Key Takeaways
An acute hemolytic transfusion reaction (AHTR) is the rapid destruction of transfused red blood cells, occurring during or within 24 hours of a blood transfusion, and it is a medical emergency [1,3].
- Timing ▾: During transfusion or within 24 hours.
- Signs and Symptoms ▾: Classic signs are fever, chills, lower back or flank pain, low blood pressure, dark or red urine (hemoglobinuria), and, in severe cases, shock, disseminated intravascular coagulation, and acute kidney injury [1,3].
- Causes ▾: The most common and most severe cause is ABO incompatibility from clerical error, such as patient misidentification, mislabeled samples, or hanging the wrong unit [1,3,8].
- Treatment and management ▾: The first action when AHTR is suspected is to stop the transfusion immediately, keep the IV line open with normal saline, and verify the patient and unit details [1,7]. Most AHTRs are preventable through two-person bedside checks, two-patient identifiers, and barcode-based electronic identification systems [1,8].
*Click ▾ for more information
What is an Acute Hemolytic Transfusion Reaction (AHTR)?
An acute hemolytic transfusion reaction (AHTR) is a sudden destruction of red blood cells triggered by an antigen-antibody mismatch between donor and recipient. It happens during the transfusion itself or within the next 24 hours [1,3].
In the most common scenario, the recipient already has antibodies (such as anti-A or anti-B) that attack the antigens on the donor's red cells. The opposite can also happen: donor plasma containing anti-A or anti-B can attack the recipient's red cells, which is why ABO-mismatched plasma-rich products such as platelets sometimes trigger AHTR [2].
AHTR is rare, but when it happens it is fast, dramatic, and almost always preventable. Hospitals build many checks into transfusion to prevent it, and that nursing teams watch closely during the first 15 minutes of every unit.
Sign and Symptoms
Symptoms can begin within minutes. Mild reactions may show only fever or chills, while severe reactions progress rapidly to shock and organ failure.
The classic features of a severe AHTR are:
- Fever and chills, often the first sign
- Lower back or flank pain
- Pain or burning at the infusion site
- Hypotension (low blood pressure) and tachycardia (fast heart rate)
- Shortness of breath
- Hemoglobinuria, where the urine looks dark, tea-colored, or red
- Bleeding from IV sites, indicating disseminated intravascular coagulation (DIC)
- Reduced or absent urine output, indicating acute kidney injury
Hives and itching, by contrast, suggest an allergic rather than a hemolytic reaction and should not be confused with AHTR [3,7].
A Special Note on Anesthetized or Unconscious Patients
A patient under general anesthesia or who is unconscious cannot report fever, pain, or shortness of breath. In these patients, AHTR may present only as unexplained hypotension, oozing from the surgical or IV site, or hemoglobinuria in the catheter bag [1,3].
The Three Clinical Phases
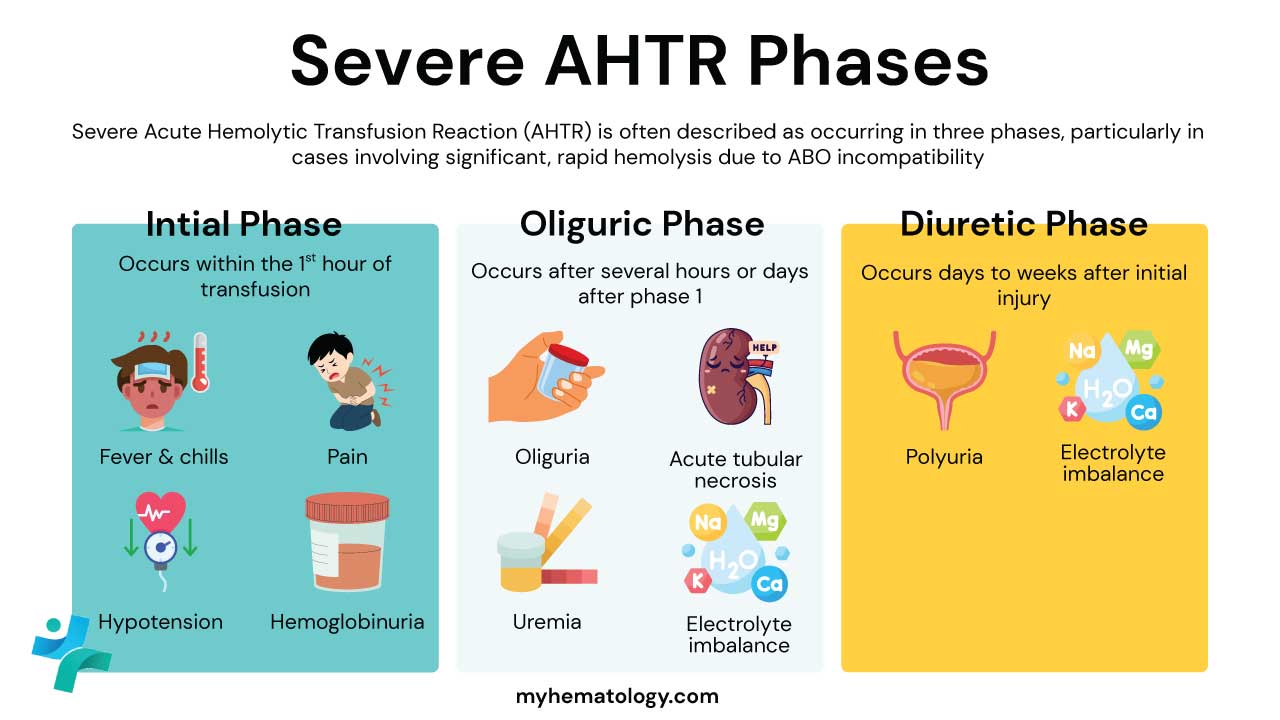
When ABO-incompatible blood is transfused, the reaction often unfolds in three stages that mirror the pattern of acute tubular necrosis:
- Hemolytic shock phase. Fever, chills, severe lower back pain, hypotension, and hemoglobinuria appear first as antibodies destroy donor red cells inside the blood vessels. Large incompatible transfusions can trigger DIC.
