Key Takeaways
Polycythemia vera is a chronic blood cancer of the bone marrow that produces too many red blood cells, and often too many platelets and white cells as well. Roughly 95–97% of cases are driven by a mutation in the JAK2 gene [1].
- Symptoms ▾: The dominant clinical danger is thrombosis (blood clots), which is the leading cause of death in polycythemia vera; symptoms such as headache, dizziness, itching after a warm shower, and a flushed face come from thicker blood and overactive marrow [8].
- Investigations ▾: Diagnosis combines an elevated hematocrit, a low serum erythropoietin (EPO), a positive JAK2 V617F or exon 12 mutation, and a bone marrow biopsy, applied through the 2022 ICC or WHO 5th edition criteria [9,10].
- Treatment and Management ▾: Every patient receives low-dose aspirin and phlebotomy to keep the hematocrit below 45%; high-risk patients (age ≥60 or prior clot) add cytoreductive drugs such as hydroxyurea or ropeginterferon alfa-2b [4,7].
- Prognosis ▾: About 10–15% of patients eventually transition to post-PV myelofibrosis (the "spent phase") over 10–20 years, and 2–14% transform to acute myeloid leukemia at 10 years [1,2].
*Click ▾ for more information
What is Polycythemia, and Where Does PV fit?
Before naming the disease, it helps to understand the umbrella term. Polycythemia simply means too many red blood cells in the blood. It is a finding, not a diagnosis. The same lab number can be produced by very different mechanisms, and getting the mechanism right is what determines treatment.
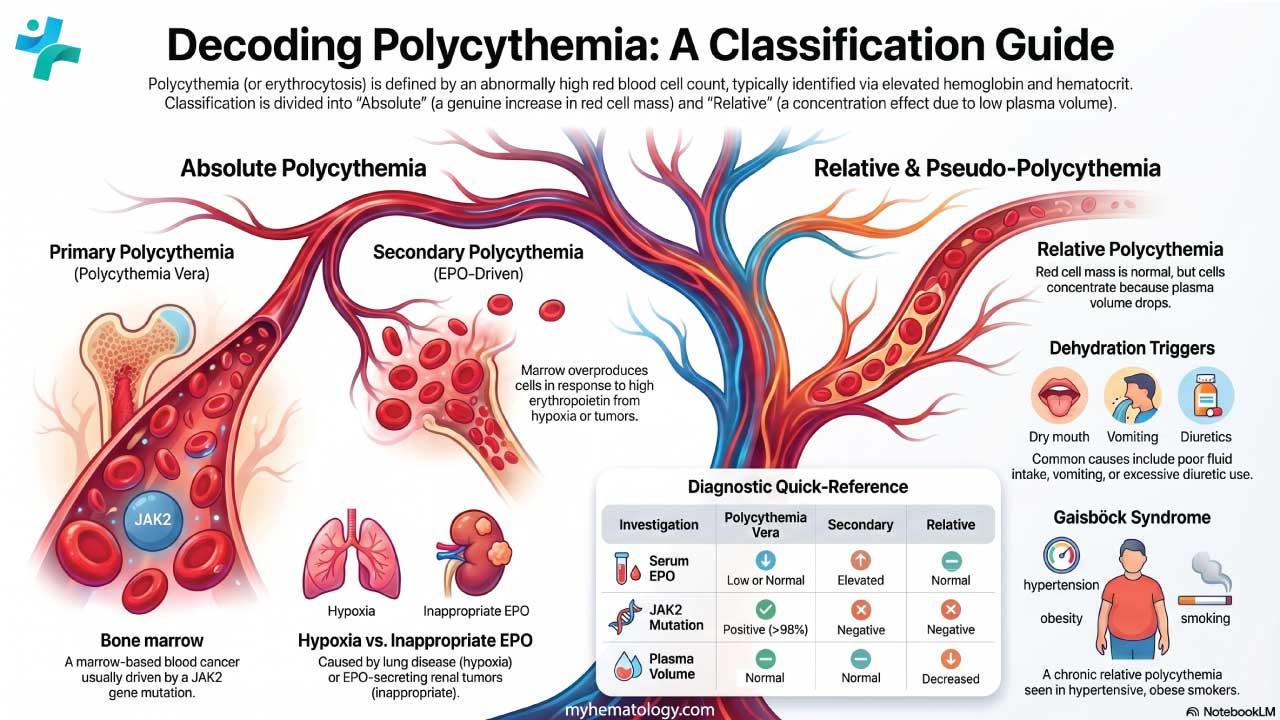
Polycythemia is split into two broad categories:
Absolute polycythemia is a true increase in the total number of red cells in the body. It comes in two flavors. Primary polycythemia means the bone marrow itself is the problem and polycythemia vera is by far the most common cause. Secondary polycythemia means the marrow is responding (correctly or incorrectly) to a signal from somewhere else, usually a low-oxygen state or a tumor that secretes erythropoietin.
Relative (or apparent) polycythemia is a different beast: the red cell number is normal, but the plasma volume has shrunk, so the concentration looks high. Dehydration is the most common cause. Gaisböck syndrome typically described in middle-aged, hypertensive, smoking men is a classic textbook example.
This distinction matters clinically because aggressive treatment of the wrong category can harm the patient.
What Is Polycythemia Vera?
Polycythemia vera (PV) is a chronic myeloproliferative neoplasm in which the bone marrow autonomously overproduces red blood cells, and frequently white cells and platelets as well [1]. The blood becomes thicker, flows less efficiently through small vessels, and clots more readily. That single mechanical change drives most of the disease's clinical picture, from the flushed face and itching to the strokes and heart attacks that make polycythemia vera dangerous when untreated.
Pathogenesis and Pathophysiology
Bone Marrow Loses Its Brakes
In healthy marrow, blood cell production is tightly regulated. Hormones bind to receptors on stem and progenitor cells, signals are transmitted into the cell, and the marrow produces only as many red cells, white cells, and platelets as the body needs.
