Key Takeaways
The activated partial thromboplastin time also known as aPTT is a blood test that measures how long plasma takes to clot through the intrinsic and common pathways of the coagulation cascade [1].
- The aPTT is the standard screening test for hemophilia A and B, and it is widely used to monitor unfractionated heparin therapy, although anti-Xa assays are increasingly preferred [5,6].
- A prolonged aPTT can come from factor deficiencies (such as hemophilia), inhibitors (such as lupus anticoagulant), drugs (heparin, direct thrombin inhibitors), liver disease, DIC, or pre-analytical errors [1,2].
- A mixing study with normal pooled plasma separates factor deficiency from inhibitors. If the prolongation corrects, suspect deficiency. If it does not correct, suspect an inhibitor [1,2].
Introduction
The activated partial thromboplastin time (aPTT) blood test measures how well a patient's blood is clotting through one specific arm of the coagulation system.
The aPTT shows up in three big clinical situations: monitoring patients on unfractionated heparin, screening for hemophilia and other intrinsic pathway deficiencies, and working up unexplained bleeding or pre-operative bleeding risk [1]. Understanding what the test measures, and what it does not, is the difference between treating the result and treating the patient.
This guide walks you through the principle, the bench protocol, the interpretation logic, and the pitfalls. By the end, you should be able to read an aPTT result and ask the right next question.
Principle of aPTT Assay
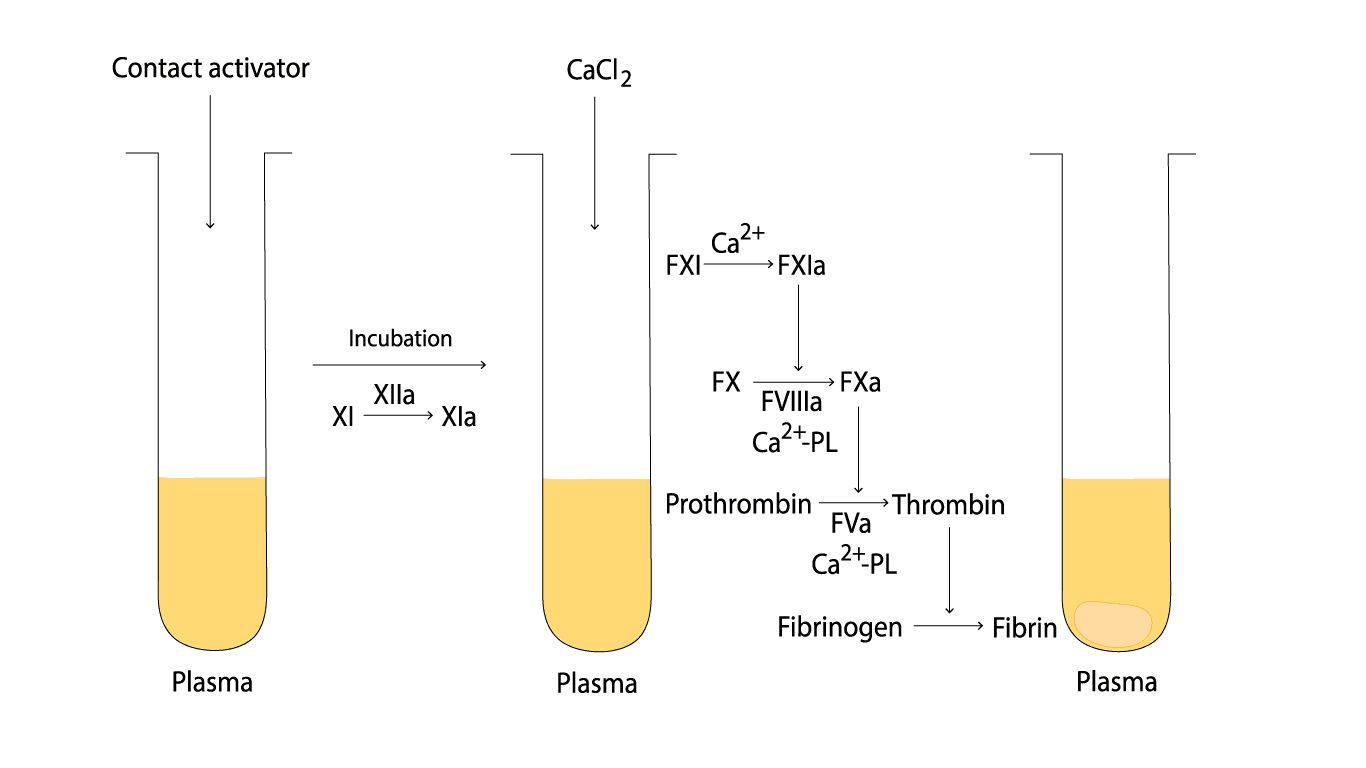
The aPTT measures plasma clotting time after the contact factors of the intrinsic pathway are deliberately switched on. No tissue thromboplastin is added, which is the key feature that separates this test from prothrombin time (PT).
