrow biopsy, supported by a "diagnostic triad" of flow cytometry, cytogenetics, and molecular testing [1,2,3].
- Treatment and management ▾: Treatment is now highly personalized. Modern care uses targeted drugs such as tyrosine kinase inhibitors, venetoclax-based regimens, and CAR-T cell therapy, alongside traditional chemotherapy [3,4,5].
*Click ▾ for more information
Introduction
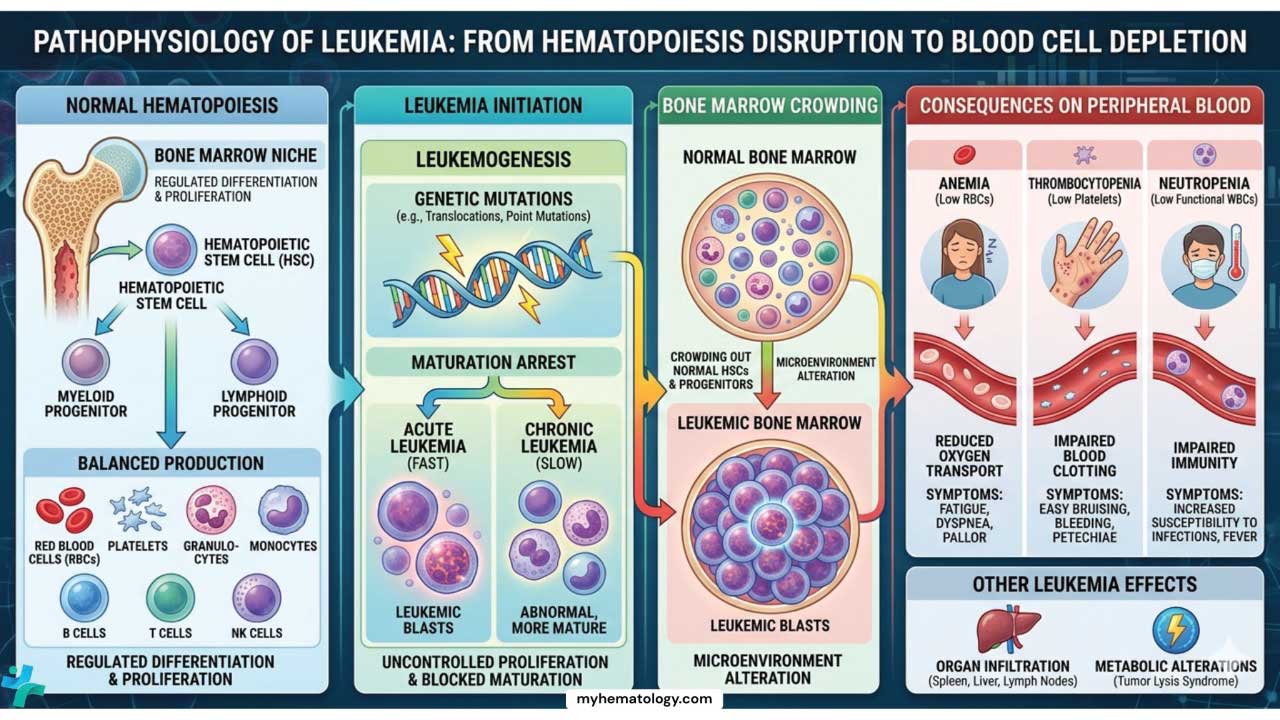
Leukemia is a group of cancers that begin in the blood-forming cells of the bone marrow. In a healthy person, stem cells in the marrow produce a steady supply of red blood cells, white blood cells, and platelets. In leukemia, immature blood cells called blasts multiply out of control. They crowd out healthy cells and spill into the bloodstream.
The result is a triad of problems: anemia from low red cells, recurrent infections from low functional white cells, and bleeding from low platelets. The specific symptoms, speed of onset, and treatment depend on which type of leukemia is involved.
Leukemia was first named in 1845 when the Scottish physician John Hughes Bennett described "leucocythemia." Rudolf Virchow soon distinguished lymphatic from myeloid forms based on the cells involved. The 20th century brought chemotherapy, bone marrow transplantation, and the discovery of recurrent chromosomal abnormalities. The 21st century has shifted the field toward precision medicine, where treatment is tailored to a patient's specific molecular and immunological profile.
perly, leading to various health problems.
Global burden of leukemia
Leukemia is a major global health challenge. In 2020, an estimated 474,519 new cases were diagnosed worldwide, accounting for about 2.5% of all new cancer diagnoses, and 311,594 deaths were attributed to it [1,2]. More than 4 million people are estimated to be living with the disease globally, a figure that is growing as treatments improve and populations age [1].
Patterns vary by region and age. ALL is the most common cancer in young children and remains a leading cause of childhood cancer mortality in countries with limited pediatric oncology services. AML is more common in adults and increases sharply with age. CLL is the most common adult leukemia overall in Western populations [1,2].
Classification of Leukemia
Classification matters because it directly determines treatment. Modern classification uses three lenses at once: the cell of origin, the speed of disease progression, and the specific genetic abnormalities driving the cancer.
By Cell Type
- Lymphoid leukemias arise from abnormal lymphoid progenitor cells, which would normally mature into B-cells or T-cells. They are more common in children and young adults.
- Myeloid leukemias arise from myeloid progenitors, which would normally produce red blood cells, granulocytes, monocytes, and platelets. They are more common in middle-aged and older adults.
By Course
- Acute leukemias progress rapidly. Blasts multiply within weeks, suppressing normal blood cell production.
- Chronic leukemias develop slowly over months or years. Abnormal cells accumulate but often retain some ability to mature.
Subtypes
Acute Lymphoblastic Leukemia (ALL)
ALL is the most common pediatric cancer. It is divided into B-cell and T-cell types based on which lymphocyte lineage is affected. B-cell ALL is the more common form in children. Subtypes include early B-cell, late B-cell, Philadelphia chromosome-positive (Ph+), and Burkitt-type ALL. T-cell ALL is less common and includes early T-cell precursor ALL and cortical T-cell ALL. The diagnosis typically rests on identifying numerous lymphoblasts on a peripheral blood smear.
