Key Takeaways
Dendritic cells are the immune system's most powerful antigen-presenting cells. They capture material from pathogens, damaged cells, or tumors and show it to T cells, which then launch a targeted adaptive immune response.
- Classification ▾: Classic subsets are cDC1, cDC2, and pDC. Current single-cell studies add DC3, monocyte-derived DCs, and a transitional AXL⁺SIGLEC6⁺ population to the family [4,5].
- Functions of Dendritic Cells ▾: They control both immunity and tolerance. The same cells that activate T cells against pathogens also teach the immune system not to attack the body's own tissues.
- Dendritic cells are a real therapeutic target ▾. Sipuleucel-T is the first FDA-approved dendritic cell-based therapy for prostate cancer [7], and newer personalized neoantigen vaccines combined with checkpoint inhibitors are in active clinical trials [6,8].
*Click ▾ for more information
Introduction
If T cells are the immune system's snipers, dendritic cells are the spotters. They sit quietly in tissues that meet the outside world like the skin, the gut lining, the airways and sampling whatever comes in. When something looks dangerous, they grab it, change their behavior dramatically, and carry the information to a lymph node, where the adaptive immune response begins.
This single ability makes them one of the most important cells in immunology. They influence vaccine responses, antiviral defense, transplant outcomes, autoimmune disease, and most modern cancer immunotherapies. If you understand dendritic cells, much of the rest of immunology falls into place.
Overview of the immune system
The immune system is usually split into two arms that work together.
The innate immune system is the fast, generic response: physical barriers like skin, phagocytes such as neutrophils and macrophages, natural killer cells, and inflammation. It buys time.
The adaptive immune system is slower but specific and long-lasting. It relies on lymphocytes like B cells, which make antibodies, and T cells, which kill infected cells or coordinate other immune cells. Adaptive immunity is also responsible for immunological memory, which is why vaccines work.
Dendritic cells are the bridge. They are innate sensors that physically deliver information to the adaptive system.
Dendritic Cell Classification
Dendritic cells are not one thing. They are a family, and that family has grown.
Their job description which includes capture, process, present, is shared, but each subset is tuned for a different kind of threat. The classical view, which is still useful, splits them into conventional dendritic cells (cDCs) and plasmacytoid dendritic cells (pDCs). Single-cell RNA sequencing in the past decade has added several more populations [4,5].
| Feature | Dendritic Cells | Neutrophils | Macrophages | Lymphocytes (B & T) |
|---|---|---|---|---|
| Main job | Antigen presentation, starting adaptive immunity | Phagocytosis of bacteria, inflammation | Phagocytosis, antigen presentation, tissue repair | Antibodies (B), cell-mediated immunity (T) |
| Antigen presentation | Most powerful; uniquely activate naive T cells | Limited | Yes, mainly in established infection | Not in the same way |
| Shape | Long branching projections | Lobed nucleus, granular | Large and variable | Small, round, large nucleus |
| Origin | Mostly myeloid; some lymphoid | Myeloid | Myeloid (from monocytes) | Lymphoid |
| Where | Tissues, then lymph nodes | Blood, then sites of infection | Tissues | Lymphoid organs, blood, lymph |
| Lifespan | Weeks to months | Days | Months to years | Variable |
| Key markers | CD11c, MHC II, CD80/86 | CD15, CD16 | CD14, CD68 | CD19/CD20 (B); CD3/CD4/CD8 (T) |
Conventional dendritic cells (cDCs)
Conventional dendritic cells are the workhorse antigen presenters. They arise from myeloid progenitors in the bone marrow and split into two main types [2,3].
cDC1s specialize in cross-presentation which means taking antigens picked up from outside the cell and displaying them on MHC class I. This is how they alert CD8⁺ killer T cells to viruses and tumor cells. They carry markers like CD141 (BDCA-3) in humans, plus XCR1, and are central to anti-tumor immunity [8].
cDC2s are more versatile. They present mainly on MHC class II to CD4⁺ helper T cells and shape Th1, Th2, and Th17 responses, depending on the signals they receive. They carry CD1c (BDCA-1) in humans.