Here is the sequence inside the test tube. Patient plasma is incubated with a contact activator (kaolin, silica, or ellagic acid) and a phospholipid. The activator triggers Factor XII, which converts to Factor XIIa. Factor XIIa then activates Factor XI to Factor XIa. During this incubation step, calcium is deliberately absent to stop clotting from running ahead of the timer.
Once calcium chloride is added, Factor XIa activates Factor IX, and the cascade proceeds through Factor VIII, the common pathway (Factors X, V, II, I), and finally to a visible fibrin clot. The phospholipid in the reagent stands in for the platelet surface, which is why the test runs on platelet-poor plasma (PPP), plasma that has had its platelets removed by centrifugation [1].
The aPTT is therefore sensitive to the contact factors (XII, XI, prekallikrein, HMWK), Factors VIII and IX, and the common pathway factors (X, V, II, I). It also flags circulating inhibitors and most heparin in the sample.
Materials
- #Platelet poor plasma (PPP) of patient and control. PPP is prepared by centrifuging the peripheral blood at 2000 g for 15 minutes at room temperature.
- *Activator-phospholipid solution
- *0.025 mol/L calcium chloride (CaCl2)
- *Glass tubes 5 ml
- *Water bath
- Stopwatch and timer
- Pipettes (100 - 200 ul) and pipette tips
*These items must be pre-warmed to 37°C.
#PPP must be kept at room temperature. Cold storage can cold-activate Factor VII and cause inaccurate timing. Citrated samples should ideally be tested within 4 hours of collection [3].
Protocol
The addition of activator and phospholipid to the platelet-poor plasma initiates the intrinsic coagulation pathway. This pathway involves a series of enzymatic reactions, leading to the formation of thrombin, the enzyme responsible for converting fibrinogen to fibrin, the insoluble clot.
Run every step inside the water bath at 37 °C, except the brief moments when you lift the tube to look for clot formation.
- Pipette 0.1 mL of patient plasma and 0.1 mL of control plasma into separate, labeled test tubes. Set the timer for 3 minutes.
- Add 0.2 mL of activator-phospholipid solution to each tube and start the timer immediately.
- Incubate at 37 °C for 3 minutes with occasional gentle agitation.
- Have the stopwatch ready. Add 0.1 mL of CaCl₂ and start the stopwatch the instant the calcium hits the plasma.
- Tilt the tube to about 45° and agitate gently to mix.
- Lift the tube briefly and intermittently to watch for the first wisp of fibrin.
- Stop the stopwatch the moment a clot appears, and record the time.
- Run patient and control plasma in duplicate. Report the average.
Reagent kits vary slightly between manufacturers. Always read the package insert for your specific assay before deviating from this generic protocol.
Interpretation
The reference range for the activated partial thromboplastin time is typically 26–40 seconds, though every lab must establish its own range based on its reagent and analyzer. A result outside that range needs context, not panic. The clinical question is always: why is this number where it is?