In PV, that regulation breaks. The marrow produces blood cells regardless of what the body asks for. Red cell overproduction (erythrocytosis) is the most prominent feature, but white cell counts (leukocytosis) and platelet counts (thrombocytosis) are also elevated in many patients. Together this is called panmyelosis.
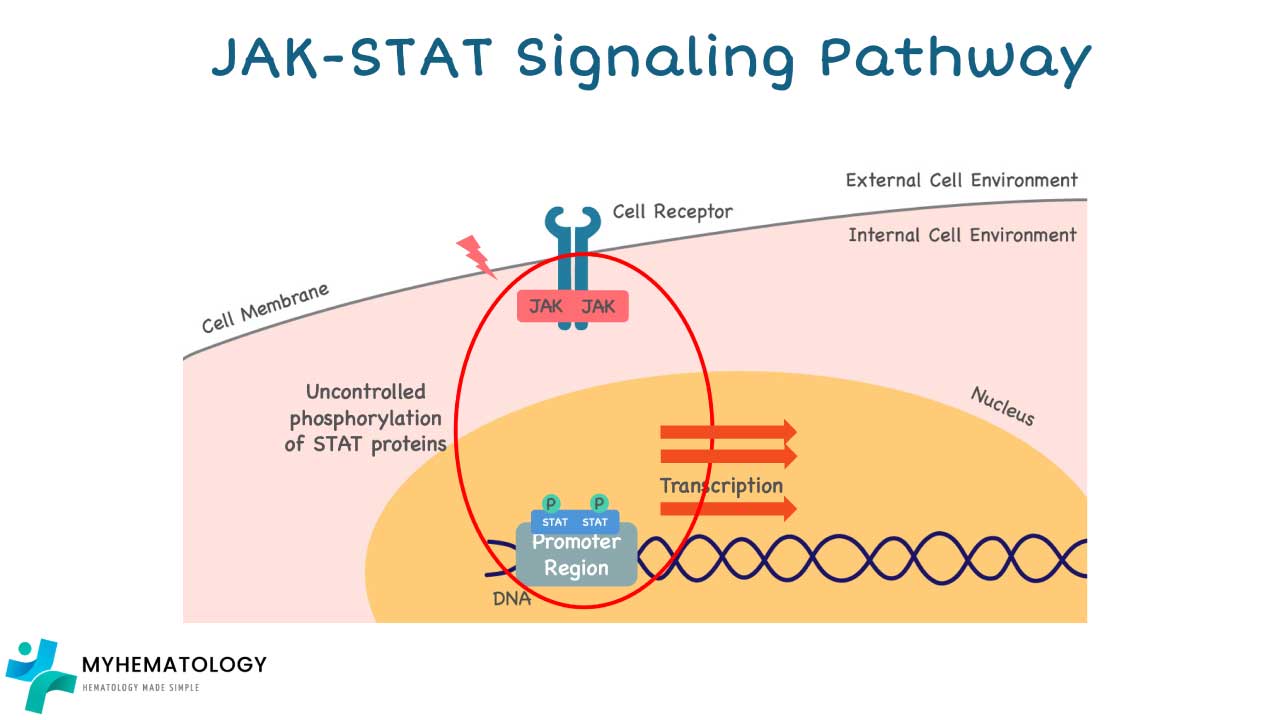
A Stuck Switch in the JAK-STAT Pathway
The molecular driver is almost always a mutation in JAK2, a gene that codes for an enzyme inside blood-cell precursors. Normally, JAK2 only switches on when erythropoietin (EPO) or a related hormone binds to the cell surface. The activated JAK2 then turns on STAT proteins, which travel to the nucleus and trigger blood-cell production.
In polycythemia vera, JAK2 itself is mutated:
- The V617F mutation is found in roughly 95–97% of PV patients [1,13].
- Exon 12 mutations account for most of the rest.
These mutations lock JAK2 in the "on" position. The marrow no longer waits for an EPO signal but it makes red cells continuously. CALR and MPL mutations, which drive the related myeloproliferative neoplasms essential thrombocythemia and primary myelofibrosis, are very rarely seen in PV.
Why Thicker Blood Causes Real Harm
Once red cell mass climbs, blood viscosity rises with it. Sluggish blood through narrow vessels means reduced oxygen delivery to tissues, paradoxical fatigue (despite the apparent excess of oxygen-carriers), and a sharp increase in the risk of clots in arteries and veins. This is why thrombosis is the main cause of death in polycythemia vera [8].
Risk Factors
The exact trigger for the JAK2 mutation is unknown, but several factors are linked to higher PV risk:
- Age. Most patients are diagnosed between 60 and 65; risk climbs after age 40.
- Family history. Having a first-degree relative with PV slightly raises risk, though most cases are sporadic.
- Smoking. A possible contributor, though the mechanism is not fully understood.
Polycythemia Vera Symptoms and Signs
Symptoms in polycythemia vera fall into a few mechanism-based clusters. Recognizing these clusters helps you predict, in clinic or on a test, what a patient with PV is likely to report.
In modern clinical practice, symptom burden is formally quantified using standardized tools like the MPN Symptom Assessment Form Total Symptom Score (MPN-SAF TSS). Tracking this score objectively is critical because a rising symptom burden can be an early indicator of disease progression, often preceding any visible changes in blood counts and prompting a re-evaluation of therapy [11].