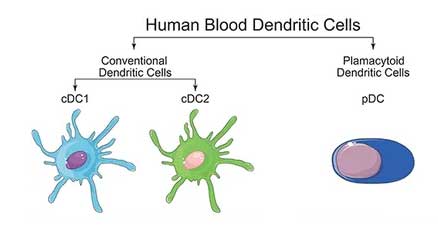
Plasmacytoid dendritic cells (pDCs)
Plasmacytoid dendritic cells look more like plasma cells than classical dendritic cells, which is where the name comes from. Their standout role is pouring out type I interferons (IFN-α/β) when they sense viral nucleic acids through TLR7 and TLR9 [2]. Type I interferons put neighboring cells into an antiviral state and recruit other immune cells. They are weaker antigen presenters than cDCs but help bridge innate and adaptive immunity. Markers include CD123 and BDCA-2 (CD303).
DC3, mo-DCs, and AXL⁺SIGLEC6⁺ dendritic cells
Recent single-cell transcriptomic work has reshaped this map [4,5]:
- DC3 is now recognized as a distinct, bona fide lineage that develops independently of cDC2s and monocytes, heavily reliant on the cytokine GM-CSF. Rather than just a "mixed" signature, DC3s are specialized pro-inflammatory cells increasingly implicated in driving systemic inflammation (particularly in autoimmune conditions) and play a critical role in shaping the tumor microenvironment [10].
- Monocyte-derived dendritic cells (mo-DCs) form in inflamed tissues when monocytes are pushed toward a dendritic-cell-like state. They matter both biologically and practically as most clinical DC vaccines are mo-DCs grown from a patient's blood.
- AXL⁺SIGLEC6⁺ dendritic cells (also called AS-DCs, DC5, or transitional DCs) share features of pDCs and cDCs and can prime T cells potently. Whether they are a true subset or a transitional state is still debated.
Tissue-resident dendritic cells
Some dendritic cells live in specific tissues and have specialized roles. Langerhans cells sit in the epidermis and contribute to skin immunity and tolerance. While they look and function similarly to classical dendritic cells, Langerhans cells are actually derived from embryonic macrophages rather than bone marrow dendritic cell progenitors [11]. Follicular dendritic cells in lymphoid follicles trap antigen–antibody complexes for B cells to inspect. Despite the shared name, they are not derived from the dendritic cell lineage discussed above.
Morphology of Dendritic Cells
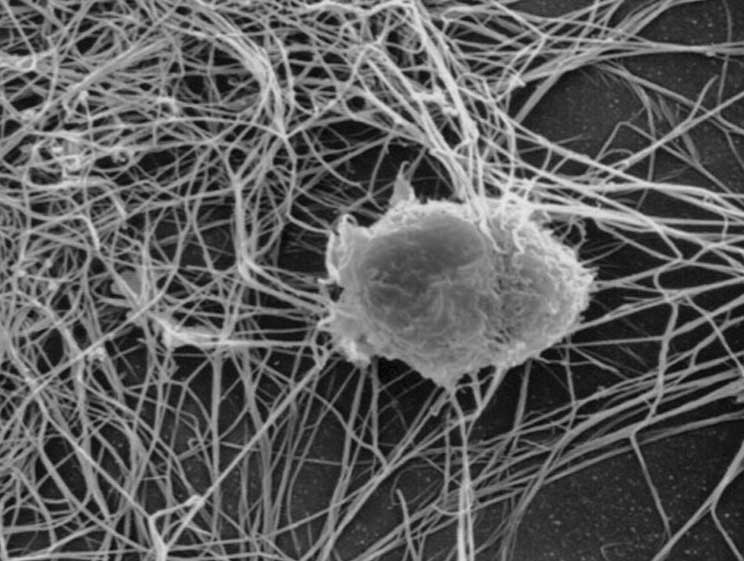
Dendritic cells are named for their dendrites — long, branching cytoplasmic projections that look like tree branches under a microscope.