Acute Myeloid Leukemia (AML)

AML is the more common acute leukemia in adults. The original French-American-British (FAB) system grouped AML into subtypes (M0 through M7) based on cell appearance under the microscope, with acute promyelocytic leukemia (APL, M3) being the best known.
The current WHO 5th edition (2022) and ICC 2022 classifications instead group AML by genetic drivers, which better predict prognosis and guide therapy [1,2].
APL is a hematologic emergency
APL can cause rapid bleeding from disseminated intravascular coagulation. When APL is suspected on the smear or by clinical picture, the standard of care is to start all-trans retinoic acid (ATRA), and arsenic trioxide where available, before genetic confirmation arrives [6].
Pediatric Versus Adult Acute Leukemia at a Glance
| Feature | Pediatric (<18 years) | Adult (>40 years) |
|---|---|---|
| Most common type | ALL (~80% of cases) | AML (rises with age) |
| Origin | Almost always de novo | Often secondary to MDS or prior chemotherapy |
| Common ALL cytogenetics | t(12;21) ETV6-RUNX1, high hyperdiploidy Favorable | t(9;22) BCR::ABL1, hypodiploidy Unfavorable |
| Common AML mutations | KMT2A and NUP98 rearrangements | NPM1, DNMT3A, TET2 (linked to clonal hematopoiesis) |
| Genetic landscape | "Quiet" genome with structural fusions | Higher mutational burden, age-related epigenetic changes |
| Treatment response | Highly chemotherapy-sensitive | More chemo-resistance and toxicity |
| 5-year survival | ~90% ALL ~65–70% AML | ~30–40% ALL ~15–25% AML (varies by age) |
Chronic Lymphocytic Leukemia (CLL)
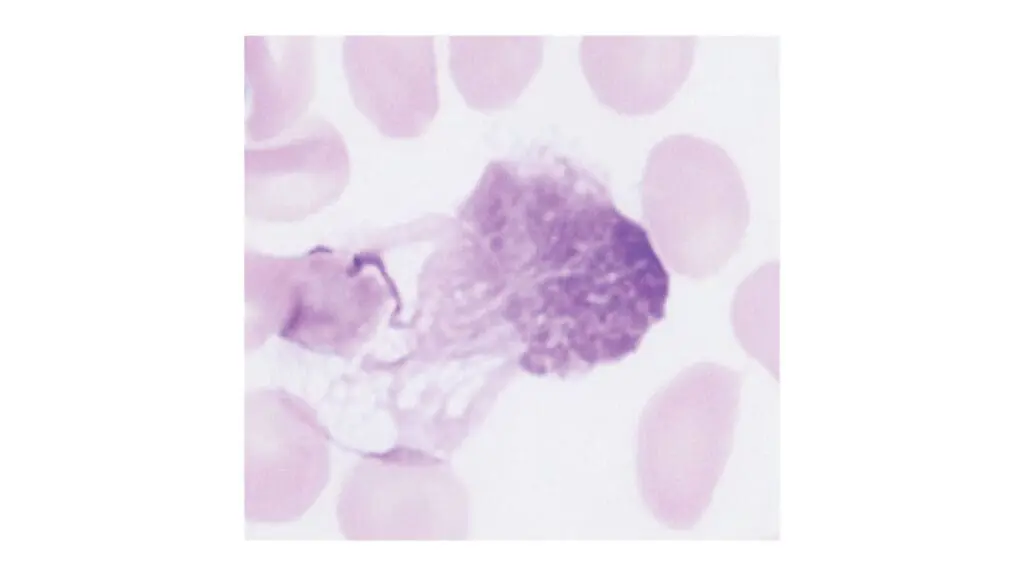
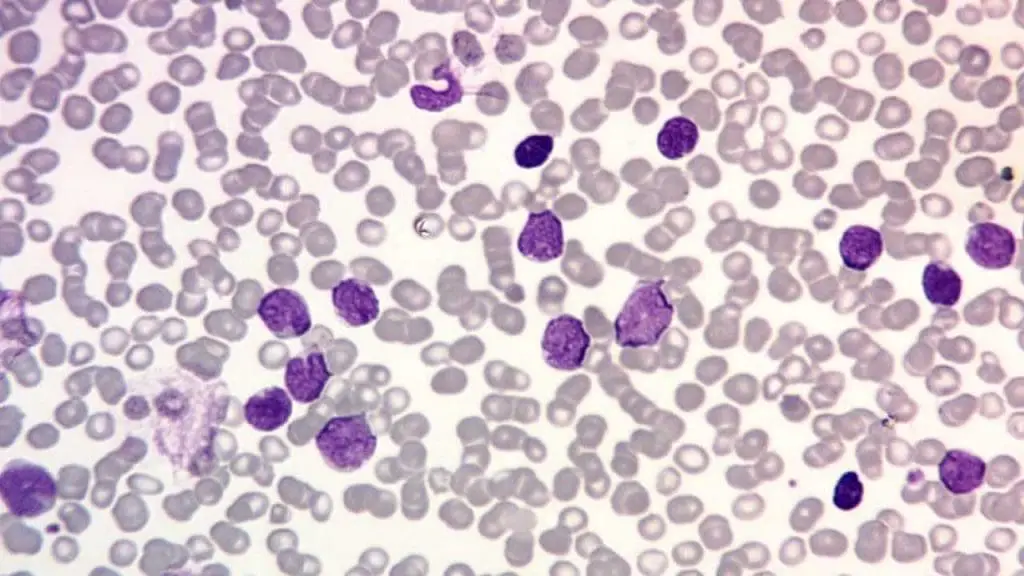
CLL is the most common chronic leukemia in adults. It involves the slow accumulation of mature-appearing B-lymphocytes in the blood, marrow, and lymph nodes. The hallmark finding on a peripheral blood smear is small, mature-looking lymphocytes with clumped "soccer-ball" chromatin, accompanied by smudge cells (Gumprecht shadows), which are fragile lymphocytes that rupture during slide preparation [10].
Chronic Myeloid Leukemia (CML)
CML is defined by the Philadelphia chromosome, the t(9;22) translocation that creates the BCR::ABL1 fusion gene. The fusion produces a constantly active tyrosine kinase that drives uncontrolled growth of myeloid cells. CML usually presents with leukocytosis, basophilia, and a left shift on the blood smear. Untreated, it progresses from a chronic phase to an accelerated phase and finally to blast crisis. Tyrosine kinase inhibitors (TKIs) have transformed it into a manageable chronic disease [11].