Common Causes of a Prolonged aPTT
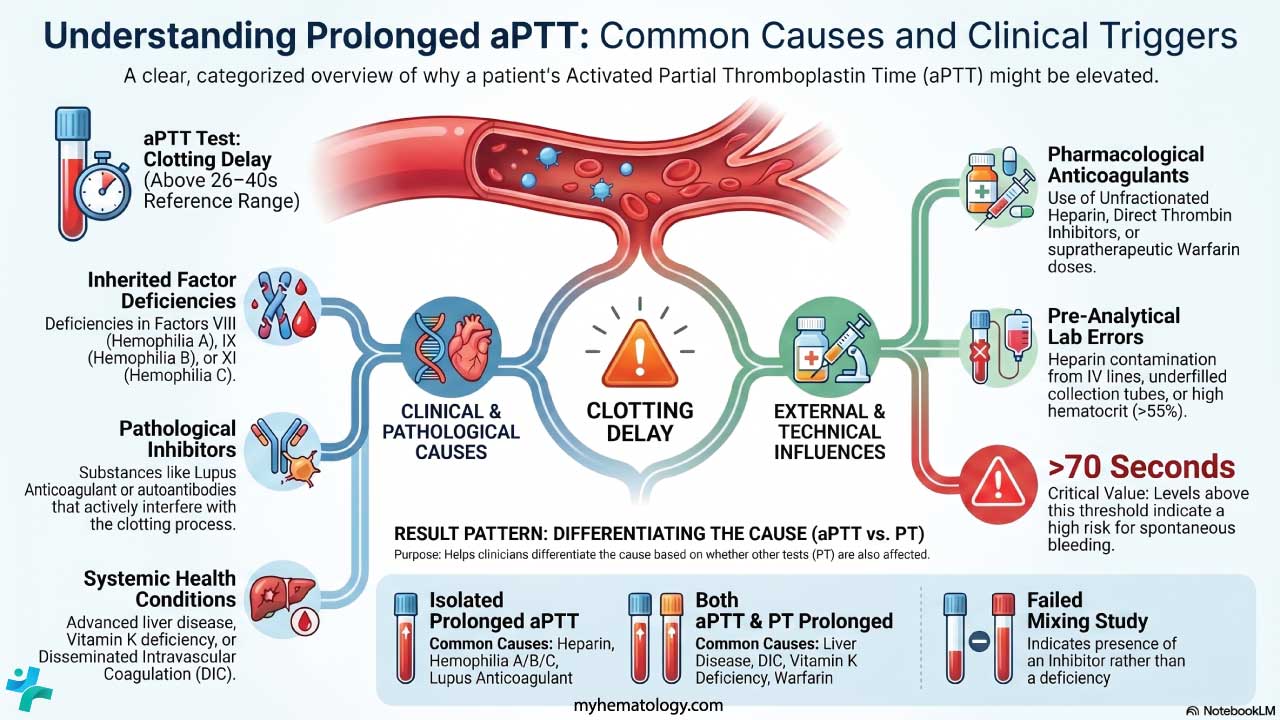
A prolonged aPTT means the intrinsic and/or common pathway is taking longer than expected to generate a clot. The differential splits into a few clean categories.
Inherited factor deficiencies (intrinsic pathway)
- Hemophilia A: Factor VIII deficiency.
- Hemophilia B (Christmas disease): Factor IX deficiency.
- Hemophilia C: Factor XI deficiency, most common in Ashkenazi Jewish populations.
- Von Willebrand disease (vWD): Severe vWF deficiency lowers Factor VIII secondarily, because vWF is its carrier protein, which can prolong the aPTT.
- Contact factor deficiencies: Factor XII, prekallikrein, or high molecular weight kininogen (HMWK). These prolong the aPTT in the lab but do not cause clinical bleeding.
Modern hemophilia management has moved well beyond factor concentrate alone. Emicizumab, a bispecific antibody that mimics Factor VIII, has changed prophylaxis for Hemophilia A, and gene therapies are now approved for both Hemophilia A and B.
CRITICAL WARNING:
Because emicizumab acts as an activated Factor VIII, it exerts a strong procoagulant effect in the test tube, which falsely shortens or completely normalizes the aPTT [8]. You cannot use a standard aPTT or a one-stage aPTT-based single-factor assay to monitor hemostasis or check for inhibitors in patients on emicizumab. Instead, clinical laboratories must use a specific chromogenic Factor VIII assay utilizing bovine reagents, which are unaffected by the drug [10].