Under light microscopy, an immature dendritic cell looks fairly unremarkable: rounded and irregular. Once it matures, it sprouts numerous branched projections that give it a star-like appearance. Electron microscopy shows that these projections are filled with mitochondria, ribosomes, and endosomes, and that the surface is heavily folded. All of that surface area helps them sample as much of their environment as possible.
The dendrites support three modes of antigen uptake:
Receptor-mediated endocytosis — pulling in specific antigens caught by surface receptors.
Phagocytosis — swallowing whole particles such as bacteria or cell debris.
Macropinocytosis — drinking surrounding fluid in big gulps to sample dissolved antigens.
| Feature | Immature cDC | Mature cDC | cDC1 | cDC2 | pDC |
|---|---|---|---|---|---|
| Shape | Rounded | Highly irregular | Slender dendrites | Broader, leaf-like | Rounded, plasmacytoid |
| Dendrites | Few, short | Many, long, branched | Elongated | Broader | Few, short |
| Uptake activity | High | Reduced | – | – | – |
| T-cell activation | Low | High | High (CD8⁺ via cross-presentation) | High (CD4⁺) | Lower than cDCs |
| Key markers | MHC II, CD11c | MHC II high, CD11c, CD80/86 high | CD141, XCR1 | CD1c (BDCA-1) | CD123, BDCA-2, TLR7, TLR9 |
Development and Maturation
Where they come from
Dendritic cells originate from hematopoietic stem cells in the bone marrow. Transcription factors including PU.1, IRF8, and BATF3 (for cDC1s) and E2-2 (for pDCs) guide their lineage commitment, while cytokines such as FLT3L and GM-CSF support their differentiation and survival [3].
Once made, immature dendritic cells leave the bone marrow, circulate briefly, and settle in peripheral tissues especially the skin, gut, and lung, where they take up residence near surfaces that meet the outside world. Adhesion molecules and chemokines (CCL2, CCL3, CCL5) guide this migration through receptors such as CCR2 and CCR5.
Maturation: the moment dendritic cells switch jobs
Maturation is the most important transition in a dendritic cell's life. When pattern recognition receptors including TLRs, C-type lectin receptors, and the cytosolic cGAS-STING pathway detect microbial or damage signals, the cell flips a switch:
- Antigen uptake decreases.
- MHC class I and II expression climbs.
- Costimulatory molecules CD80 and CD86 rise sharply.
- The chemokine receptor CCR7 turns on, drawing the cell toward lymph nodes.
This is the same switch that mature vaccine adjuvants are designed to flip [8].
Reference range (with a caveat)
A small study of healthy adults reported peripheral blood dendritic cells at 0.16–0.68% of leukocytes, 0.55–1.63% of mononuclear cells, and 13–37 × 10⁶/L [1]. However, clinical medicine does not currently use standard reference intervals for dendritic cells in routine blood work; their quantification is strictly reserved for specialized research or targeted diagnostic settings.
Routine full blood counts do not report dendritic cells; specialized flow cytometry is needed.
Functions of Dendritic Cells

Antigen Capture and Processing
In peripheral tissues, dendritic cells sample anything that could be a problem — bacteria, viruses, dying cells, tumor debris. The material is taken in by phagocytosis, macropinocytosis, or receptor-mediated endocytosis and is broken down inside the cell along two pathways: a proteasomal pathway for things made inside the cell, and a lysosomal pathway for things brought in from outside [3].
Antigen Presentation
The resulting peptide fragments are loaded onto MHC molecules and pushed to the surface:
- MHC class I displays peptides to CD8⁺ cytotoxic T cells, which kill infected cells.
- MHC class II displays peptides to CD4⁺ helper T cells, which coordinate everyone else.
- Cross-presentation, a specialty of cDC1s, places extracellular antigens onto MHC class I and activates CD8⁺ T cells against pathogens or tumor cells the dendritic cell never directly infected [8].
