Key Takeaways
Disseminated intravascular coagulation is an acquired, life-threatening disorder where systemic clot formation, disordered fibrinolysis, and blood vessel injury happen at once, leading to both microthrombi and bleeding [1].
- Causes ▾:Disseminated intravascular coagulation is always secondary to another condition. The most common triggers are sepsis, major trauma, certain cancers (especially acute promyelocytic leukemia), and obstetric emergencies [2,7].
- Investigations & Diagnosis ▾: The classic lab pattern is low platelets, prolonged PT and aPTT, low fibrinogen, raised D-dimer, and schistocytes on the blood film. Diagnosis combines the clinical context with a scoring tool such as the ISTH overt-DIC score (≥5 points) or the Sepsis-Induced Coagulopathy (SIC) score, which detects coagulopathy earlier [2,6].
- Treatment and management ▾: Treatment is built around fixing the underlying cause. Bleeding patients receive platelets, fresh frozen plasma, and cryoprecipitate; patients with predominant clotting may receive heparin [3,5].
*Click ▾ for more information
What is disseminated intravascular coagulation?
Disseminated intravascular coagulation (DIC) is a condition in which the clotting system loses its normal localization. Instead of clotting only at sites of injury, thrombin is generated throughout the bloodstream. Tiny clots form in small vessels while platelets and clotting proteins are used up faster than the body can replace them. Bleeding and clotting occur at the same time.
The 2025 ISTH definition captures this clearly: an acquired, life-threatening disorder marked by systemic coagulation activation, disordered fibrinolysis, and endothelial injury that produces microthrombosis, with progression from an early, often silent phase to an advanced phase with bleeding or organ dysfunction [1].
A point worth fixing in your mind from the start: DIC is never a primary disease. It is a complication. Treating DIC means treating whatever set it off.
What causes DIC?
The triggers fall into a small number of mechanism-based groups. They all converge on one thing: large-scale exposure of tissue factor to blood, or massive endothelial activation, which kicks off systemic thrombin generation [2,4].
Severe infection (especially sepsis). Bacterial endotoxins and inflammatory cytokines drive widespread tissue factor expression on monocytes and endothelium. Sepsis is the single most common cause [2].
Major trauma, burns, and surgery. Damaged tissue spills tissue factor directly into circulation.
Malignancy. Acute promyelocytic leukemia (APL) and metastatic adenocarcinomas of the lung, pancreas, prostate, and stomach release procoagulant material into blood.
Obstetric emergencies. Placental abruption, amniotic fluid embolism, retained products of conception, severe preeclampsia, HELLP syndrome, and septic abortion all push thromboplastin-rich material into the maternal circulation.
Vascular disorders. Aortic aneurysms, giant hemangiomas, and cardiopulmonary bypass cause local clot formation that overflows systemically.
Other. Severe liver failure, pancreatitis, heat stroke, hypothermia, snake envenomation, and incompatible transfusion reactions can all trigger DIC.
How DIC develops
The pathophysiology is best understood as loss of localization of clotting, amplified by inflammation.