Symptoms from Thicker Blood and Sluggish Flow
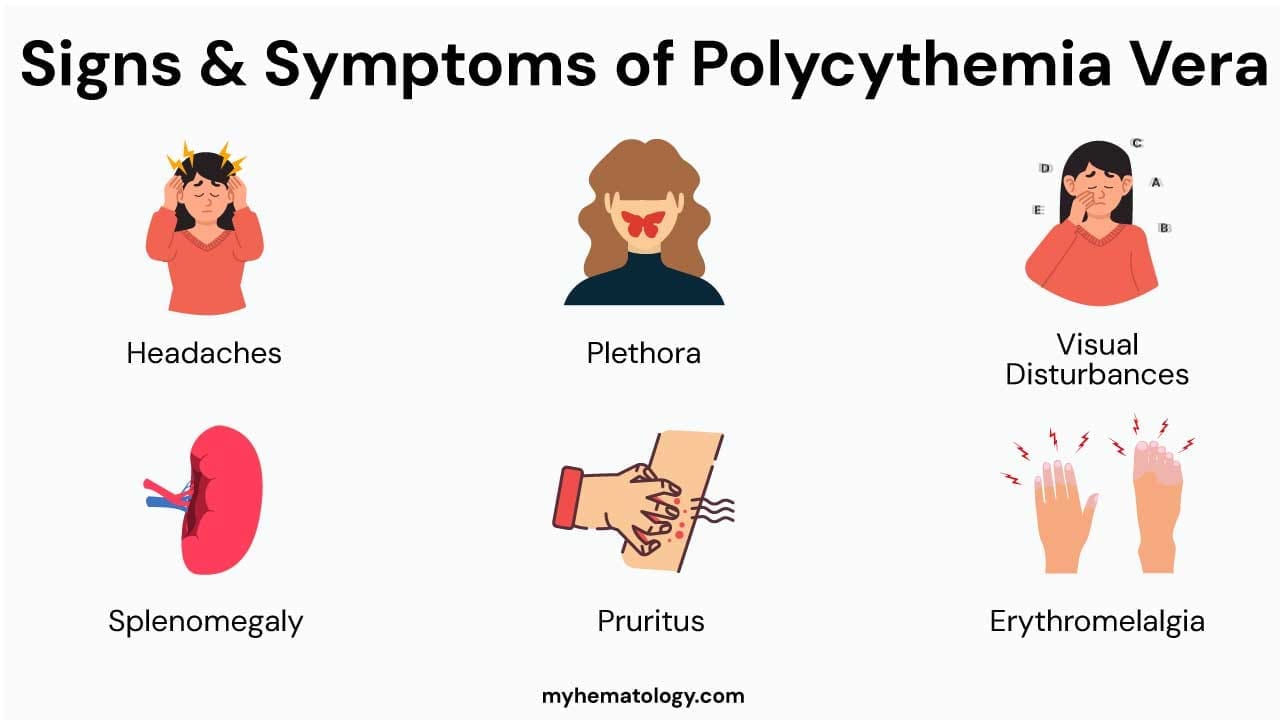
Headache, dizziness, lightheadedness, blurred or transient vision loss, tinnitus, and tingling or burning in the hands and feet (paresthesias) all stem from impaired microcirculation. Severe cases can produce transient ischemic attacks (TIAs) or stroke. Fatigue is common and often debilitating, even though oxygen-carrying capacity is technically high — efficient delivery, not capacity, is the bottleneck.
Plethora
The hallmark visible sign of polycythemia vera. Patients have a flushed, ruddy, sometimes purplish appearance of the face, lips, and mucous membranes from circulating red cells near the skin surface.
Splenomegaly
The enlarged spleen presses on the stomach and other abdominal organs, producing left upper quadrant fullness, early satiety (feeling full after eating only a little), and sometimes pain. Splenic infarction is uncommon but possible.
Symptoms from Platelets and Endothelium
Three are characteristic:
- Aquagenic pruritus — intense itching after contact with water (typically warm), without visible rash. Up to half of patients experience it. The mechanism likely involves basophil and mast cell activation, with histamine and prostaglandin release in the skin.
- Erythromelalgia — burning pain, redness, and warmth in the hands or feet, often triggered by heat or exercise. It is caused by platelet-mediated microvascular clots and usually responds quickly to low-dose aspirin.
- Microvascular events — TIAs, atypical chest pain, and visual disturbances from tiny clots.

Symptoms from High Cell Turnover
The breakdown of so many blood cells releases uric acid, which can crystallize in joints and cause gout. Some patients also report night sweats and mild weight loss, especially as disease progresses.
Paradoxical Bleeding
Counterintuitively, some patients bleed more easily like nosebleeds, easy bruising, gum bleeding. This is often due to acquired von Willebrand syndrome at very high platelet counts, where large von Willebrand factor multimers are pathologically cleaved.
Asymptomatic Presentation
A significant minority of PV cases are picked up incidentally on a routine complete blood count. This is one reason guideline-based investigation of any unexplained erythrocytosis matters.
Investigations in Polycythemia Vera
Diagnosing polycythemia vera is a structured exercise: confirm the erythrocytosis is real, prove the bone marrow is the source, and identify the driver mutation.
Complete Blood Count (CBC) with Differential
In PV, the CBC typically shows:
- Elevated red blood cell count and hemoglobin.
- Hematocrit above 49% in men and 48% in women.
- Often normal or mildly elevated white blood cell and platelet counts.
Serum Erythropoietin (EPO) Level
This is the single most useful pointer toward primary versus secondary disease. In PV, autonomous red cell production suppresses EPO, so the level is low or subnormal. In secondary polycythemia, EPO is elevated as the body responds to hypoxia or an EPO-secreting tumor.
Molecular Mutation Testing
The decisive genetic test:
- JAK2 V617F is found in approximately 95–97% of PV patients [1,13].
- JAK2 exon 12 mutations account for most of the remaining cases.
A negative JAK2 result with low EPO and persistent erythrocytosis should prompt a search for rare hereditary erythrocytoses (for example, EPO receptor mutations).
Bone Marrow Biopsy
The biopsy in PV typically shows hypercellularity for age, with proliferation of all three lineages and clusters of pleomorphic, mature megakaryocytes without atypia. This pattern is part of the formal diagnostic criteria.