Acquired inhibitors
- Lupus anticoagulant (LA): An antiphospholipid antibody. It produces the classic biological paradox: it prolongs the aPTT in the test tube by interfering with the phospholipid reagent, yet in the patient it is associated with thrombosis, not bleeding. The lab finding and the clinical risk point in opposite directions [2]. Furthermore, the sensitivity of the aPTT to LA is highly dependent on the reagent's activator and phospholipid composition. Reagents using silica are traditionally recommended for high sensitivity, though low-phospholipid ellagic acid reagents are also highly effective [9].
- Specific factor inhibitors: Autoantibodies, usually IgG, against a specific factor. The most clinically important is the acquired Factor VIII inhibitor (acquired hemophilia A), which can cause life-threatening bleeding and does not correct on a mixing study [4].
Drug effects
- Unfractionated heparin (UFH): The most common cause of a prolonged aPTT in hospitalized patients. Heparin enhances antithrombin, which inhibits thrombin (Factor IIa) and Factor Xa.
- Direct thrombin inhibitors: Dabigatran, argatroban, bivalirudin.
- DOACs: Direct Factor Xa inhibitors (rivaroxaban, apixaban) and direct thrombin inhibitors (dabigatran) affect the assay differently. Dabigatran will generally prolong the aPTT. Conversely, the aPTT is dangerously insensitive to apixaban and rivaroxaban; it often remains completely normal even at therapeutic or supratherapeutic doses [11]. The aPTT must not be used to monitor DOAC therapy; specific anti-Xa or dilute thrombin time assays are required.
Multiple factor deficiencies (both aPTT and PT prolonged). When both screening tests are abnormal, think common pathway or a global problem.
- Liver disease: Reduced synthesis of nearly all clotting factors, with Factor VIII a notable exception.
- Disseminated intravascular coagulation (DIC): Widespread activation consumes factors and platelets.
- Vitamin K deficiency: Impairs Factors II, VII, IX, and X. Severe deficiency hits both PT and aPTT.
- Supratherapeutic warfarin: Very high doses eventually prolong the aPTT, even though PT is far more sensitive.
Pre-analytical errors (false prolongation). Before chasing a diagnosis, rule out the sample.
- Heparin contamination, typically from a central line flushed with heparin.
- Inadequate fill volume. The 9:1 blood-to-citrate ratio is critical. Samples must be drawn into a light blue top tube containing exactly 3.2% (0.109 mol/L) sodium citrate [3]. An underfilled tube has excess citrate, which binds the calcium in the reagent and falsely prolongs the result. To prevent tissue factor activation or cross-contamination, ensure the coagulation tube is drawn after non-additive tubes but before serum or heparin tubes.
- Polycythemia (hematocrit > 55%). Less plasma per tube means a higher relative citrate concentration, again over-anticoagulating the sample. For these patients, the citrate volume must be adjusted using the standard clinical laboratory formula: C=1.85×10−3×(100−Hct)×Vblood where C is the volume of citrate to leave in the tube, Hct is the patient's hematocrit, and V is the volume of blood to be collected) [7].
- Hemolysis, lipemia, or icterus, which can interfere with optical clot detection.
- Delayed processing, especially samples sitting beyond 4 hours [3].
Isolated Prolonged aPTT
Intrinsic pathwayIsolated Prolonged PT
Extrinsic pathwayBoth Prolonged
Multiple pathwaysMixing Study
Once an isolated prolonged aPTT shows up and pre-analytical errors have been excluded, the next clinical question is sharp and binary: is this a factor deficiency or an inhibitor? The mixing study is the gatekeeper that answers it [1,2].
How it works. Mix patient plasma 1:1 with normal pooled plasma (NPP), which contains roughly 100% of every clotting factor. Repeat the aPTT on the mixture.
How to read it.
- Correction: The aPTT returns to the normal range. The 50% factor concentration supplied by the NPP was enough to fix the deficit, so the patient has a factor deficiency (e.g., hemophilia A or B).