Less Common Types
Hairy cell leukemia is a slow-growing B-cell cancer named for the cytoplasmic projections seen on the cells. Adult T-cell leukemia-lymphoma (ATLL) is associated with HTLV-1 infection. Myelodysplastic syndromes (MDS) and myeloproliferative neoplasms (MPN) can sometimes transform into acute leukemia.
Leukemia Pathophysiology
To understand what goes wrong in leukemia, it helps to first picture what goes right.
Normal Hematopoiesis
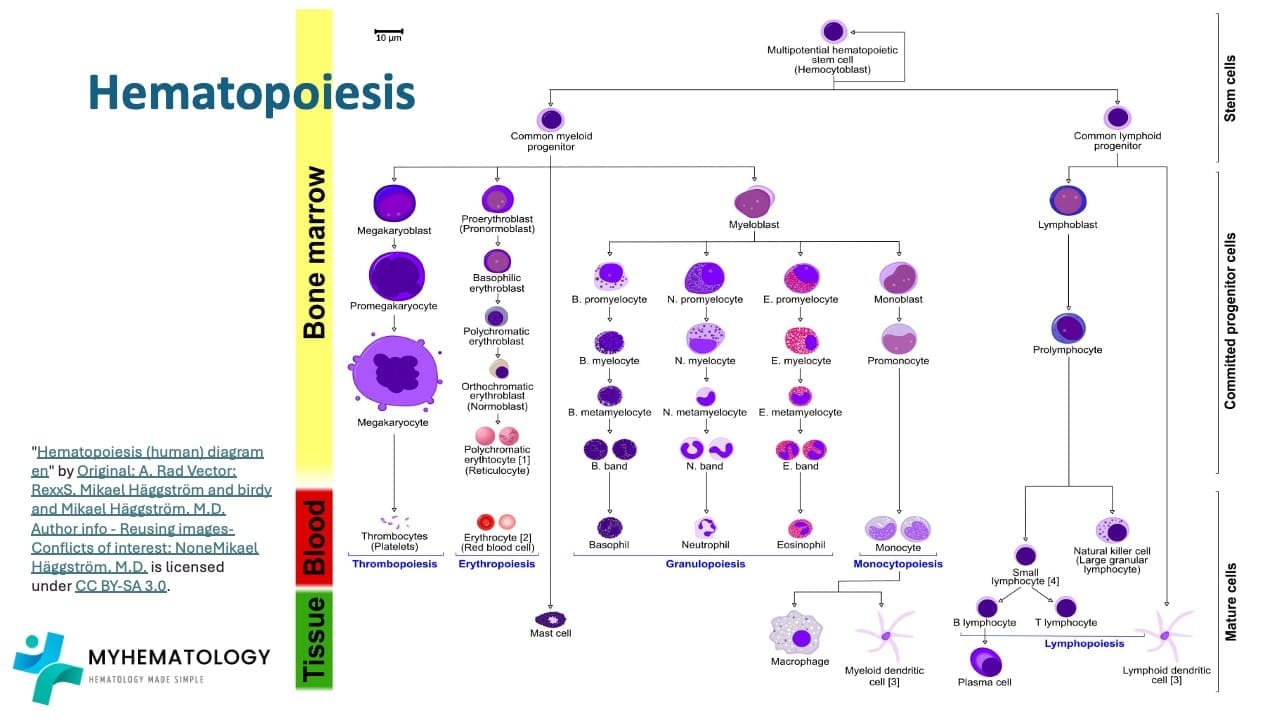
All blood cells originate from a hematopoietic stem cell in the bone marrow. The stem cell can both copy itself and differentiate, meaning mature into specialized cells. It first commits to one of two paths: the lymphoid lineage or the myeloid lineage.
The lymphoid pathway produces B-lymphocytes, T-lymphocytes, and natural killer cells, the immune system's adaptive defenders. The myeloid pathway produces red blood cells (which carry oxygen), platelets (which clot), and granulocytes and monocytes (which fight infection). Each step is tightly regulated by transcription factors and growth signals.
What Goes Wrong in Leukemia
Leukemia begins when a stem or progenitor cell acquires a genetic abnormality that locks it in an immature state and drives it to multiply. Three categories of genetic change contribute:
- Chromosomal abnormalities. Translocations, deletions, and duplications alter gene function. The Philadelphia chromosome in CML is the classic example.
- Point mutations. Single-letter changes in DNA can activate growth-promoting oncogenes or disable tumor suppressor genes. Examples include FLT3 in AML and TP53 in CLL.
- Epigenetic changes. Chemical tags on DNA or histones can switch genes on or off without altering the sequence. DNMT3A and TET2 mutations are common drivers.
A related concept is clonal hematopoiesis of indeterminate potential (CHIP), an age-related state where blood stem cells acquire leukemia-associated mutations but the person has not yet developed cancer. CHIP is now recognized as a precursor risk state for AML and other myeloid cancers [7].
How This Affects the Body
The consequences of these molecular events follow a logical chain. Abnormal cells multiply uncontrollably, crowd out normal stem cells, and disrupt the bone marrow's ability to produce mature cells. The result is the classic clinical triad:
- Anemia (low red blood cells) causes fatigue, pallor, and shortness of breath.
- Neutropenia (low functional white blood cells) leads to recurrent and severe infections.
- Thrombocytopenia (low platelets) causes easy bruising, nosebleeds, and mucosal bleeding.
Leukemic cells can also infiltrate organs, causing an enlarged spleen, liver, or lymph nodes, and in some cases central nervous system disease.
Epidemiology and Risk Factors
Leukemia affects all ages, but its patterns offer clues to its causes.
Age and sex. ALL peaks in early childhood. AML and CLL become more common with age, with the highest rates in people over 65. CML usually appears between 45 and 55. Most leukemia types show a slight male predominance.
Genetic predisposition. Down syndrome substantially increases the risk of childhood ALL. Other inherited conditions, including Li-Fraumeni syndrome and Fanconi anemia, also raise leukemia risk. Having a close relative with leukemia slightly increases personal risk.