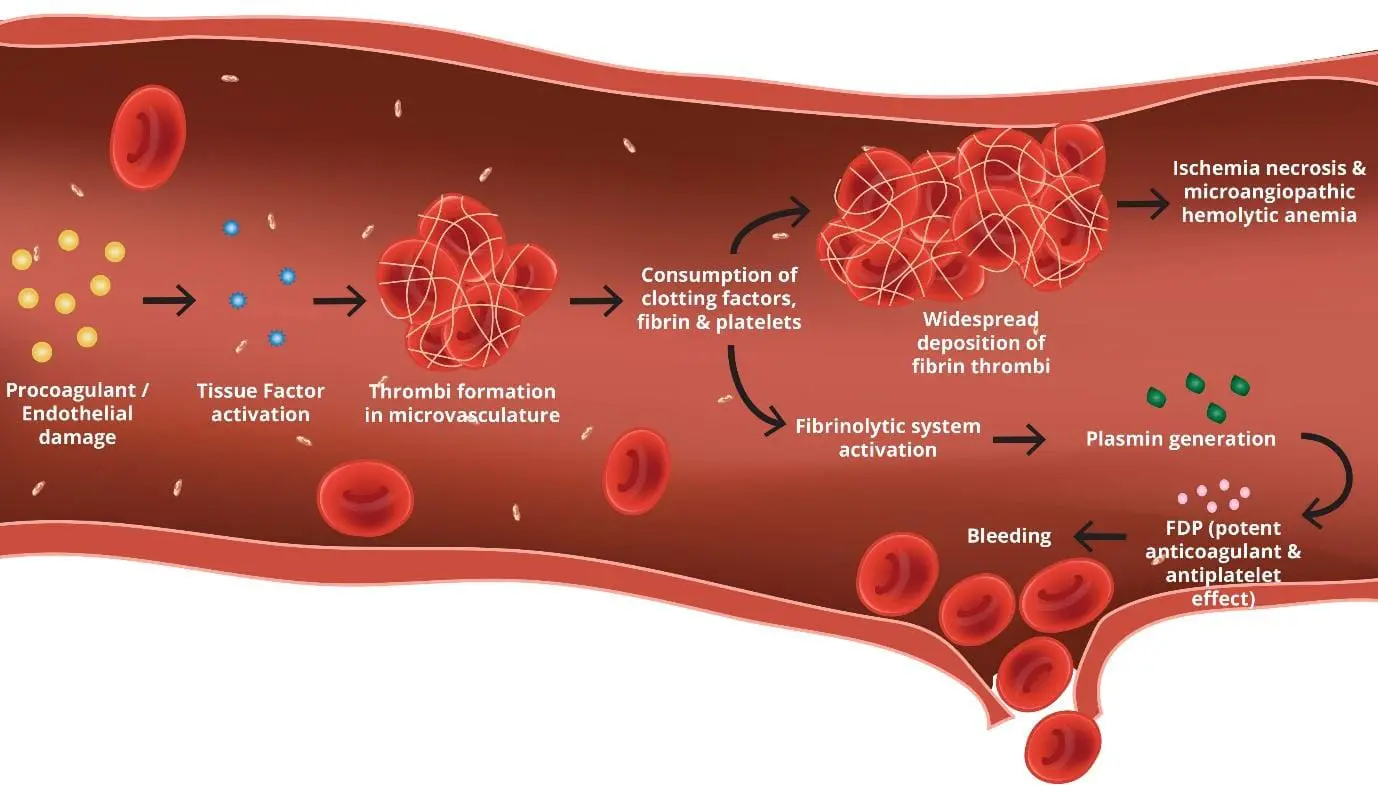
A trigger exposes large amounts of tissue factor to blood. This produces a thrombin burst across the vasculature. Thrombin converts fibrinogen into fibrin, and fibrin meshes form in small vessels (microthrombi). At the same time, the body's natural anticoagulants — antithrombin, protein C, and tissue factor pathway inhibitor — are consumed or down-regulated. Their depletion removes the brakes on clotting [4].
Fibrinolysis is activated in response, but in sepsis it is paradoxically suppressed by high levels of plasminogen activator inhibitor-1 (PAI-1), which traps clots in place and worsens organ injury. In other settings, such as APL or trauma, fibrinolysis runs unchecked and accelerates bleeding [3,4].
This intertwined process is now called thromboinflammation. Activated leukocytes release neutrophil extracellular traps (NETs) and damage-associated molecular patterns (DAMPs), platelets aggregate, and the endothelium loses its anticoagulant surface. Coagulation and inflammation amplify each other [2].
The end result is a paradox: the patient is bleeding because their blood is clotting too much. Platelets and clotting factors are exhausted by the systemic clotting, and there is nothing left to stop hemorrhage at sites that need it.