- Failure to correct: The aPTT stays prolonged. Something in the patient's plasma is neutralizing the factors from the NPP. Suspect an inhibitor such as lupus anticoagulant or an acquired Factor VIII antibody.
The incubated mixing study. Some inhibitors, particularly Factor VIII autoantibodies, are time- and temperature-dependent. They may not show their full effect immediately. The 2024 ICSH recommendations suggest performing both an immediate and an incubated (1–2 hours at 37 °C) mixing study when an inhibitor is suspected [1]. A pattern that corrects immediately but prolongs after incubation is highly suggestive of an acquired Factor VIII inhibitor.
What comes next. If a Factor VIII inhibitor is suspected, the Bethesda assay quantifies the inhibitor titer in Bethesda units, which guides treatment decisions [4]. If lupus anticoagulant is suspected, dedicated LA testing (DRVVT and confirmatory mixes) is performed.
For a deeper dive into protocols, incubation timing, and inhibitor patterns, see the full guide on Manual aPTT Mixing Studies.
Heparin Monitoring
Traditionally, the therapeutic aPTT target for unfractionated heparin has been 1.5 to 2.5 times the laboratory's mean control value. That target should ideally be calibrated against an anti-Xa range of 0.3–0.7 IU/mL [5,6]. Many centers now run the anti-Xa assay as their primary heparin monitoring tool because it is more reliable in patients with elevated Factor VIII, lupus anticoagulant, or consumptive coagulopathy, all of which can throw off the aPTT [5]. The activated partial thromboplastin time still has a role, but understanding its limitations is part of modern practice.
Common Pitfalls
- A prolonged aPTT does not always mean bleeding risk. Lupus anticoagulant prolongs it in the tube but raises thrombosis risk in the patient.
- Factor XII deficiency prolongs the aPTT but does not cause clinical bleeding. Do not mistake a lab number for a hemorrhagic disorder.
- The PT/INR is for warfarin. The aPTT is for heparin. Mixing these up is one of the most common errors in early clinical training.
- Sample quality first, diagnosis second. Always rule out underfill, heparin contamination, and delayed processing before working up a "mystery" prolonged aPTT.
- Children, especially neonates, have physiologically longer aPTT values than adults. Use age-appropriate reference ranges.
Frequently Asked Questions (FAQs)
What is the difference between PT and aPTT?
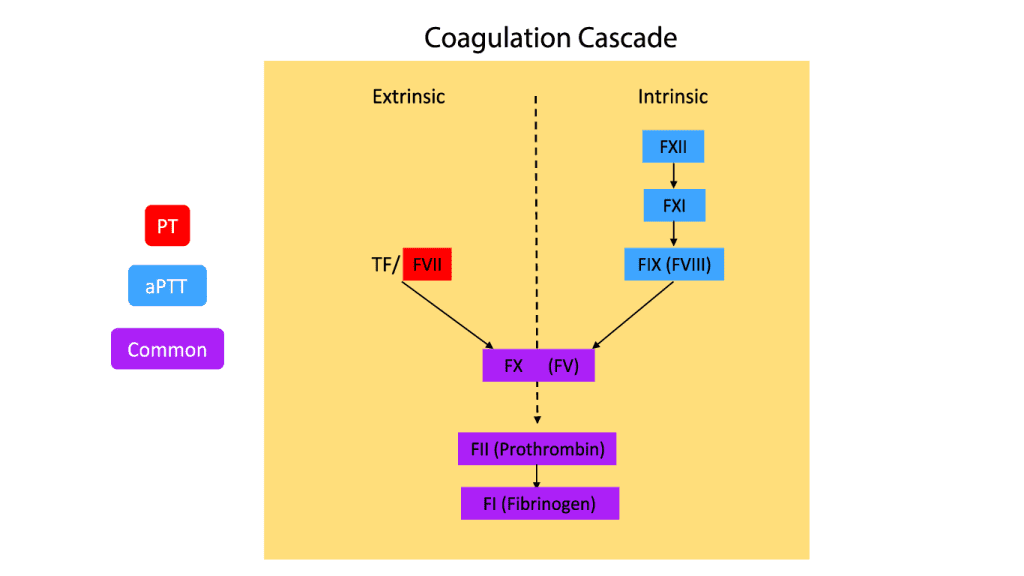
Both tests measure clotting time, but they assess different pathways. The Prothrombin Time (PT) measures the extrinsic and common pathways and is used to monitor warfarin. The activated partial thromboplastin time measures the intrinsic and common pathways and is used to monitor unfractionated heparin and to screen for hemophilia. PT evaluates Factors VII, X, V, II, and I. aPTT evaluates Factors XII, XI, IX, VIII, X, V, II, and I.