- Oliguric phase. Free hemoglobin and shock injure the renal tubules. Urine output falls and electrolyte disturbances such as hyperkalemia can develop.
- Diuretic (recovery) phase. As tubules regenerate, urine output rises sharply. Fluid and electrolyte balance must be watched closely to avoid dehydration and hypokalemia.
How Long Does It Take for an AHTR to Occur?
By definition, AHTR occurs during the transfusion or within 24 hours of completion. Severe ABO-mediated reactions typically begin in the first 5 to 15 minutes [1,3]. This is why the opening minutes of every unit are given slowly under direct observation, and why nursing protocols cluster vital sign checks at the start of a transfusion.
Causes of AHTR

Causes fall into two broad groups: immune-mediated (the majority) and non-immune-mediated (less common but important).
Immune-Mediated Causes
ABO Incompatibility — The Leading Cause
AHTR from ABO incompatibility is almost always the result of clerical or human error, not a laboratory failure [1,3,8]. The usual mistakes are:
- Misidentifying the patient at the bedside.
- Drawing or labeling a blood sample incorrectly, the so-called wrong blood in tube (WBIT) error.
- Hanging the wrong unit on the wrong patient.
The mechanism is fast and aggressive. Anti-A and anti-B antibodies (called isohemagglutinins) are naturally present in people who lack the matching antigen. They are usually IgM and powerfully activate the complement cascade. When incompatible blood enters the recipient, antibodies bind donor red cells, complement punches holes in their membranes, and intravascular hemolysis follows within minutes [1,3].
Non-ABO Alloantibodies
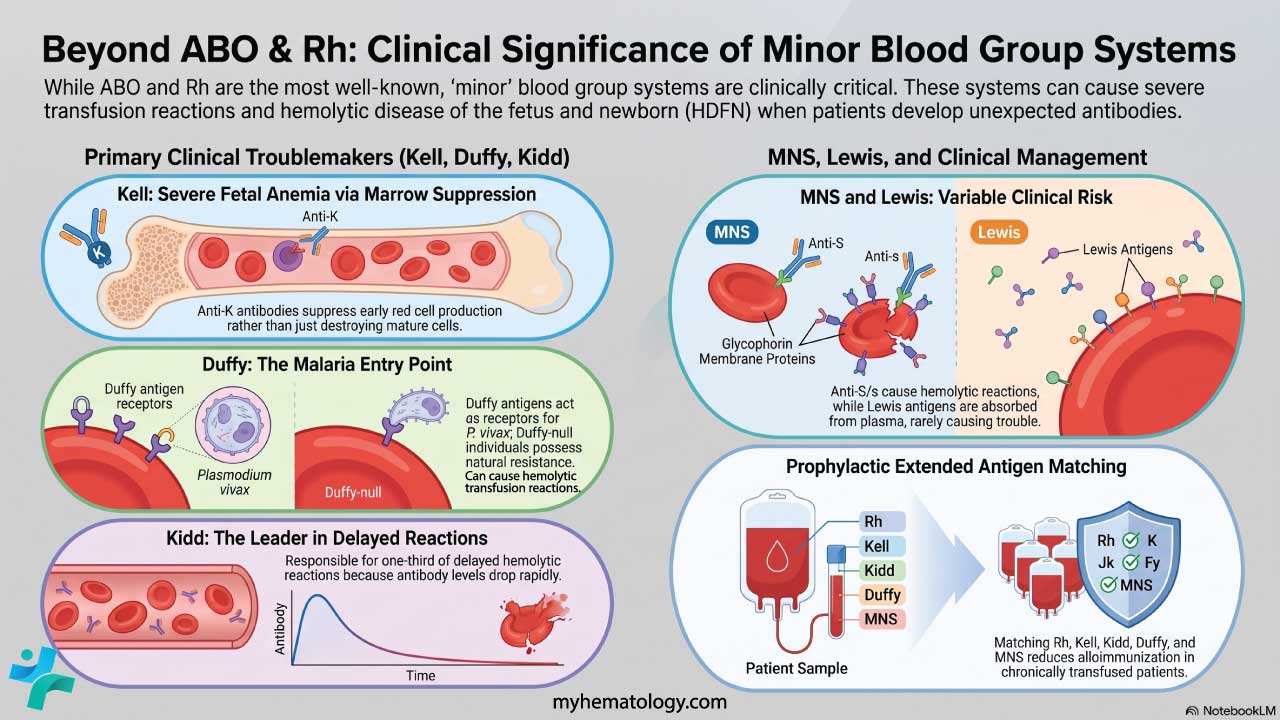
Less common but still important, these reactions occur in patients who have made alloantibodies (usually IgG) after previous transfusions or pregnancies. The most clinically important groups are:
- Kidd (anti-Jka, anti-Jkb). These antibodies fix complement and are notorious for severe acute hemolysis.