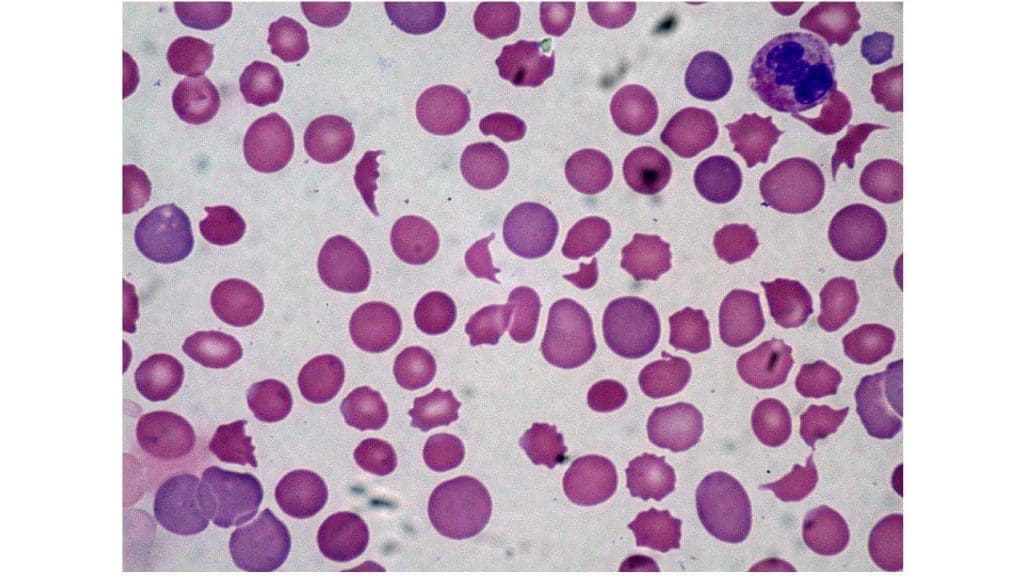
Microangiopathy hemolytic anemia in DIC
As red blood cells squeeze past fibrin strands in small vessels, they get sheared into fragments called schistocytes. This is a consequence of the clotting, not a cause. The presence of schistocytes on the blood film is a clue to microangiopathy and supports the diagnosis. However, it is important to note that schistocytes are only observed in 10% to 20% of DIC cases; their absence does not rule out the diagnosis [9].
Thrombotic and hemorrhagic phenotypes
The traditional split between acute and chronic DIC remains useful, but the 2025 ISTH update emphasizes a more clinically actionable framework: thrombotic versus hemorrhagic phenotype [1,6].
Thrombotic phenotype is dominated by microvascular clotting and organ dysfunction. This is the picture in sepsis-associated DIC, where suppressed fibrinolysis traps fibrin in kidneys, lungs, and skin. Heparin or other anticoagulant strategies may be considered.
Hemorrhagic phenotype is dominated by bleeding from coagulation factor consumption and excessive fibrinolysis. APL, severe trauma, and obstetric DIC are typical examples. Blood product replacement is the priority and heparin is generally avoided.
Many patients shift between phenotypes during their illness, which is why repeat testing matters.
Clinical features of DIC

The clinical picture has two layers. The first is the underlying illness — fever, hypotension, and tachycardia in sepsis, for example. The second is DIC itself. Keep them mentally separate.
Bleeding. Oozing from venipuncture or surgical sites, gum bleeding, epistaxis, petechiae (pinpoint skin bleeds), ecchymoses, hematuria, or major hemorrhage from any site.
Thrombosis. Skin necrosis, digital ischemia (purpura fulminans in severe sepsis), deep vein thrombosis, pulmonary embolism, stroke, or acute kidney injury from microthrombi.
Organ dysfunction. Reflects the combined effect of microthrombi and tissue hypoperfusion: oliguria, confusion, respiratory failure.
A bleeding patient with simultaneous skin or digital ischemia in the setting of sepsis or major trauma should always raise suspicion for disseminated intravascular coagulation.
Laboratory investigations
| Test | Expected Finding in DIC |
|---|---|
| Platelet count | Decreased (<100 × 10⁹/L, often <50) |
| Prothrombin time (PT) | Prolonged |
| Activated partial thromboplastin time (aPTT) | Prolonged |
| Fibrinogen | Decreased (<1.5 g/L; <1 g/L in severe disease) |
| D-dimer / fibrin degradation products | Elevated |
| Peripheral blood film | Schistocytes, thrombocytopenia |
| Antithrombin activity | Decreased |
Trends matter more than single values. A falling platelet count and a falling fibrinogen level over hours are more meaningful than one snapshot. Order serial coagulation studies in patients at risk [3,5].
In modern critical care, major trauma, and obstetrics, viscoelastic tests such as Thromboelastography (TEG) or Rotational Thromboelastometry (ROTEM) are increasingly utilized. These tests provide real-time, functional visualization of clot formation and fibrinolysis, allowing for more rapid and highly targeted blood product transfusions compared to standard laboratory assays [10].