What coagulation factors does the aPTT assess?
The activated partial thromboplastin time evaluates Factor XII, Factor XI, Factor IX, and Factor VIII from the intrinsic pathway, plus Factor X, Factor V, Factor II (prothrombin), and Factor I (fibrinogen) from the common pathway. A deficiency or inhibitor against any of these can prolong the result.
What is a critical aPTT level?
A result above 70 seconds is generally treated as a critical value because of the high risk of spontaneous bleeding, although exact cutoffs vary between laboratories. Context matters: a patient on therapeutic heparin will have a deliberately prolonged aPTT, and that number is interpreted differently from the same value in a patient who is not anticoagulated.
Does the aPTT change with age?
Yes. Neonates and young children typically have longer aPTT values than adults because several clotting factors are physiologically lower at birth and mature over the first months to years of life. Adult values are relatively stable. The elderly may show a slight increase, but the change is far less marked than in pediatrics. Always use age-appropriate reference ranges.
Can the aPTT be used to monitor warfarin?
No. Warfarin is monitored using the PT, reported as the International Normalized Ratio (INR). Although very high warfarin doses can eventually prolong the aPTT, PT/INR is much more sensitive to the vitamin K-dependent factors and is the international standard.
Why does the aPTT stay prolonged after a mixing study?
A failure to correct points to an inhibitor rather than a deficiency. The normal pooled plasma supplied 50% of every clotting factor, which is enough to fix a deficiency, but something in the patient's plasma is neutralizing those factors. The most common culprits are lupus anticoagulant and specific factor antibodies, particularly against Factor VIII [2].
What happens if the sample is contaminated with heparin?
Heparin contamination, often from a sample drawn through a central line that was flushed with heparin, dramatically prolongs the aPTT. Laboratories confirm this with a Thrombin Time (TT) or by treating the sample with a heparin-neutralizing agent such as protamine sulfate or a heparinase. If the prolongation disappears, heparin was the cause.
Can the aPTT ever be shortened?
Yes. A shortened aPTT, sometimes below 25 seconds, can occur with elevated Factor VIII (acute phase reactant), in pregnancy, in some malignancies, and in inflammatory states. It can signal a hypercoagulable tendency and a higher risk of venous thromboembolism, although it is not used alone to make that diagnosis.
Why is the aPTT used to screen for hemophilia?
Hemophilia A (Factor VIII deficiency) and Hemophilia B (Factor IX deficiency) both involve intrinsic pathway factors. Because the aPTT specifically measures intrinsic and common pathway function, it captures these deficiencies as a prolonged clotting time. A confirmed prolongation then leads to specific factor assays to identify which factor is missing and how severe the deficiency is.
Glossary of Related Medical Terms
- Intrinsic pathway: The arm of the clotting cascade triggered by contact with damaged vessel surfaces. Involves Factors XII, XI, IX, and VIII.
- Extrinsic pathway: Triggered by tissue injury releasing tissue factor. Involves Factor VII. Measured by PT.
- Common pathway: The shared final stretch involving Factors X, V, II, and I.
- Contact activator: Reagent (silica, kaolin, or ellagic acid) that switches on Factor XII.
- Phospholipid (partial thromboplastin): Lipid surface in the reagent that mimics the platelet membrane.
- Platelet-poor plasma (PPP): Plasma centrifuged to remove platelets.
- Mixing study: A 1:1 mix of patient plasma with normal pooled plasma to separate factor deficiency from inhibitor.