Next-Generation Sequencing (NGS)
While JAK2 remains the primary diagnostic target, Next-Generation Sequencing (NGS) is increasingly becoming the standard of care for comprehensive risk assessment. Up to a third of PV patients carry additional, non-driver mutations (such as ASXL1, TET2, SRSF2, or IDH2). While these do not cause PV, their presence can significantly alter a patient’s prognosis and increase the long-term risk of progression to myelofibrosis or acute myeloid leukemia [12].
Other Investigations
Imaging (ultrasound or CT) confirms splenomegaly. Erythrocyte sedimentation rate (ESR) is often low in PV but is non-specific.
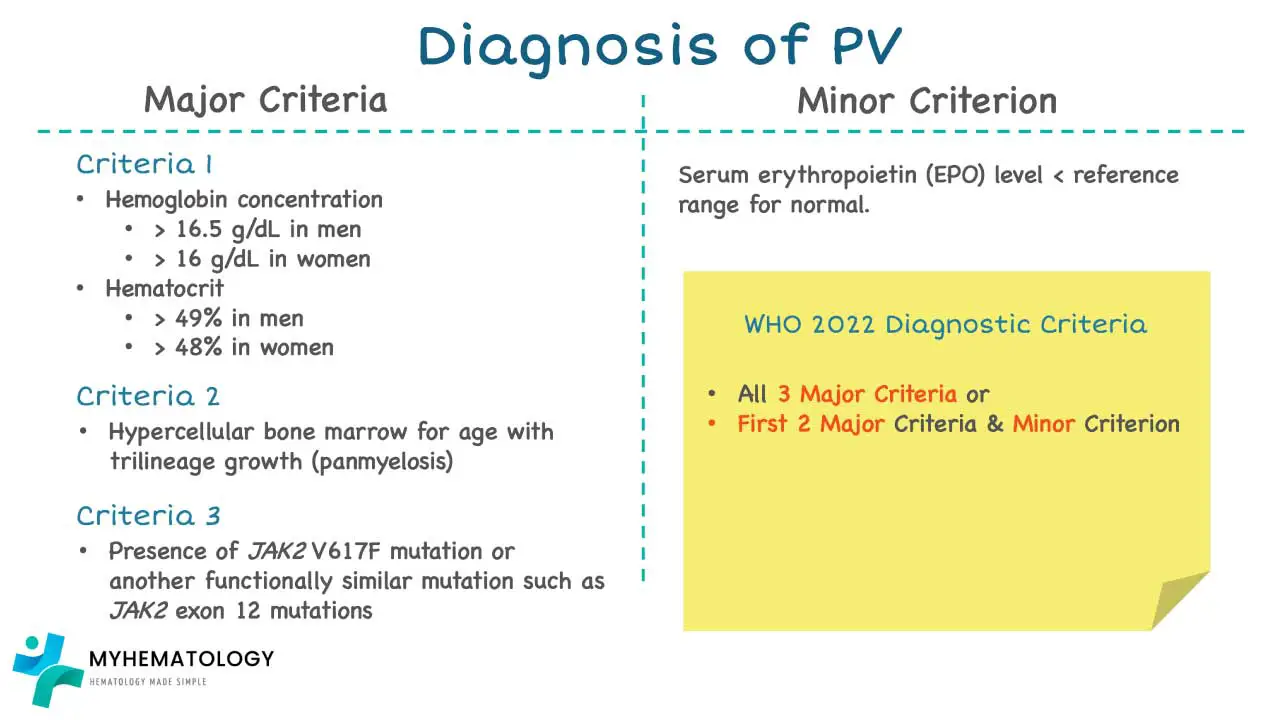
Diagnostic Criteria (2022)
Two parallel classifications are now in use: the 2022 World Health Organization 5th edition and the International Consensus Classification (ICC) [9,10]. They largely agree for PV and require either all three major criteria or the first two major criteria plus the minor criterion:
Major criteria
- Increased hemoglobin, hematocrit, or red blood cell mass.
- Hypercellular bone marrow biopsy with trilineage proliferation and prominent erythroid and granulocytic lineages, with mature, pleomorphic megakaryocytes.
- JAK2 V617F or JAK2 exon 12 mutation.
Minor criterion
- Subnormal serum EPO level.
Differential Diagnosis
The clinical task is distinguishing primary polycythemia (PV) from secondary polycythemia and from relative polycythemia. Serum EPO and JAK2 status do most of the work.
Relative (Apparent) Polycythemia
Plasma volume is low, red cell mass is normal. Causes include dehydration, severe burns, diuretic use, and Gaisböck syndrome.
Secondary Polycythemia from Appropriate EPO Production
The body raises EPO in response to genuine hypoxia: COPD, obstructive sleep apnea, high altitude living, cyanotic congenital heart disease, high-affinity hemoglobins (such as Hb Chesapeake), and the carboxyhemoglobinemia of heavy smokers.
Secondary Polycythemia from Inappropriate EPO Production
EPO is high despite normal oxygenation, typically because of an EPO-secreting tumor: renal cell carcinoma, hepatocellular carcinoma, uterine leiomyomas, or cerebellar hemangioblastoma.