Other tests are guided by the suspected trigger: blood cultures and lactate for sepsis, fibrinogen and PML-RARA testing if APL is suspected, imaging for trauma.
Scoring systems
Scoring tools turn the lab pattern into a structured probability estimate.
ISTH overt-DIC score uses platelet count, PT prolongation, fibrinogen, and D-dimer (or FDP). A score of ≥5 in a patient with a known DIC-precipitating condition supports the diagnosis [5]. The updated 2025 framework formally structures the pathway from early-phase to late-phase DIC. Early-phase scoring relies heavily on platelet counts, PT-INR, and organ dysfunction (e.g., SOFA score), whereas late-phase overt DIC scoring heavily weighs fibrinogen depletion and massive D-dimer elevations [1].
Sepsis-Induced Coagulopathy (SIC) score uses platelet count, INR, and SOFA score. It was designed to detect early coagulopathy in septic patients before they meet overt-DIC criteria, opening a window for earlier intervention [2,6].
Japanese Association for Acute Medicine (JAAM) DIC score is more sensitive for early DIC and is used widely in Japan; it includes parameters reflecting organ damage [6].
Sequential Organ Failure Assessment (SOFA) score is not a DIC tool but quantifies overall organ dysfunction and complements DIC scores in critical care.
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Thrombotic thrombocytopenic purpura (TTP) | ADAMTS13 activity <10%; microangiopathic haemolytic anaemia (MAHA) + thrombocytopaenia; thrombosis; coagulation studies usually normal; schistocytes on film |
| Hemolytic uremic syndrome (HUS) | Diarrhea-associated; predominant kidney injury; normal coagulation |
| Severe liver disease | Decreased synthesis (not consumption) of factors; normal or only mildly raised D-dimer |
| Heparin-induced thrombocytopenia (HIT) | Heparin exposure; normal fibrinogen; positive HIT antibodies |
| Massive transfusion / dilutional coagulopathy | History of large-volume transfusion; coagulopathy from dilution rather than activation |
| Vitamin K deficiency / warfarin effect | Prolonged PT > aPTT; normal platelets, fibrinogen, and D-dimer; corrects with vitamin K |
How is DIC treated?
Treatment is built on three pillars [3,5,7].
1. Treat the underlying cause
This is the only intervention that resolves DIC. Antibiotics and source control for sepsis. Delivery and uterine evacuation for obstetric DIC. All-trans retinoic acid (ATRA) plus arsenic trioxide for APL. Surgical control for trauma. Without addressing the trigger, supportive measures only buy time.
2. Replace what is being consumed (for bleeding patients)
Use blood products based on bleeding or invasive procedures, not on lab numbers alone [5].
- Platelets if count <50 × 10⁹/L with active bleeding, or <20 × 10⁹/L in non-bleeding high-risk patients.
- Fresh frozen plasma if PT or aPTT is >1.5× normal in bleeding patients or before procedures.
- Fibrinogen concentrate or cryoprecipitate if fibrinogen is <1.5 g/L in bleeding patients (some guidelines use <1 g/L). Modern clinical guidelines increasingly favor fibrinogen concentrate over cryoprecipitate because it carries a lower risk of pathogen transmission, does not require thawing, and allows for precise, low-volume dosing in emergencies [11].
Prophylactic transfusion in stable, non-bleeding patients is generally not recommended [5,7].
3. Anticoagulation (for thrombosis-predominant patients)
Therapeutic-dose heparin can be considered in DIC where thrombosis dominates — purpura fulminans, large-vessel venous or arterial thromboembolism. Continuous-infusion unfractionated heparin is often preferred when bleeding risk is also high, because of its short half-life and reversibility with protamine. Heparin is avoided in patients with active major bleeding, recent intracranial hemorrhage, or platelet counts that cannot be supported. It is crucial to distinguish therapeutic anticoagulation from standard prophylaxis; prophylactic-dose low molecular weight heparin (LMWH) remains the standard of care for preventing deep vein thrombosis in critically ill, non-bleeding patients, even in the presence of moderate thrombocytopenia [3,5].