Environmental exposures. High-dose ionizing radiation, including prior radiation therapy, is a well-established cause. Chemical exposures matter too, particularly benzene (used in some industrial processes), formaldehyde, ethylene oxide, and certain pesticides. These are recognized in occupational health frameworks.
Lifestyle. Cigarette smoking increases AML risk in proportion to intensity and duration of smoking.
Prior treatment. Some chemotherapy drugs and radiotherapy regimens used for other cancers can cause therapy-related AML or MDS years later.
Clinical Presentation
Leukemia symptoms are often vague at first, which is part of what makes early diagnosis difficult.
General Signs and Symptoms
- Persistent fatigue and weakness (from anemia)
- Recurrent or persistent fever (from neutropenia and infection)
- Easy bruising, nosebleeds, gum bleeding, or petechiae (from thrombocytopenia)
- Swollen, painless lymph nodes in the neck, armpits, or groin
- Unintended weight loss and night sweats
Specific Signs and Symptoms
- Abdominal fullness or discomfort from an enlarged spleen or liver
- Bone or joint pain, especially in long bones, from marrow expansion
- Headaches, vision changes, or seizures if leukemia involves the central nervous system
- Skin changes, such as the violaceous nodules seen in some myeloid leukemias
Acute leukemias typically present with rapidly worsening symptoms and demand urgent care. Chronic leukemias may be detected incidentally on a routine blood test, sometimes years before symptoms appear.
Investigations and Diagnosis
The diagnostic approach to leukemia follows a logical sequence: detect, confirm, then classify.
Phase 1: Initial Screening and Morphology
Most cases begin with a symptomatic patient or an unexpected blood test result.
- Complete blood count (CBC) with differential typically shows abnormal white cell counts, anemia, and thrombocytopenia. A "leukemic hiatus" describes the presence of blasts and mature cells without intermediate stages.
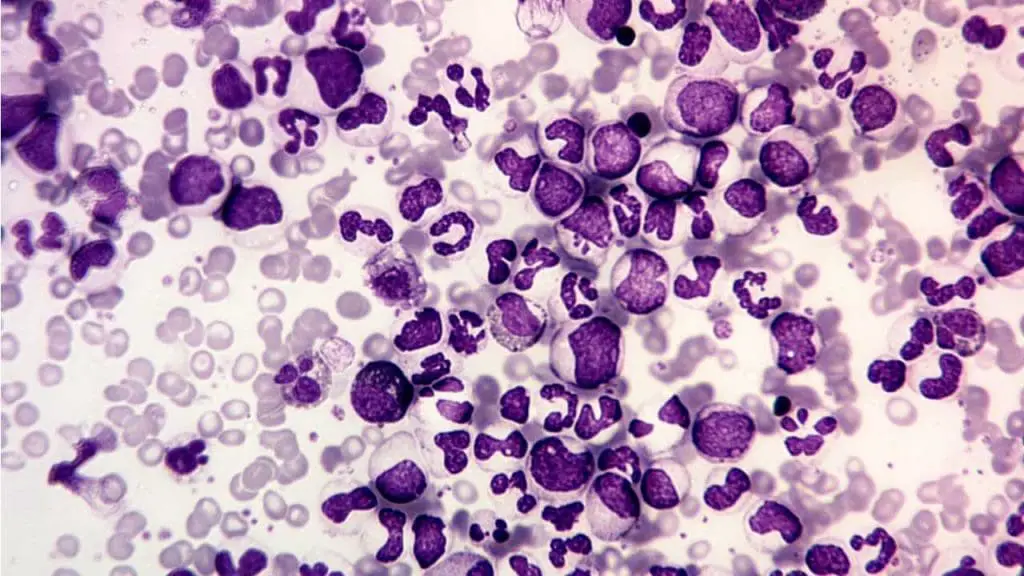
- Peripheral blood smear (PBS) allows direct visualization. Lymphoblasts are smaller with scant cytoplasm and fine chromatin. Myeloblasts are larger with more cytoplasm and prominent nucleoli. Auer rods, needle-shaped pink inclusions inside myeloblasts, confirm AML.
Phase 2: Confirmation by Bone Marrow Biopsy
Bone marrow aspiration and trephine biopsy remain the gold standard. The aspirate is best for counting blasts and assessing morphology. The biopsy shows cellularity and architecture and is essential when the aspirate yields a "dry tap," often seen in hairy cell leukemia or myelofibrosis. Cytochemistry, including myeloperoxidase (MPO) and Sudan Black B staining, is still useful for confirming myeloid lineage in resource-limited settings.
Phase 3: The Diagnostic Triad
Modern leukemia diagnosis is not complete without three parallel investigations on the marrow sample [1,2,3]:
1. Immunophenotyping by flow cytometry. This identifies surface and cytoplasmic CD markers to determine cell lineage.
Flow cytometry reference
| Lineage | Primary markers | Key clinical pointer |
|---|---|---|
| Stem cell / pan-leukemic | CD34HLA-DRTdT | TdT is highly specific for lymphoblasts (ALL) |
| Myeloid (AML) | CD13CD33MPO | MPO is the gold standard for myeloid commitment |
| Monocytic (AML-M4/M5) | CD14CD64 | Distinguishes monocytic from granulocytic AML |
| B-Lymphoid (B-ALL/CLL) | CD19cCD79aCD22 | CD5/CD23 co-expression is hallmark of CLL |
| T-Lymphoid (T-ALL) | cCD3CD7 | Cytoplasmic CD3 is the most lineage-specific T-cell marker |
| Megakaryocytic (AML-M7) | CD41CD61 | Diagnoses rare acute megakaryoblastic leukemia |
| Erythroid (AML-M6) | Glycophorin A | Used when morphology suggests pure erythroid disease |
2. Cytogenetics by karyotyping and FISH. This detects structural chromosomal changes such as t(15;17) in APL, t(8;21) in AML, and t(9;22) in CML and Ph+ ALL [1, 2].