T Cell Activation and Polarization
Mature dendritic cells migrate to lymph nodes and meet T cells. Three signals are needed: the peptide–MHC complex (signal 1), costimulatory molecules CD80/86 (signal 2), and cytokines (signal 3). That third signal decides what kind of T cell forms:
- IL-12 drives Th1 responses for intracellular pathogens.
- IL-4 drives Th2 responses for parasites and allergens.
- TGF-β drives regulatory T cells that suppress immune responses.
Immune Tolerance
Not every encounter should trigger an attack. Dendritic cells present self-antigens in a non-activating way, leading T cells either into anergy (a kind of immune silence) or toward regulatory T-cell fates. They also produce IL-10 and TGF-β, both of which dampen immune responses. This is how the immune system avoids attacking the body itself.
Other Functions
Plasmacytoid dendritic cells dominate the antiviral type I interferon response. Other dendritic cells produce pro-inflammatory cytokines that drive inflammation, while tissue-resident populations contribute to repair and tissue maintenance.
Clinical Significance: When Dendritic Cell Numbers or Function Go Wrong
Changes in dendritic cells can be numerical (more or fewer than expected) or functional (the right number, but doing the wrong thing). Function often matters more than count.
Increased dendritic cells
Higher dendritic cell numbers or sometimes called dendrocytosis in the literature, though this is not a standard clinical diagnosis typically appear as a downstream sign of another process:
- Infections. Viral infections such as HIV, CMV, and hepatitis viruses, and some bacterial infections (tuberculosis, sepsis), commonly drive expansion and activation of dendritic cells.
- Autoimmune disease. SLE, rheumatoid arthritis, and Sjögren's syndrome involve dendritic cells presenting self-antigens and pushing chronic inflammation [2].
- Cancers. Some hematological malignancies are associated with raised dendritic cell counts.
- Chronic inflammation. Inflammatory bowel disease and psoriasis are typical examples.
- Vaccination and transplantation. Both can transiently elevate dendritic cell numbers as part of a normal immune response.
Decreased dendritic cells
Low dendritic cell counts or sometimes called dendropenia, again not a formal diagnosis appear in:
- Primary immunodeficiencies with defects in DC development (e.g., IRF8 mutations) [4].
- HIV infection, which damages both DCs directly and the CD4⁺ T cells they depend on.
- Severe malnutrition, which impairs immune cell production generally.
- Hematological cancers such as acute myeloid leukemia.
- Chemotherapy and radiotherapy.
- Immunosuppressive drugs: corticosteroids, calcineurin inhibitors (cyclosporine, tacrolimus), and similar agents.
- Aging, which contributes to immunosenescence.
Functional alterations
Even when counts are normal, dendritic cells can misbehave. In chronic infection, pathogens can blunt their antigen-processing machinery. In autoimmunity, they break tolerance and present self-antigens with full activation. In cancer, tumor cells release factors that turn dendritic cells tolerogenic, helping the tumor hide from T cells [8]. In dendritic cell deficiency, antigen presentation fails, T cells are poorly activated, and antiviral interferon production drops which is a particularly damaging combination when plasmacytoid dendritic cells are affected.
How Dendritic Cells Are Investigated in the Lab
Counting and characterizing dendritic cells requires specialized methods, because they are scarce in blood and lack a single defining marker.
Flow cytometry is the standard. Panels of fluorescent antibodies against markers such as CD11c, CD123, CD141, CD1c, and HLA-DR allow each major subset to be identified and counted [1,2].
Immunohistochemistry localizes dendritic cells inside tissue sections which is useful for understanding where they sit in tumors or autoimmune lesions.
Functional assays test what they can actually do. The mixed leukocyte reaction measures their ability to drive T-cell proliferation; antigen presentation and cytokine production assays add further detail.