For sepsis-associated DIC, recombinant thrombomodulin and antithrombin concentrate have been studied extensively, mainly in Japan. Evidence remains debated, and these agents are not part of standard care in most countries outside Japan [2]. Importantly, recombinant activated protein C (drotrecogin alfa) was withdrawn worldwide in 2011 after the PROWESS-SHOCK trial and is no longer used.
Antifibrinolytics such as tranexamic acid are generally avoided in DIC because they may worsen microthrombosis. Exceptions include APL with severe hyperfibrinolytic bleeding and selected obstetric DIC.
Supportive care
Fluid resuscitation, vasopressors, mechanical ventilation, and renal replacement therapy as needed. Nutritional support and early rehabilitation matter for recovery.
Prognosis
Outcomes depend almost entirely on the underlying cause and how quickly it is reversed. Sepsis-associated DIC with multi-organ failure carries the highest mortality. APL-associated DIC, once almost universally fatal, now has excellent outcomes with prompt ATRA-based therapy. Obstetric DIC, when the trigger is removed early, often resolves rapidly.
Frequently Asked Questions (FAQs)
How serious is DIC?
DIC is a medical emergency. Mortality varies widely depending on the trigger — from under 10% in well-managed obstetric cases to over 50% in septic shock with multi-organ failure. Early recognition and treatment of the underlying cause are the most important factors in survival.
What are the three most common causes of DIC?
Sepsis is by far the most common, especially gram-negative and meningococcal infection. Major trauma and burns are second. Cancer (particularly acute promyelocytic leukemia and metastatic adenocarcinomas) is third. Obstetric emergencies are also important and are often listed alongside these three.
What happens if DIC is left untreated?
Untreated DIC progresses through worsening microvascular thrombosis, multi-organ failure (kidneys, lungs, liver, brain), and uncontrolled bleeding. The combination is usually fatal. Treatment cannot be deferred while the underlying cause is investigated; both must be tackled in parallel.
Can DIC be prevented?
Often it cannot, because the triggers (severe infection, major trauma) are themselves unpredictable. However, prompt antibiotic therapy in sepsis, careful management of high-risk pregnancies, immediate ATRA in suspected APL, and avoidance of incompatible transfusions all reduce the chance of DIC developing.
How is DIC different from a "normal" blood clot like deep vein thrombosis?
A deep vein thrombosis is a single, localized clot in a large vein. DIC is widespread tiny-vessel clotting throughout the body, with simultaneous bleeding, driven by an underlying systemic illness. The mechanism, treatment, and prognosis are very different.
What should caregivers expect when a loved one is treated for DIC?
Patients are usually managed in a critical care unit. Expect frequent blood draws, multiple intravenous lines, transfusions, and treatments aimed at the underlying cause (antibiotics, surgery, chemotherapy, or delivery if pregnant). The clinical picture can change quickly, so the medical team often updates families daily. Recovery, when it happens, is gradual; even after DIC resolves, organ function may take weeks to return to baseline.
Glossary of Related Medical Terms
- Coagulation cascade — the chain of plasma protein reactions that converts soluble fibrinogen into solid fibrin to form a clot.
- Cryoprecipitate — a blood product rich in fibrinogen, factor VIII, and von Willebrand factor, used to replace fibrinogen.
- D-dimer — a small protein fragment released when fibrin clots are broken down; a high level signals active clot formation and breakdown.
- DAMPs (damage-associated molecular patterns) — molecules released by injured cells that trigger inflammation and coagulation.
- Endothelium — the thin cell layer lining the inside of blood vessels; normally keeps blood from clotting on contact.
- Fibrinolysis — the body's process for dissolving fibrin clots, mainly through the enzyme plasmin.
- Fresh frozen plasma (FFP) — donor plasma frozen soon after collection; replaces multiple clotting factors at once.
- Microangiopathic hemolytic anemia (MAHA) — anemia caused by red blood cells being shredded as they pass through fibrin strands in tiny blood vessels.
- Microthrombi — very small blood clots that block tiny vessels.
- Petechiae — pinpoint red or purple spots on the skin caused by small bleeds under the surface.
- Schistocytes — fragmented red blood cells, often helmet-shaped, seen on a blood film when cells are mechanically damaged.
- Sepsis-induced coagulopathy (SIC) — early-stage clotting dysregulation in sepsis that can progress to overt DIC if untreated.
- Thrombin — the central enzyme that converts fibrinogen to fibrin.