3. Molecular genetics by Next-Generation Sequencing (NGS). In 2026, rapid NGS is no longer optional but it is an emergency requirement. Rapid panels look for specific gene mutations (e.g., NPM1, FLT3, IDH1/2, KMT2A, TP53) that dictate immediate treatment decisions. For example, finding a FLT3 mutation changes the induction drugs given on Day 1, while a TP53 mutation signals that traditional chemotherapy will likely fail and alternative targeted approaches are required [13].
The Blast Threshold Update
A major update from the 2022 WHO and ICC classifications is that the traditional 20% blast threshold for diagnosing AML is no longer absolute. Both classifications now allow AML diagnosis at lower blast counts when defining genetic abnormalities are present, although they differ slightly in how they handle the gray zone between MDS and AML [1,2].
| Feature | WHO 5th ed (2022) | ICC (2022) |
|---|---|---|
| Genetic drivers | Eliminates the 20% blast threshold for most defining mutations, except BCR::ABL1 and CEBPA | Sets a 10% blast threshold for most recurrent genetic abnormalities |
| MDS/AML category | Maintains "MDS with increased blasts" | Introduces a new "MDS/AML" category for 10–19% blasts |
| Secondary AML | Classified as "myeloid neoplasms, secondary" | Uses diagnostic qualifiers for prior MDS or therapy |
Supportive and Staging Investigations
Beyond the marrow, systemic assessment is vital:
- Lumbar puncture is mandatory in ALL to detect or treat central nervous system disease.
- Biochemistry, including LDH, urate, and a coagulation screen (PT, APTT, fibrinogen), helps assess tumor burden and screen for disseminated intravascular coagulation, which is especially common in APL.
- Imaging with chest X-ray or CT can identify mediastinal masses (common in T-ALL) or hepatosplenomegaly. PET-CT is helpful when myeloid sarcoma or extramedullary disease is suspected.
Measurable Residual Disease (MRD)
After chemotherapy, a patient may achieve complete remission (CR) by traditional standards (less than 5% blasts on the marrow). However, very small numbers of leukemia cells often remain. MRD testing finds these cells. It is now considered the single strongest predictor of relapse in both adult and pediatric acute leukemia [8].
| Method | Sensitivity | Targets | Strengths |
|---|---|---|---|
| Flow cytometry (MFC) | 10⁻⁴ to 10⁻⁵ | Leukemia-associated immunophenotypes | Fast, applicable to most patients |
| RT-qPCR | 10⁻⁵ to 10⁻⁶ | Fusion transcripts (e.g., BCR::ABL1, PML::RARA) | Highly standardized for specific translocations |
| Next-generation sequencing | 10⁻⁶ | Ig/TCR rearrangements, gene mutations | Highest sensitivity, detects clonal evolution |
MRD now guides treatment in three concrete ways. In pediatric ALL, MRD at the end of induction (around Day 29) decides whether a child needs intensified chemotherapy or a stem cell transplant [9]. In CML, a rising BCR::ABL1 PCR signal often appears months before clinical relapse, prompting a switch in TKI [11]. In AML, patients who remain MRD-positive in first remission gain the most from allogeneic stem cell transplant [8].
The 2025 ELN-DAVID consensus update tightened the bone marrow MRD threshold for NPM1-mutated AML to 0.1% and introduced a tiered reporting framework: optimal, warning, and high risk of treatment failure [8]. It also emphasizes that "first-pull" marrow aspirates are essential to avoid false negatives from hemodilution.
Prognosis
Outcomes vary widely by leukemia type, age, genetics, and overall health. Childhood ALL now has a 5-year survival rate near 90%. Adult AML survival is lower but rising, currently in the range of 30% across all ages [12]. CLL is generally not cured but is controlled long-term with current targeted drugs. CML, once a fatal disease with a median survival of three to five years, now has 5-year survival around 70% with TKIs [11].
Treatment and Management
The management of leukemia has transitioned from "one-size-fits-all" cytotoxic chemotherapy to a highly personalized, risk-stratified approach. The strategy is defined by the integration of molecular targets, measurable residual disease (MRD) monitoring, and a major shift toward active treatment for older or less-fit patients.
The Three Phases of Acute Leukemia Treatment
| Phase | Goal | Typical Duration | Examples |
|---|---|---|---|
| Induction | Achieve complete remission (blasts <5%, recovered counts) | 4–6 weeks | “7+3” cytarabine and anthracycline for AML, multi-agent chemotherapy for ALL |
| Consolidation | Eliminate residual cells and prevent relapse | 4–8 months | High-dose cytarabine, targeted agents, allogeneic stem cell transplant |
| Maintenance | Prolong remission (used in ALL and APL) | 2–3 years | Low-dose oral methotrexate and 6-mercaptopurine, TKIs in Ph+ ALL |
Lineage-Specific Strategies
Acute Myeloid Leukemia (AML). The 2026 guidelines emphasize that mutational profile and fitness drive treatment intensity. For fit patients, intensive chemotherapy (the "7+3" regimen) remains the backbone, but it is now augmented by targeted drugs based on NGS results. For FLT3-mutated AML, midostaurin or gilteritinib are added. For IDH1 or IDH2 mutations, inhibitors like ivosidenib or enasidenib are deployed [14]. For unfit patients, the combination of venetoclax plus azacitidine remains the global standard. A major recent breakthrough is the introduction of menin inhibitors, such as revumenib, approved for patients with KMT2A translocations or NPM1 mutations, offering a highly effective targeted oral therapy for relapsed disease [15]. Furthermore, oral azacitidine (CC-486) is now frequently used as maintenance therapy for patients in remission who cannot undergo a stem cell transplant [16].
Acute Lymphoblastic Leukemia (ALL). Adolescents and young adults benefit from pediatric-inspired protocols, which use intensive asparaginase-based regimens. However, the biggest shift in adult B-ALL is the movement of immunotherapy into the frontline. Based on the landmark E1910 trial, the bispecific T-cell engager blinatumomab is now standardly incorporated into the initial consolidation phase for Ph-negative B-ALL (regardless of MRD status), drastically improving long-term survival while reducing chemotherapy reliance [17]. In Ph-positive ALL, highly potent TKIs like ponatinib are now frequently combined with blinatumomab in entirely "chemo-free" induction regimens [18].