Comparative Diagnostic Markers
| Feature | Polycythemia Vera | Secondary Polycythemia | Relative Polycythemia |
|---|---|---|---|
| Red cell mass | Increased | Increased | Normal |
| Plasma volume | Normal / Increased | Normal | Decreased |
| Serum EPO | Low / subnormal | High / elevated | Normal |
| JAK2 mutation | Positive (95–97%) | Negative | Negative |
| WBC / platelets | Often elevated | Normal | Normal |
| Splenomegaly | Common | Absent | Absent |
Complications
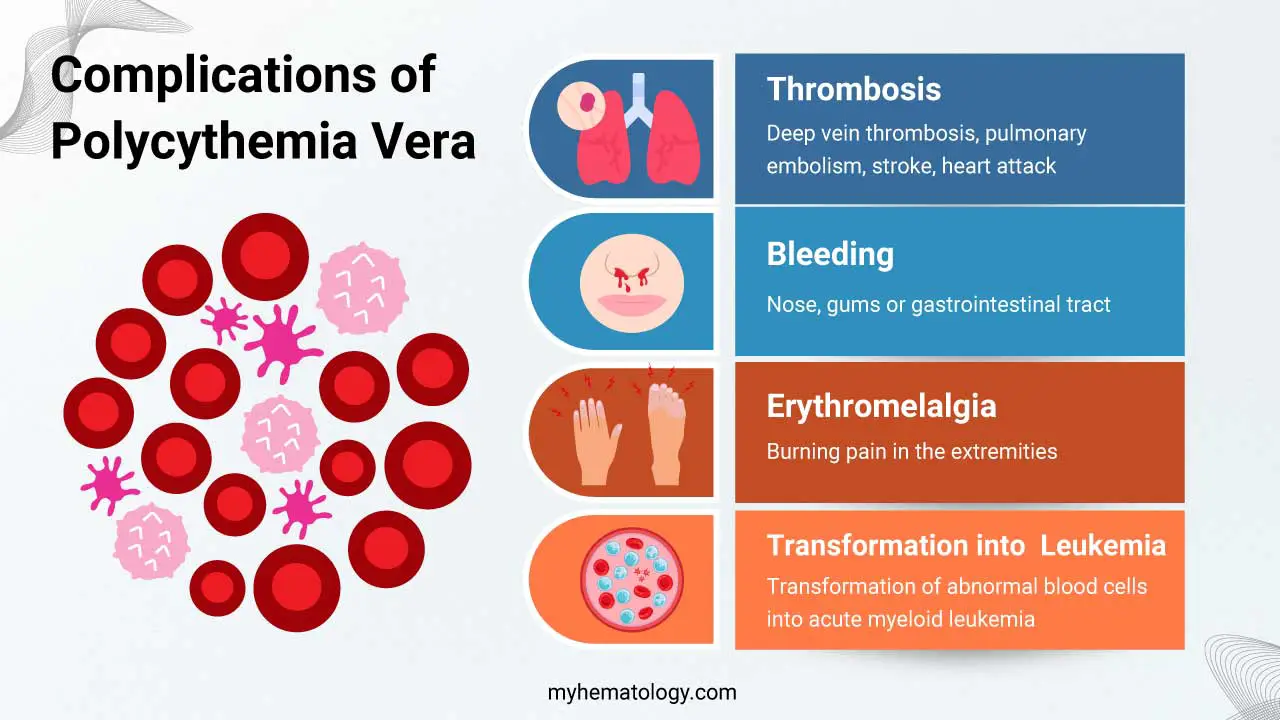
Thrombosis
The most common and most serious complication of polycythemia vera, and the leading cause of death [8]. Sites include:
- Deep vein thrombosis (DVT): swelling, pain, redness in a leg.
- Pulmonary embolism: sudden breathlessness, chest pain, low oxygen saturation.
- Stroke: focal weakness, speech changes, vision loss.
- Myocardial infarction: chest pain, breathlessness, sweating.
PV also increases risk of unusual-site thromboses such as Budd-Chiari syndrome (hepatic venous outflow obstruction), often the presenting event in younger women.
Bleeding
Less common than clots but real. Acquired von Willebrand syndrome and platelet dysfunction explain most cases; sites include nose, gums, and gastrointestinal tract.
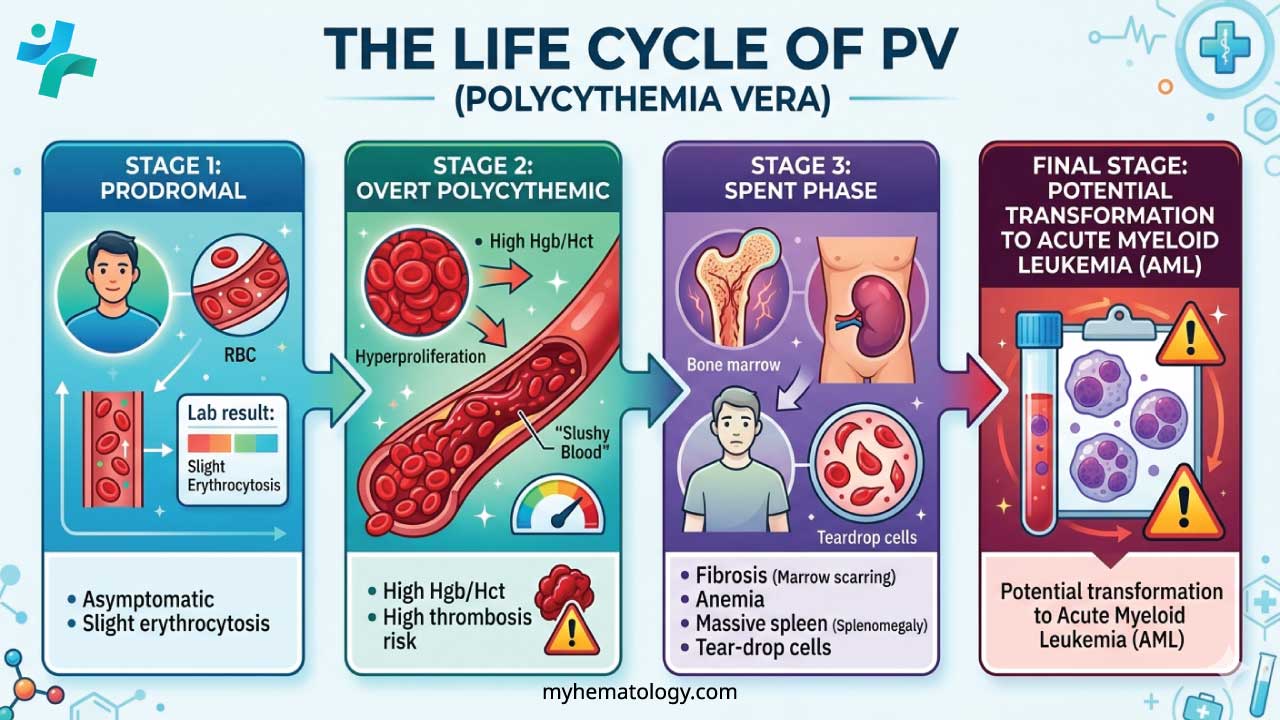
The "Spent Phase" (Post-PV Myelofibrosis)
About 10–15% of patients transition to post-PV myelofibrosis over 10–20 years [1]. Cytokines released by hyperactive megakaryocytes drive the marrow to scar with collagen fibrosis. Three findings define the picture:
- Paradoxical anemia: patients who once needed phlebotomies to lower their hemoglobin now become anemic and may need transfusions.