- Thromboinflammation — the linked activation of clotting and inflammation that drives sepsis-related DIC.
- Thrombocytopenia — a low platelet count, generally below 150 × 10⁹/L.
- Tissue factor — a protein on cells outside blood vessels that triggers clotting when exposed to blood.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Iba, T., Levy, J. H., Maier, C. L., Helms, J., Umemura, Y., Moore, H., Othman, M., Thachil, J., Connors, J. M., Levi, M., & Scarlatescu, E. (2025). Updated definition and scoring of disseminated intravascular coagulation in 2025: communication from the ISTH SSC Subcommittee on Disseminated Intravascular Coagulation. Journal of thrombosis and haemostasis : JTH, 23(7), 2356–2362. https://doi.org/10.1016/j.jtha.2025.03.038
- Iba, T., Helms, J., Connors, J. M., & Levy, J. H. (2023). The pathophysiology, diagnosis, and management of sepsis-associated disseminated intravascular coagulation. Journal of intensive care, 11(1), 24. https://doi.org/10.1186/s40560-023-00672-5
- Levi, M., & Scully, M. (2018). How I treat disseminated intravascular coagulation. Blood, 131(8), 845–854. https://doi.org/10.1182/blood-2017-10-804096
- Unar, A., Bertolino, L., Patauner, F., Gallo, R., & Durante-Mangoni, E. (2023). Pathophysiology of Disseminated Intravascular Coagulation in Sepsis: A Clinically Focused Overview. Cells, 12(17), 2120. https://doi.org/10.3390/cells12172120
- Wada, H., Thachil, J., Di Nisio, M., Mathew, P., Kurosawa, S., Gando, S., Kim, H. K., Nielsen, J. D., Dempfle, C. E., Levi, M., Toh, C. H., & The Scientific Standardization Committee on DIC of the International Society on Thrombosis Haemostasis (2013). Guidance for diagnosis and treatment of DIC from harmonization of the recommendations from three guidelines. Journal of thrombosis and haemostasis : JTH, 10.1111/jth.12155. Advance online publication. https://doi.org/10.1111/jth.12155
- Iba, T., Di Nisio, M., Thachil, J., Wada, H., Asakura, H., Sato, K., & Saitoh, D. (2018). A Proposal of the Modification of Japanese Society on Thrombosis and Hemostasis (JSTH) Disseminated Intravascular Coagulation (DIC) Diagnostic Criteria for Sepsis-Associated DIC. Clinical and applied thrombosis/hemostasis : official journal of the International Academy of Clinical and Applied Thrombosis/Hemostasis, 24(3), 439–445. https://doi.org/10.1177/1076029617720069
- Costello RA, Leslie SW, Nehring SM. Disseminated Intravascular Coagulation. [Updated 2024 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441834/
- Squizzato, A., Gallo, A., Levi, M., Iba, T., Levy, J. H., Erez, O., Ten Cate, H., Solh, Z., Gando, S., Vicente, V., & Di Nisio, M. (2020). Underlying disorders of disseminated intravascular coagulation: Communication from the ISTH SSC Subcommittees on Disseminated Intravascular Coagulation and Perioperative and Critical Care Thrombosis and Hemostasis. Journal of thrombosis and haemostasis : JTH, 18(9), 2400–2407. https://doi.org/10.1111/jth.14946
- Boral, B. M., Williams, D. J., & Boral, L. I. (2016). Disseminated Intravascular Coagulation. American journal of clinical pathology, 146(6), 670–680. https://doi.org/10.1093/ajcp/aqw195
- Walsh, M., Thomas, S. G., Howard, J. C., Evans, E., Guyer, K., Medvecz, A., Swearingen, A., Navari, R. M., Ploplis, V., & Castellino, F. J. (2011). Blood component therapy in trauma guided with the utilization of the perfusionist and thromboelastography. The journal of extra-corporeal technology, 43(3), 162–167.
- Spahn, D. R., Bouillon, B., Cerny, V., Duranteau, J., Filipescu, D., Hunt, B. J., Komadina, R., Maegele, M., Nardi, G., Riddez, L., Samama, C. M., Vincent, J. L., & Rossaint, R. (2019). The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Critical care (London, England), 23(1), 98. https://doi.org/10.1186/s13054-019-2347-3