Chronic Myeloid Leukemia (CML). Standard TKIs such as imatinib, dasatinib, nilotinib, and bosutinib remain foundational. However, asciminib, a first-in-class STAMP inhibitor that binds to the ABL myristoyl pocket rather than the ATP-binding site, has demonstrated superior efficacy and a favorable safety profile compared to older TKIs in the frontline setting (ASC4FIRST trial), positioning it as a preferred first-line option for many newly diagnosed patients [19]. The ultimate goal remains achieving a deep molecular response to allow for treatment-free remission (TFR) in carefully selected patients.
Chronic Lymphocytic Leukemia (CLL). Chemoimmunotherapy regimens such as FCR and BR are largely obsolete in the frontline. Modern care centers on continuous therapy with covalent BTK inhibitors (acalabrutinib, zanubrutinib) or fixed-duration regimens using the BCL-2 inhibitor venetoclax combined with an anti-CD20 antibody (obinutuzumab). For patients who progress on covalent BTK inhibitors, the FDA-approved non-covalent BTK inhibitor pirtobrutinib provides a vital lifeline, capable of re-establishing disease control even after the cancer mutates to resist earlier therapies [20].
Targeted and Cellular Therapies
CAR-T cell therapy. A patient's own T-cells are collected, genetically engineered to recognize CD19 (or sometimes CD22) on B-cells, expanded in the lab, and infused back. Tisagenlecleucel is approved for relapsed or refractory pediatric and young-adult B-ALL. Brexucabtagene autoleucel is approved for adult B-ALL [5]. The most important toxicities are cytokine release syndrome (CRS), a systemic inflammatory response treated with the IL-6 blocker tocilizumab, and immune effector cell-associated neurotoxicity syndrome (ICANS), which can cause confusion and seizures.
Bispecific T-cell engagers (BiTEs). These antibodies physically link the patient's T-cells to leukemic blasts, triggering immune killing. Blinatumomab is the leading example.
Supportive Care and Oncologic Emergencies
Managing leukemia is as much about complications as cancer killing.
Tumor lysis syndrome (TLS). When large numbers of leukemia cells die rapidly, they release potassium, phosphate, and uric acid into the blood. This can cause kidney failure and life-threatening arrhythmias. Prevention uses aggressive intravenous hydration and allopurinol. Rasburicase, which breaks down existing uric acid, is used in high-risk patients.
Febrile neutropenia. A patient with a low neutrophil count cannot mount a normal inflammatory response, so a fever may be the only sign of severe infection. Any temperature above 38.0 °C (100.4 °F) in a neutropenic patient is a medical emergency. Broad-spectrum intravenous antibiotics, such as piperacillin-tazobactam, must be given within one hour.
Late Effects and Survivorship
For the growing population of leukemia survivors, especially children with ALL, late effects matter. Anthracycline chemotherapy carries a long-term risk of cardiotoxicity. Cranial radiotherapy and intrathecal methotrexate can cause neurocognitive effects. Both chemotherapy and radiotherapy can affect fertility, which is why sperm banking, oocyte retrieval, or ovarian tissue cryopreservation should be discussed before treatment when possible. There is also a small but real risk of secondary malignancies decades after cure. Long-term survivorship clinics are now standard practice in major centers.
Frequently Asked Questions (FAQs)
What is leukemia caused by?
In most cases the exact cause is unknown. What we do know is that leukemia begins when blood-forming cells acquire genetic changes that disrupt normal development. Some changes are inherited, but most are acquired during life. Established contributors include high-dose radiation, exposure to chemicals such as benzene and formaldehyde, prior chemotherapy, certain viral infections (HTLV-1 in adult T-cell leukemia), and genetic conditions such as Down syndrome. Smoking is a recognized risk factor for AML.
Who is most at risk for leukemia?
Risk varies by type. Children under 5 are most susceptible to ALL. Adults over 65 are most susceptible to CLL and AML. Men have a slightly higher overall risk. Family history slightly increases risk, suggesting a genetic component. Specific risk factors include Down syndrome (raises ALL risk), occupational benzene exposure (raises AML risk), prior cancer treatment (raises therapy-related AML risk), and smoking (raises AML risk).
Is leukemia curable if caught early?
It depends on the type. Childhood ALL has cure rates near 90% with modern treatment. Adult AML has improving outcomes, especially with targeted therapy, though cure rates remain lower than in children. CML is not technically cured, but TKIs allow most patients to live a near-normal lifespan, and a select group can achieve treatment-free remission. CLL is generally considered incurable but is controlled long-term, with many patients living for decades.
What does measurable residual disease (MRD) mean?
MRD, sometimes called minimal residual disease, refers to the small number of leukemia cells that remain after treatment but are too few to see by traditional microscopy. Modern tests can find one leukemia cell among 100,000 to 1,000,000 normal cells. MRD status is the strongest predictor of relapse and now guides decisions about further chemotherapy, targeted drugs, or stem cell transplant [8].
How is flow cytometry used in the diagnosis of leukemia?
Flow cytometry analyzes the unique cluster of differentiation (CD) markers on a cell's surface and inside the cell. By running a marrow or blood sample through the flow cytometer, the lab determines the lineage of the leukemic cells (myeloid versus lymphoid) and their stage of maturation. This precise immunophenotyping is essential for assigning the correct WHO or ICC subtype and for choosing targeted therapy [1,2].
What is the difference between leukemia and lymphoma?
Both are blood cancers, but they differ in location and presentation. Leukemia primarily affects the bone marrow and bloodstream, with abnormal cells circulating freely. Lymphoma primarily affects the lymphatic system, including lymph nodes, spleen, and thymus, and typically forms solid tumors in those tissues. The same lymphocyte type can give rise to either disease, which is why the distinction sometimes blurs in advanced cases.
How long can a person live with leukemia?
Survival varies widely by type, age, genetics, and access to care. Childhood ALL now has a 5-year survival rate close to 90%. Adult AML 5-year survival sits around 30% and is improving with targeted therapy [12]. CLL has 5-year survival above 85%. CML 5-year survival has reached approximately 70% in the era of TKIs [11]. These figures are population averages; individual outcomes depend strongly on disease subtype and treatment response.
What can caregivers do to support someone with leukemia?