- Massive splenomegaly: with the marrow shut down, blood production shifts to the spleen and liver (extramedullary hematopoiesis).
- Leukoerythroblastic blood film with teardrop cells (dacrocytes): immature white and red precursors squeezed out of the fibrotic marrow.
Constitutional symptoms like drenching night sweats, weight loss, low-grade fever typically intensify.
Transformation to Acute Leukemia
This is the most feared late complication. Across published cohorts, the risk of leukemic transformation in PV is approximately 2–14% at 10 years and 5–19% at 15 years, with substantial variation depending on cohort and exposure to older cytotoxic drugs [1,2]. Most cases are acute myeloid leukemia (AML), and prognosis after transformation is poor (median survival under 6 months in some series).
Treatment and Management
The goals of treatment are simple to state: prevent thrombosis (the leading killer), control symptoms, and slow disease progression. The intensity is tailored to the patient.
Risk Stratification
- High risk: age ≥60 years or any prior arterial or venous thrombosis.
- Low risk: neither feature.
Phlebotomy
The cornerstone of treatment. Removing 450–500 mL of blood lowers red cell mass directly. The target hematocrit is below 45%, supported by the randomized CYTO-PV trial which showed roughly four times fewer cardiovascular events at this target than at 45–50% [7]. While <45% is the universal standard, current guidelines and expert consensus increasingly recommend a stricter target of <42% for female patients to account for normal physiological differences in baseline hematocrit and optimize cardiovascular protection [4].
Repeated phlebotomy induces iron deficiency, which itself helps limit erythrocyte production. Routine iron supplementation is avoided because it counteracts hematocrit control.
Low-Dose Aspirin
Recommended for almost all PV patients (typically 75–100 mg daily) unless contraindicated by major bleeding history or aspirin allergy. It reduces the risk of arterial thrombosis and is particularly effective for erythromelalgia and microvascular symptoms.
Cytoreductive Therapy
Adding a drug that lowers blood cell production is mandatory in high-risk patients and considered in low-risk patients with poor phlebotomy tolerance, progressive splenomegaly, or refractory symptoms.
Hydroxyurea has been the long-standing first-line option. It inhibits ribonucleotide reductase and reduces all blood cell lines. Dose is titrated against the CBC, with monitoring for myelosuppression, mucositis, and skin changes. Long-term use carries a small but recognized increased risk of non-melanoma skin cancers.
Ropeginterferon alfa-2b (Besremi) received FDA approval for PV in 2021 and is now listed by the National Comprehensive Cancer Network (NCCN) as a preferred first-line cytoreductive therapy for both low-risk symptomatic and high-risk PV [3,4]. It is a long-acting, monopegylated interferon given subcutaneously. Long-term clinical data demonstrates that ropeginterferon can significantly reduce the JAK2 allele burden (the percentage of mutated cells in the marrow), offering true disease-modifying potential. Because of this ability to act on the underlying clonal architecture, it is increasingly favored over hydroxyurea for younger patients to potentially delay long-term disease progression [13]. Side effects include flu-like symptoms, fatigue, and mood changes; thyroid and autoimmune monitoring is recommended. It is also the preferred cytoreductive option in younger patients and during pregnancy.
Ruxolitinib is an oral JAK1/JAK2 inhibitor approved for PV patients who are intolerant or resistant to hydroxyurea. It is particularly useful for refractory aquagenic pruritus and symptomatic splenomegaly. Monitoring is needed for cytopenias, infection risk, and non-melanoma skin cancers.
Anagrelide mainly lowers platelets and has limited use in PV, where erythrocyte control matters more.
Emerging Therapy: Rusfertide
Rusfertide is a first-in-class hepcidin mimetic given by subcutaneous injection. It reduces the iron available for red cell production by trapping iron inside cells (such as macrophages and enterocytes) via the inhibition of ferroportin. This effectively starves the bone marrow of the iron needed to overproduce red blood cells, virtually eliminating the need for routine therapeutic phlebotomies [6]. The Phase 3 VERIFY trial showed that 77% of phlebotomy-dependent PV patients achieved a clinical response on rusfertide as add-on to standard care, compared with 33% on placebo [5]. The FDA accepted a New Drug Application for rusfertide in 2026 under Priority Review, with a target action date in the third quarter of 2026 [5,6]. If approved, rusfertide will be the first hepcidin-pathway therapy in polycythemia vera.
Symptom Management
- Pruritus: antihistamines, paroxetine, narrowband UVB, and ruxolitinib for refractory cases.
- Erythromelalgia: low-dose aspirin (sometimes twice daily), heat avoidance, and cytoreduction if persistent.
- Gout: allopurinol or other urate-lowering therapy, with prophylaxis during flares.