Emerging techniques include single-cell RNA sequencing, which revealed the DC3 and AXL⁺SIGLEC6⁺ populations [4,5], and mass cytometry (CyTOF), which measures dozens of markers simultaneously. More recently, spatial transcriptomics has revolutionized the field. While single-cell RNA sequencing reveals what dendritic cells are doing, spatial transcriptomics maps exactly where they are doing it within intact tissues, uncovering how they organize critical "immune hubs" within solid tumors [12].
Therapeutic Targeting of Dendritic Cells
Because dendritic cells decide whether the adaptive immune system attacks or tolerates, they are an attractive lever for therapy.
Dendritic cell vaccines for cancer
The clearest example of a dendritic cell-based therapy in clinical use is Sipuleucel-T (Provenge), approved by the FDA in 2010 for metastatic castration-resistant prostate cancer. It works by loading a patient's own antigen-presenting cells with a prostate cancer antigen and infusing them back [7].
While Sipuleucel-T proved the concept of dendritic cell therapies, ex vivo generation by taking cells out, engineering them, and putting them back, is complex and costly. The modern frontier has shifted dramatically toward in vivo targeting using mRNA-lipid nanoparticles (LNPs) [13].
Two broad strategies dominate current research [2,8]:
- In vivo targeting (The modern standard): Using specialized lipid nanoparticles or biomaterial platforms to deliver tumor neoantigen mRNA directly to dendritic cells inside the patient's body. This instructs the dendritic cells to manufacture, process, and present the antigens internally, bypassing the need for cell extraction [13].
- Ex vivo loading (The classical approach): Collecting monocyte-derived dendritic cells from a patient, loading them with tumor peptides or mRNA, and reinfusing them (e.g., the TriMixDC platform).
Recent trials increasingly combine dendritic cell vaccines with immune checkpoint inhibitors such as anti-PD-1 or anti-CTLA-4. The rationale is straightforward: the vaccine creates tumor-specific T cells, and the checkpoint inhibitor stops the tumor from switching them off [6,8].
Tolerogenic dendritic cells for autoimmune disease
The opposite goal by calming the immune system uses tolerogenic dendritic cells (tolDCs). These are generated in vitro using agents like vitamin D3, dexamethasone, or genetic modification to produce dendritic cells that suppress rather than activate. Early-phase trials are exploring tolDCs in type 1 diabetes, rheumatoid arthritis, and multiple sclerosis.
Targeting dendritic cells in infections
In chronic infection, the aim is usually to reactivate sluggish dendritic cells. TLR agonists and other immunostimulatory molecules are being studied to boost dendritic cell maturation and antigen presentation. Better targeting of pathogen-derived antigens to dendritic cell surface receptors is another active area.
What is next
Genetically modified dendritic cells, dendritic cells embedded in biomaterial scaffolds, and strategies that direct dendritic cell migration into specific lymph nodes or tumors all represent active frontiers [2,8]. None of these is a magic bullet, but the field has moved from "can we make a dendritic cell vaccine?" — answered yes years ago — to "how do we make it work consistently in solid tumors?"
Frequently Asked Questions (FAQs)
What do dendritic cells actually do?
Dendritic cells are the immune system's scouts. They patrol tissues such as the skin, gut, and lungs, swallow up bits of pathogens or damaged cells, then travel to a nearby lymph node and show those fragments to T cells. That introduction is what kicks off a targeted, adaptive immune response.
How are dendritic cells different from macrophages?
Both can swallow pathogens and present antigens, but dendritic cells are far better at activating naive T cells (T cells that have never seen an antigen before). Macrophages mostly clean up debris and amplify ongoing immune responses. Think of dendritic cells as recruiters and macrophages as front-line cleanup crew.
What are the main types of dendritic cells?
The classical groups are conventional DCs (split into cDC1 and cDC2) and plasmacytoid DCs (pDCs). Modern single-cell studies have added DC3, monocyte-derived DCs (mo-DCs), and a transitional AXL⁺SIGLEC6⁺ subset to the picture. Each type favors a different kind of immune response.