- Lupus anticoagulant: An antiphospholipid antibody that prolongs aPTT in the lab but raises thrombosis risk in the patient.
- Factor inhibitor: An antibody, usually IgG, that neutralizes a specific clotting factor, most commonly Factor VIII.
- Bethesda assay: A test that quantifies the strength of a Factor VIII inhibitor in Bethesda units.
- Anti-Xa assay: A direct measure of heparin or anti-Xa drug activity. Increasingly used to monitor unfractionated heparin instead of the aPTT.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Adcock, D. M., Moore, G. W., Kershaw, G. W., Montalvao, S. A. L., & Gosselin, R. C. (2024). International Council for Standardization in Haematology (ICSH) recommendations for the performance and interpretation of activated partial thromboplastin time and prothrombin time mixing tests. International journal of laboratory hematology, 46(5), 777–788. https://doi.org/10.1111/ijlh.14344
- Favaloro E. J. (2020). Coagulation mixing studies: Utility, algorithmic strategies and limitations for lupus anticoagulant testing or follow up of abnormal coagulation tests. American journal of hematology, 95(1), 117–128. https://doi.org/10.1002/ajh.25669
- Kitchen, S., Adcock, D. M., Dauer, R., Kristoffersen, A. H., Lippi, G., Mackie, I., Marlar, R. A., & Nair, S. (2021). International Council for Standardisation in Haematology (ICSH) recommendations for collection of blood samples for coagulation testing. International journal of laboratory hematology, 43(4), 571–580. https://doi.org/10.1111/ijlh.13584
- Witmer, C., & Young, G. (2013). Factor VIII inhibitors in hemophilia A: rationale and latest evidence. Therapeutic advances in hematology, 4(1), 59–72. https://doi.org/10.1177/2040620712464509
- Vandiver, J. W., & Vondracek, T. G. (2012). Antifactor Xa levels versus activated partial thromboplastin time for monitoring unfractionated heparin. Pharmacotherapy, 32(6), 546–558. https://doi.org/10.1002/j.1875-9114.2011.01049.x
- Garcia, D. A., Baglin, T. P., Weitz, J. I., & Samama, M. M. (2012). Parenteral anticoagulants: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest, 141(2 Suppl), e24S–e43S. https://doi.org/10.1378/chest.11-2291
- Gorio, C., Molinari, A. C., Martini, T., Ferretti, A., Albrici, G., Carracchia, G., Ierardi, A., Leotta, M., Portesi, N., Sacco, M., Strangio, A., Mancuso, M. E., Santoro, R. C., & AICE (Associazione Italiana Centri Emofilia) (2025). Hemostasis Laboratory Diagnostics in Newborns. Journal of clinical medicine, 14(14), 5068. https://doi.org/10.3390/jcm14145068
- Jenkins, P. V., Bowyer, A., Burgess, C., Gray, E., Kitchen, S., Murphy, P., Platton, S., Riddell, A., Chowdary, P., & Lester, W. (2020). Laboratory coagulation tests and emicizumab treatment A United Kingdom Haemophilia Centre Doctors' Organisation guideline. Haemophilia : the official journal of the World Federation of Hemophilia, 26(1), 151–155. https://doi.org/10.1111/hae.13903
- Kumano, O., Ieko, M., Naito, S., Yoshida, M., & Takahashi, N. (2012). APTT reagent with ellagic acid as activator shows adequate lupus anticoagulant sensitivity in comparison to silica-based reagent. Journal of thrombosis and haemostasis : JTH, 10(11), 2338–2343. https://doi.org/10.1111/j.1538-7836.2012.04906.x
- Lee, M. Y., Lee, W. I., Kang, S. Y., Kim, M. H., & Park, Y. S. (2023). Verification and Comparison of Chromogenic Factor VIII Activity Assays in Patients With Hemophilia Treated With and Without Emicizumab. Annals of laboratory medicine, 43(1), 96–99. https://doi.org/10.3343/alm.2023.43.1.96
- Marco-Rico, A. (2024). Laboratory Monitoring of Direct Oral Anticoagulants. In Anticoagulation - An Update. IntechOpen. https://doi.org/10.5772/intechopen.112079