Managing Complications
Acute thrombosis is treated with anticoagulation (heparin, warfarin, or direct oral anticoagulants) and tighter hematocrit control. Bleeding is managed by site and severity, with care to weigh aspirin or anticoagulant continuation. Transformation to myelofibrosis is treated with supportive care, JAK inhibitors for symptomatic spleen and constitutional symptoms, and, in selected younger patients, allogeneic stem cell transplant (the only potentially curative option). Transformation to AML is treated by standard AML protocols.
Lifestyle and Follow-Up
Hydration, smoking cessation, blood pressure and lipid control, and exposure to cardiovascular risk factor management are all part of long-term care. Regular CBC, spleen assessment, symptom review, and screening for skin malignancy (especially under hydroxyurea or ruxolitinib) are routine.
Prognosis
Polycythemia vera is not curable with current pharmacologic therapy, but it is highly treatable. Median survival is approximately 14–20 years, and many patients live considerably longer with good hematocrit control [8]. Outcomes have improved over the past two decades thanks to the recognition that thrombosis is the main driver of mortality and the availability of better cytoreductive options. Early diagnosis, consistent hematocrit control, and risk-appropriate cytoreduction together close most of the gap with the general population.
Frequently Asked Questions (FAQs)
What is polycythemia vera, in plain terms?
Polycythemia vera is a slow-growing blood cancer of the bone marrow. A genetic mutation, almost always in a gene called JAK2, causes the marrow to make too many red blood cells (and sometimes white cells and platelets). The blood becomes thicker and clots more easily, which is the main reason the disease is dangerous.
How is polycythemia vera diagnosed?
Diagnosis combines a high hematocrit, a low blood erythropoietin (EPO) level, and a positive test for the JAK2 mutation (V617F or, less often, exon 12). A bone marrow biopsy is usually performed to confirm the picture and exclude other myeloproliferative neoplasms. Doctors apply the 2022 WHO 5th edition or International Consensus Classification (ICC) criteria, which require either all three major criteria or the first two majors plus the minor criterion (low EPO).
Can polycythemia vera be cured?
Polycythemia vera cannot currently be cured by drugs. The only potentially curative option is an allogeneic stem cell transplant, which is reserved for selected younger patients whose disease has transformed. With proper treatment, most patients live near-normal lifespans, with a median survival of around 14–20 years, and many live substantially longer.
What is the treatment for polycythemia vera?
Every patient receives low-dose aspirin (75–100 mg/day) and phlebotomy to keep the hematocrit below 45%. High-risk patients (age ≥60 or prior clot) also get cytoreductive therapy. Hydroxyurea has long been the standard first-line drug, but the NCCN now lists ropeginterferon alfa-2b (Besremi) as a preferred first-line option for both low- and high-risk PV. Ruxolitinib, a JAK inhibitor, is used when hydroxyurea fails or for severe itch and spleen enlargement. A new drug called rusfertide is in late-stage development.
Why does itching after a warm shower happen in PV?
This symptom is called aquagenic pruritus. It is thought to involve activation of basophils and mast cells, which release histamine and other inflammatory chemicals when the skin is warmed. The itch is typically intense but leaves no visible rash. Up to half of polycythemia vera patients experience it, and it is often the symptom that finally drives them to seek care.
Will polycythemia vera turn into leukemia?
Most patients never progress to leukemia, but the risk is real. Across published studies, transformation to acute myeloid leukemia is reported in roughly 2–14% of patients at 10 years and 5–19% at 15 years, with risk rising over time and higher in those exposed to certain older cytotoxic drugs. Roughly 10–15% of patients develop post-PV myelofibrosis (the spent phase) over 10–20 years.
Glossary of Related Medical Terms
- Allogeneic stem cell transplant: Replacement of diseased bone marrow with healthy stem cells donated by another person. The only potentially curative therapy for PV but reserved for selected younger patients with high-risk transformation, because of significant treatment-related risk.
- Aquagenic pruritus: Severe itching triggered by contact with water, especially warm water. A characteristic PV symptom; the skin looks normal.
- Cytoreduction: Drug treatment that lowers the number of blood cells the bone marrow makes, used when phlebotomy and aspirin alone are not enough.
- Erythrocytosis: A measured increase in red blood cells in the blood. The most prominent feature of PV.
- Erythromelalgia: Burning pain, redness, and warmth in the hands or feet, often triggered by heat. Caused by tiny clots in small blood vessels.
- Erythropoietin (EPO): A hormone made mainly by the kidneys that signals the bone marrow to produce red blood cells. EPO is low in PV because production is no longer dependent on this signal.
- Extramedullary hematopoiesis: Blood-cell production outside the bone marrow, mainly in the spleen and liver. Common when the marrow becomes scarred.
- Hematocrit (Hct): The percentage of blood volume made up by red cells. The single most important number to control in PV; the target is below 45%.
- Hyperviscosity: Thicker, stickier blood that flows poorly through small vessels.
- JAK2 V617F mutation: A change in the JAK2 gene found in about 95–97% of PV patients. It locks the JAK2 protein in the on position, driving constant blood-cell production.
- JAK-STAT pathway: The signaling cascade that normally tells blood-cell precursors to grow and divide. PV hijacks this pathway.
- Leukoerythroblastic blood film: A smear that shows immature white cells and nucleated red cells together. Suggests the bone marrow is being squeezed (for example, by fibrosis).
- Megakaryocyte: The large bone marrow cell that produces platelets.
- Myeloproliferative neoplasm (MPN): A group of bone marrow cancers that overproduce mature blood cells. PV is one of three classic MPNs, alongside essential thrombocythemia and primary myelofibrosis.
- Phlebotomy (venesection): Therapeutic removal of a unit of blood (about 450–500 mL) to bring the hematocrit down. The cornerstone of PV treatment.
- Plethora: A flushed, ruddy, sometimes purplish complexion caused by high red cell mass.