Are dendritic cells used in cancer treatment?
Yes. Sipuleucel-T, approved in 2010 for advanced prostate cancer, is a dendritic cell-based therapy. More recent research focuses on personalized DC vaccines loaded with tumor neoantigens, often combined with checkpoint inhibitors like pembrolizumab.
Can you have too few dendritic cells?
Yes. Low dendritic cell numbers can occur in primary immunodeficiencies, untreated HIV, severe malnutrition, after chemotherapy or radiotherapy, and with long-term immunosuppressive drugs. The clinical consequence is weakened activation of T cells and reduced antiviral defense, especially when plasmacytoid DCs are affected.
Do dendritic cells appear on a regular blood test?
No. Routine full blood counts do not report dendritic cells because they make up less than 1% of circulating white cells. Specialized flow cytometry is needed to count and characterize them, usually in research or specialist immunology labs.
Glossary of Related Medical Terms
- Antigen — any molecule that the immune system can recognize and respond to. Often a fragment of a microbe, but can be a tumor protein or even a self-protein in autoimmune disease.
- Antigen-presenting cell (APC) — an immune cell that displays processed antigen fragments on its surface so T cells can recognize them. Dendritic cells, macrophages, and B cells are the main "professional" APCs.
- MHC (Major Histocompatibility Complex) — surface proteins that hold antigen fragments up for T cells to see. Class I shows fragments from inside the cell; Class II shows fragments taken in from outside.
- Cross-presentation — the unusual trick of taking up outside antigens and displaying them on MHC Class I, allowing killer T cells to be alerted to viruses or tumor cells. cDC1s are particularly good at this.
- Maturation — the change a dendritic cell undergoes after it senses danger: it stops gobbling up material, ramps up MHC and CD80/86, and migrates to a lymph node to find T cells.
- Tolerance (immune tolerance) — the immune system's ability to not attack the body's own tissues. Dendritic cells help maintain this by presenting self-antigens in a non-activating way.
- Type I interferons (IFN-α/β) — antiviral signaling proteins. Plasmacytoid DCs are the body's biggest producers.
- Pattern recognition receptor (PRR) — sensors on or inside immune cells that detect microbial features. Toll-like receptors (TLRs) are the best-known family.
- Toll-like receptor (TLR) — a class of PRRs that recognizes specific microbial signatures (e.g., TLR7 and TLR9 sense viral nucleic acids).
- Neoantigen — a novel protein fragment made by a mutated tumor that is not found in healthy cells, making it an attractive vaccine target.
- Sipuleucel-T — the first FDA-approved dendritic cell-based therapy, used in advanced prostate cancer.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Haller Hasskamp, J., Zapas, J. L., & Elias, E. G. (2005). Dendritic cell counts in the peripheral blood of healthy adults. American journal of hematology, 78(4), 314–315. https://doi.org/10.1002/ajh.20296
- Patente, T. A., Pinho, M. P., Oliveira, A. A., Evangelista, G. C. M., Bergami-Santos, P. C., & Barbuto, J. A. M. (2019). Human Dendritic Cells: Their Heterogeneity and Clinical Application Potential in Cancer Immunotherapy. Frontiers in immunology, 9, 3176. https://doi.org/10.3389/fimmu.2018.03176
- Collin, M., & Bigley, V. (2018). Human dendritic cell subsets: an update. Immunology, 154(1), 3–20. https://doi.org/10.1111/imm.12888