The most useful caregiver actions are practical. Track appointments, medications, and side effects. Watch for fever above 38.0 °C in a patient on chemotherapy, since this is a medical emergency requiring same-hour antibiotics. Reduce infection risk at home through hand hygiene and food safety. Recognize that fatigue, mood changes, and "chemo brain" are common during and after treatment. Connect early with a hematology social worker, who can help with financial, fertility, and long-term survivorship support.
Glossary of Related Medical Terms
- Acute leukemia: Fast-growing blood cancer where immature blasts dominate the marrow within weeks.
- Allogeneic stem cell transplant: Replacement of diseased marrow with stem cells from a matched donor.
- Auer rods: Pink, needle-shaped inclusions in leukemic cells that confirm AML.
- Blast: An immature blood cell. Excess blasts in blood or marrow signal acute leukemia.
- BCR::ABL1: Fusion gene from the Philadelphia chromosome translocation, driving CML and Ph+ ALL.
- CAR-T cell therapy: Treatment that re-engineers a patient's T-cells to attack leukemia.
- Chronic leukemia: Slow-growing blood cancer where abnormal cells accumulate over months to years.
- Clonal hematopoiesis of indeterminate potential (CHIP): Age-related state where blood stem cells carry leukemia-linked mutations without overt disease.
- Cytogenetics: Study of chromosome structure, used to identify abnormalities in leukemia.
- Cytopenia: Reduced count of one or more blood cell types.
- Differentiation: The maturation of a stem cell into a specialized cell type.
- Flow cytometry: Lab method using lasers to identify cell-surface markers, central to leukemia subtyping.
- Hematopoiesis: Normal process of blood cell formation in the bone marrow.
- Immunophenotyping: Using CD markers to determine lineage and maturity of leukemia cells.
- Induction chemotherapy: First, intensive treatment phase aimed at complete remission.
- Measurable residual disease (MRD): Small numbers of remaining leukemia cells detected by sensitive testing.
- Neutropenia: Low neutrophil count, increasing risk of severe infection.
- Philadelphia chromosome: Shortened chromosome 22 from the t(9;22) translocation, hallmark of CML.
- Remission: State where signs of leukemia have disappeared. Complete remission requires <5% marrow blasts and recovered counts.
- Smudge cells (Gumprecht shadows): Fragile, ruptured lymphocytes seen on the smear in CLL.
- Thrombocytopenia: Low platelet count, leading to bruising and bleeding.
- Tumor lysis syndrome (TLS): Metabolic emergency from rapid leukemia cell breakdown during treatment.
- Tyrosine kinase inhibitor (TKI): Targeted drug that blocks BCR::ABL1; transformed CML treatment.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Döhner, H., Wei, A. H., Appelbaum, F. R., Craddock, C., DiNardo, C. D., Dombret, H., Ebert, B. L., Fenaux, P., Godley, L. A., Hasserjian, R. P., Larson, R. A., Levine, R. L., Miyazaki, Y., Niederwieser, D., Ossenkoppele, G., Röllig, C., Sierra, J., Stein, E. M., Tallman, M. S., Tien, H. F., … Löwenberg, B. (2022). Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood, 140(12), 1345–1377. https://doi.org/10.1182/blood.2022016867
- DiNardo, C. D., Jonas, B. A., Pullarkat, V., Thirman, M. J., Garcia, J. S., Wei, A. H., Konopleva, M., Döhner, H., Letai, A., Fenaux, P., Koller, E., Havelange, V., Leber, B., Esteve, J., Wang, J., Pejsa, V., Hájek, R., Porkka, K., Illés, Á., Lavie, D., … Pratz, K. W. (2020). Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. The New England journal of medicine, 383(7), 617–629. https://doi.org/10.1056/NEJMoa2012971
- Maude, S. L., Laetsch, T. W., Buechner, J., Rives, S., Boyer, M., Bittencourt, H., Bader, P., Verneris, M. R., Stefanski, H. E., Myers, G. D., Qayed, M., De Moerloose, B., Hiramatsu, H., Schlis, K., Davis, K. L., Martin, P. L., Nemecek, E. R., Yanik, G. A., Peters, C., Baruchel, A., … Grupp, S. A. (2018). Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. The New England journal of medicine, 378(5), 439–448. https://doi.org/10.1056/NEJMoa1709866
- Lo-Coco, F., Avvisati, G., Vignetti, M., Thiede, C., Orlando, S. M., Iacobelli, S., Ferrara, F., Fazi, P., Cicconi, L., Di Bona, E., Specchia, G., Sica, S., Divona, M., Levis, A., Fiedler, W., Cerqui, E., Breccia, M., Fioritoni, G., Salih, H. R., Cazzola, M., … Study Alliance Leukemia (2013). Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. The New England journal of medicine, 369(2), 111–121. https://doi.org/10.1056/NEJMoa1300874
- Jaiswal, S., Fontanillas, P., Flannick, J., Manning, A., Grauman, P. V., Mar, B. G., Lindsley, R. C., Mermel, C. H., Burtt, N., Chavez, A., Higgins, J. M., Moltchanov, V., Kuo, F. C., Kluk, M. J., Henderson, B., Kinnunen, L., Koistinen, H. A., Ladenvall, C., Getz, G., Correa, A., … Ebert, B. L. (2014). Age-related clonal hematopoiesis associated with adverse outcomes. The New England journal of medicine, 371(26), 2488–2498. https://doi.org/10.1056/NEJMoa1408617
- Cloos, J., Valk, P. J. M., Thiede, C., Döhner, K., Roboz, G. J., Wood, B. L., Walter, R. B., Wang, S., Wierzbowska, A., Wei, A. H., Wu, D., Vergez, F., Venditti, A., van der Reijden, B. A., van de Loosdrecht, A. A., Tiong, I. S., Thol, F. R., Subklewe, M., Roumier, C., Reuvekamp, T., … Heuser, M. (2026). 2025 update on MRD in acute myeloid leukemia: a consensus document from the ELN-DAVID MRD Working Party. Blood, 147(11), 1147–1167. https://doi.org/10.1182/blood.2025031480
- Sekeres, M. A., Mattison, R., Artz, A., Baer, M. R., Chua, C. C., Demichelis-Gómez, R., Egan, P. C., Fletcher, L., Foucar, C., Garcia, J. S., Gilberto, L., Gómez de León, A., Lancet, J., Loh, K. P., Malcovati, L., Marini, B., Platzbecker, U., Sorror, M. L., Tinsley-Vance, S., Treitz, J., … Brignardello-Petersen, R. (2026). American Society of Hematology 2025 guidelines for treating newly diagnosed acute myeloid leukemia in older adults. Blood advances, 10(6), 1897–1928. https://doi.org/10.1182/bloodadvances.2025017934
- Hallek, M., Cheson, B. D., Catovsky, D., Caligaris-Cappio, F., Dighiero, G., Döhner, H., Hillmen, P., Keating, M., Montserrat, E., Chiorazzi, N., Stilgenbauer, S., Rai, K. R., Byrd, J. C., Eichhorst, B., O'Brien, S., Robak, T., Seymour, J. F., & Kipps, T. J. (2018). iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood, 131(25), 2745–2760. https://doi.org/10.1182/blood-2017-09-806398
- Hochhaus, A., Baccarani, M., Silver, R. T., Schiffer, C., Apperley, J. F., Cervantes, F., Clark, R. E., Cortes, J. E., Deininger, M. W., Guilhot, F., Hjorth-Hansen, H., Hughes, T. P., Janssen, J. J. W. M., Kantarjian, H. M., Kim, D. W., Larson, R. A., Lipton, J. H., Mahon, F. X., Mayer, J., Nicolini, F., … Hehlmann, R. (2020). European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia, 34(4), 966–984. https://doi.org/10.1038/s41375-020-0776-2
- https://seer.cancer.gov/statfacts/html/leuks.html
- National Comprehensive Cancer Network. (2024). NCCN Clinical Practice Guidelines in Oncology: Acute Myeloid Leukemia.