- Post-PV myelofibrosis (spent phase): Late stage of PV in which the bone marrow scars and stops producing enough cells. Patients become anemic and the spleen enlarges.
- Risk stratification: Sorting patients into groups (low vs. high risk in PV) to decide how aggressive treatment should be. In PV, age ≥60 or any prior thrombosis = high risk.
- Thrombosis: Formation of a blood clot inside a vessel. The leading cause of death in PV.
Disclaimer: This article is intended for educational and informational purposes only . It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cerquozzi, S., & Tefferi, A. (2015). Blast transformation and fibrotic progression in polycythemia vera and essential thrombocythemia: a literature review of incidence and risk factors. Blood cancer journal, 5(11), e366. https://doi.org/10.1038/bcj.2015.95
- Finazzi, G., Caruso, V., Marchioli, R., Capnist, G., Chisesi, T., Finelli, C., Gugliotta, L., Landolfi, R., Kutti, J., Gisslinger, H., Marilus, R., Patrono, C., Pogliani, E. M., Randi, M. L., Villegas, A., Tognoni, G., Barbui, T., & ECLAP Investigators (2005). Acute leukemia in polycythemia vera: an analysis of 1638 patients enrolled in a prospective observational study. Blood, 105(7), 2664–2670. https://doi.org/10.1182/blood-2004-09-3426
- Gisslinger, H., Klade, C., Georgiev, P., Krochmalczyk, D., Gercheva-Kyuchukova, L., Egyed, M., Rossiev, V., Dulicek, P., Illes, A., Pylypenko, H., Sivcheva, L., Mayer, J., Yablokova, V., Krejcy, K., Grohmann-Izay, B., Hasselbalch, H. C., Kralovics, R., Kiladjian, J. J., & PROUD-PV Study Group (2020). Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study. The Lancet. Haematology, 7(3), e196–e208. https://doi.org/10.1016/S2352-3026(19)30236-4
- Gerds, A. T., Gotlib, J., Ali, H., Bose, P., Dunbar, A., Elshoury, A., George, T. I., Gundabolu, K., Hexner, E., Hobbs, G. S., Jain, T., Jamieson, C., Kaesberg, P. R., Kuykendall, A. T., Madanat, Y., McMahon, B., Mohan, S. R., Nadiminti, K. V., Oh, S., Pardanani, A., … Hochstetler, C. (2022). Myeloproliferative Neoplasms, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN, 20(9), 1033–1062. https://doi.org/10.6004/jnccn.2022.0046
- Kuykendall, A.T., et al. Results from VERIFY, a phase 3, double-blind, placebo (PBO)-controlled study of rusfertide for treatment of polycythemia vera (PV).. J Clin Oncol43, LBA3-LBA3(2025). https://doi.org/10.1200/JCO.2025.43.17_suppl.LBA3
- Hoffman, R., Kremyanskaya, M., Ginzburg, Y., et al. (2024). Rusfertide (PTG-300) treatment in phlebotomy-dependent polycythemia vera patients.. J Clin Oncol40, 7003-7003(2022). https://doi.org/10.1200/JCO.2022.40.16_suppl.7003
- Marchioli, R., Finazzi, G., Specchia, G., Cacciola, R., Cavazzina, R., Cilloni, D., De Stefano, V., Elli, E., Iurlo, A., Latagliata, R., Lunghi, F., Lunghi, M., Marfisi, R. M., Musto, P., Masciulli, A., Musolino, C., Cascavilla, N., Quarta, G., Randi, M. L., Rapezzi, D., … CYTO-PV Collaborative Group (2013). Cardiovascular events and intensity of treatment in polycythemia vera. The New England journal of medicine, 368(1), 22–33. https://doi.org/10.1056/NEJMoa1208500
- Tefferi, A., Rumi, E., Finazzi, G., Gisslinger, H., Vannucchi, A. M., Rodeghiero, F., Randi, M. L., Vaidya, R., Cazzola, M., Rambaldi, A., Gisslinger, B., Pieri, L., Ruggeri, M., Bertozzi, I., Sulai, N. H., Casetti, I., Carobbio, A., Jeryczynski, G., Larson, D. R., Müllauer, L., … Barbui, T. (2013). Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia, 27(9), 1874–1881. https://doi.org/10.1038/leu.2013.163
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Emanuel, R. M., Dueck, A. C., Geyer, H. L., Kiladjian, J. J., Slot, S., Zweegman, S., te Boekhorst, P. A., Commandeur, S., Schouten, H. C., Sackmann, F., Kerguelen Fuentes, A., Hernández-Maraver, D., Pahl, H. L., Griesshammer, M., Stegelmann, F., Doehner, K., Lehmann, T., Bonatz, K., Reiter, A., Boyer, F., … Mesa, R. A. (2012). Myeloproliferative neoplasm (MPN) symptom assessment form total symptom score: prospective international assessment of an abbreviated symptom burden scoring system among patients with MPNs. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 30(33), 4098–4103. https://doi.org/10.1200/JCO.2012.42.3863
- Grinfeld, J., Nangalia, J., Baxter, E. J., Wedge, D. C., Angelopoulos, N., Cantrill, R., Godfrey, A. L., Papaemmanuil, E., Gundem, G., MacLean, C., Cook, J., O'Neil, L., O'Meara, S., Teague, J. W., Butler, A. P., Massie, C. E., Williams, N., Nice, F. L., Andersen, C. L., Hasselbalch, H. C., … Campbell, P. J. (2018). Classification and Personalized Prognosis in Myeloproliferative Neoplasms. The New England journal of medicine, 379(15), 1416–1430. https://doi.org/10.1056/NEJMoa1716614
- Kiladjian, JJ., Klade, C., Georgiev, P. et al. Long-term outcomes of polycythemia vera patients treated with ropeginterferon Alfa-2b. Leukemia 36, 1408–1411 (2022). https://doi.org/10.1038/s41375-022-01528-x