- Segura E. (2022). Human dendritic cell subsets: An updated view of their ontogeny and functional specialization. European journal of immunology, 52(11), 1759–1767. https://doi.org/10.1002/eji.202149632
- Villani, A. C., Satija, R., Reynolds, G., Sarkizova, S., Shekhar, K., Fletcher, J., Griesbeck, M., Butler, A., Zheng, S., Lazo, S., Jardine, L., Dixon, D., Stephenson, E., Nilsson, E., Grundberg, I., McDonald, D., Filby, A., Li, W., De Jager, P. L., Rozenblatt-Rosen, O., … Hacohen, N. (2017). Single-cell RNA-seq reveals new types of human blood dendritic cells, monocytes, and progenitors. Science (New York, N.Y.), 356(6335), eaah4573. https://doi.org/10.1126/science.aah4573
- Carreno, B. M., Magrini, V., Becker-Hapak, M., Kaabinejadian, S., Hundal, J., Petti, A. A., Ly, A., Lie, W. R., Hildebrand, W. H., Mardis, E. R., & Linette, G. P. (2015). Cancer immunotherapy. A dendritic cell vaccine increases the breadth and diversity of melanoma neoantigen-specific T cells. Science (New York, N.Y.), 348(6236), 803–808. https://doi.org/10.1126/science.aaa3828
- Kantoff, P. W., Higano, C. S., Shore, N. D., Berger, E. R., Small, E. J., Penson, D. F., Redfern, C. H., Ferrari, A. C., Dreicer, R., Sims, R. B., Xu, Y., Frohlich, M. W., Schellhammer, P. F., & IMPACT Study Investigators (2010). Sipuleucel-T immunotherapy for castration-resistant prostate cancer. The New England journal of medicine, 363(5), 411–422. https://doi.org/10.1056/NEJMoa1001294
- Wculek, S. K., Cueto, F. J., Mujal, A. M., Melero, I., Krummel, M. F., & Sancho, D. (2020). Dendritic cells in cancer immunology and immunotherapy. Nature reviews. Immunology, 20(1), 7–24. https://doi.org/10.1038/s41577-019-0210-z
- Pearce, E. J., & Everts, B. (2015). Dendritic cell metabolism. Nature reviews. Immunology, 15(1), 18–29. https://doi.org/10.1038/nri3771
- Dutertre, C. A., Becht, E., Irac, S. E., Khalilnezhad, A., Narang, V., Khalilnezhad, S., Ng, P. Y., van den Hoogen, L. L., Leong, J. Y., Lee, B., Chevrier, M., Zhang, X. M., Yong, P. J. A., Koh, G., Lum, J., Howland, S. W., Mok, E., Chen, J., Larbi, A., Tan, H. K. K., … Ginhoux, F. (2019). Single-Cell Analysis of Human Mononuclear Phagocytes Reveals Subset-Defining Markers and Identifies Circulating Inflammatory Dendritic Cells. Immunity, 51(3), 573–589.e8. https://doi.org/10.1016/j.immuni.2019.08.008
- Doebel, T., Voisin, B., & Nagao, K. (2017). Langerhans Cells - The Macrophage in Dendritic Cell Clothing. Trends in immunology, 38(11), 817–828. https://doi.org/10.1016/j.it.2017.06.008
- Pelka, K., Hofree, M., Chen, J. H., Sarkizova, S., Pirl, J. D., Jorgji, V., Bejnood, A., Dionne, D., Ge, W. H., Xu, K. H., Chao, S. X., Zollinger, D. R., Lieb, D. J., Reeves, J. W., Fuhrman, C. A., Hoang, M. L., Delorey, T., Nguyen, L. T., Waldman, J., Klapholz, M., … Hacohen, N. (2021). Spatially organized multicellular immune hubs in human colorectal cancer. Cell, 184(18), 4734–4752.e20. https://doi.org/10.1016/j.cell.2021.08.003
- Kranz, L. M., Diken, M., Haas, H., Kreiter, S., Loquai, C., Reuter, K. C., Meng, M., Fritz, D., Vascotto, F., Hefesha, H., Grunwitz, C., Vormehr, M., Hüsemann, Y., Selmi, A., Kuhn, A. N., Buck, J., Derhovanessian, E., Rae, R., Attig, S., Diekmann, J., … Sahin, U. (2016). Systemic RNA delivery to dendritic cells exploits antiviral defence for cancer immunotherapy. Nature, 534(7607), 396–401. https://doi.org/10.1038/nature18300