- Montesinos, P., Recher, C., Vives, S., Zarzycka, E., Wang, J., Bertani, G., Heuser, M., Calado, R. T., Schuh, A. C., Yeh, S. P., Daigle, S. R., Hui, J., Pandya, S. S., Gianolio, D. A., de Botton, S., & Döhner, H. (2022). Ivosidenib and Azacitidine in IDH1-Mutated Acute Myeloid Leukemia. The New England journal of medicine, 386(16), 1519–1531. https://doi.org/10.1056/NEJMoa2117344
- Issa, G. C., Aldoss, I., DiPersio, J., Cuglievan, B., Stone, R., Arellano, M., Thirman, M. J., Patel, M. R., Dickens, D. S., Shenoy, S., Shukla, N., Kantarjian, H., Armstrong, S. A., Perner, F., Perry, J. A., Rosen, G., Bagley, R. G., Meyers, M. L., Ordentlich, P., Gu, Y., … Stein, E. M. (2023). The menin inhibitor revumenib in KMT2A-rearranged or NPM1-mutant leukaemia. Nature, 615(7954), 920–924. https://doi.org/10.1038/s41586-023-05812-3
- Wei, A. H., Döhner, H., Pocock, C., Montesinos, P., Afanasyev, B., Dombret, H., Ravandi, F., Sayar, H., Jang, J. H., Porkka, K., Selleslag, D., Sandhu, I., Turgut, M., Giai, V., Ofran, Y., Kizil Çakar, M., Botelho de Sousa, A., Rybka, J., Frairia, C., Borin, L., … QUAZAR AML-001 Trial Investigators (2020). Oral Azacitidine Maintenance Therapy for Acute Myeloid Leukemia in First Remission. The New England journal of medicine, 383(26), 2526–2537. https://doi.org/10.1056/NEJMoa2004444
- Litzow, M. R., Sun, Z., Mattison, R. J., Paietta, E. M., Roberts, K. G., Zhang, Y., Racevskis, J., Lazarus, H. M., Rowe, J. M., Arber, D. A., Wieduwilt, M. J., Liedtke, M., Bergeron, J., Wood, B. L., Zhao, Y., Wu, G., Chang, T. C., Zhang, W., Pratz, K. W., Dinner, S. N., … Tallman, M. S. (2024). Blinatumomab for MRD-Negative Acute Lymphoblastic Leukemia in Adults. The New England journal of medicine, 391(4), 320–333. https://doi.org/10.1056/NEJMoa2312948
- Jabbour, E., Short, N. J., Jain, N., Huang, X., Montalban-Bravo, G., Banerjee, P., Rezvani, K., Jiang, X., Kim, K. H., Kanagal-Shamanna, R., Khoury, J. D., Patel, K., Kadia, T. M., Daver, N., Chien, K., Alvarado, Y., Garcia-Manero, G., Issa, G. C., Haddad, F. G., Kwari, M., … Kantarjian, H. (2023). Ponatinib and blinatumomab for Philadelphia chromosome-positive acute lymphoblastic leukaemia: a US, single-centre, single-arm, phase 2 trial. The Lancet. Haematology, 10(1), e24–e34. https://doi.org/10.1016/S2352-3026(22)00319-2
- Hochhaus, A., Wang, J., Kim, D. W., Kim, D. D. H., Mayer, J., Goh, Y. T., le Coutre, P., Takahashi, N., Kim, I., Etienne, G., Andorsky, D., Issa, G. C., Larson, R. A., Bombaci, F., Kapoor, S., McCulloch, T., Malek, K., Yau, L., Ifrah, S., Hoch, M., … ASC4FIRST Investigators (2024). Asciminib in Newly Diagnosed Chronic Myeloid Leukemia. The New England journal of medicine, 391(10), 885–898. https://doi.org/10.1056/NEJMoa2400858
- Mato, A. R., Woyach, J. A., Brown, J. R., Ghia, P., Patel, K., Eyre, T. A., Munir, T., Lech-Maranda, E., Lamanna, N., Tam, C. S., Shah, N. N., Coombs, C. C., Ujjani, C. S., Fakhri, B., Cheah, C. Y., Patel, M. R., Alencar, A. J., Cohen, J. B., Gerson, J. N., Flinn, I. W., … Jurczak, W. (2023). Pirtobrutinib after a Covalent BTK Inhibitor in Chronic Lymphocytic Leukemia. The New England journal of medicine, 389(1), 33–44. https://doi.org/10.1056/NEJMoa2300696