- Duffy (anti-Fya, anti-Fyb). Can cause significant hemolysis.
- Kell (anti-K). More often associated with delayed reactions, but acute events occur.
- MNS (anti-M). A rare but documented cause of acute reactions [5].
A specific challenge is the "silent" antibody: levels can fall below the detection threshold of pre-transfusion screening, then rise rapidly after re-exposure (the anamnestic response) and trigger acute hemolysis [3].
ABO-Mismatched Platelets
A less recognized cause is the transfusion of ABO-incompatible platelets. Donor plasma carrying anti-A or anti-B can attack the recipient's red cells, producing AHTR even though the visible product is platelets, not red cells [2]. Group O platelets given to non-O recipients carry the highest risk.
Non-Immune-Mediated Causes
Overheating in an unmonitored warmer or freezing without a cryoprotectant ruptures red cell membranes.
Co-infusing blood with non-isotonic fluids such as 5% dextrose causes red cells to swell and burst. Only 0.9% normal saline (or specifically approved compatible fluids) should share a line with blood.
High-pressure pumps or very small-bore needles shear red cell membranes.
Organisms such as Yersinia enterocolitica and Pseudomonas species release hemolysins and endotoxins that destroy red cells and trigger septic shock [3,7].
Management of AHTR
Treatment is time-critical and built on three priorities: stop the transfusion, stabilize the patient, and protect the kidneys [1].
The First Five Minutes
- Stop the transfusion. Clamp the line. This is the single most important action because every additional milliliter of incompatible blood worsens the reaction.
- Maintain venous access. Do not pull the cannula. Start 0.9% normal saline through a fresh line, or after disconnecting the blood unit at the same site.
- Assess airway, breathing, circulation. Call for help. Activate the rapid response or emergency team.
- Recheck identity. Verify the patient's wristband and the blood component label side by side.
- Notify the blood bank and treating physician immediately.
Supportive Care
| Intervention | Purpose | Details | |
|---|---|---|---|
| Restore circulation and renal perfusion | Aggressive isotonic crystalloid (normal saline or balanced solutions). This is the cornerstone of therapy. [1] | ||
| Maintain mean arterial pressure if fluids are insufficient | Norepinephrine is typically first-line; dopamine is an alternative. | ||
| Flush haemoglobin from renal tubules | Aim for 1–2 mL/kg/hour (roughly ≥100 mL/hour in adults). [1] | ||
| Not Routinely Recommended | Bicarbonate infusion and furosemide were once standard but current evidence does not support routine use. [1] They may still be considered case by case under specialist guidance. | ||
| Control bleeding and clotting | Replace clotting factors with fresh frozen plasma, cryoprecipitate, and platelets, guided by lab results. See: DIC — A Microangiopathy. | ||
| Manage hypoxia | Supplemental oxygen; mechanical ventilation if TRALI or severe pulmonary oedema develops. |
Laboratory Workup
| # | Test | Purpose |
|---|---|---|
| 1 |
Repeat Clerical Check
|
Confirm patient and unit labels match. |
| 2 |
Visual Inspection of Post-Reaction Plasma
|
Pink or red plasma indicates hemoglobinemia. |
| 3 | Detects antibody or complement coating the patient's red cells. | |
| 4 |
Repeat Blood Typing & Crossmatch
|
Compares pre- and post-transfusion samples with the donor unit. |
| 5 | Test for signs of DIC (e.g., PT, PTT, Fibrinogen, D-dimer). | |
| 6 |
Bacterial Culture
|
Send cultures from the patient and the unused portion of the unit to rule out a septic transfusion reaction. |
Beyond the Acute Phase
- Specialist consultation. A hematologist or transfusion medicine specialist should be involved in every severe case.
- Dialysis. Required if acute kidney injury progresses despite supportive care.
- Future transfusions. Should be delayed when possible. When unavoidable, the blood bank issues antigen-negative, phenotype-matched units to reduce further sensitization.
- Hyperhemolysis syndrome. This is destruction of both transfused and the patient's own red cells, most often seen in sickle cell disease. It may need IV immunoglobulin (IVIG), corticosteroids, or the complement inhibitor eculizumab under specialist care [1].
Reporting and Hemovigilance
Every suspected AHTR must be reported to the hospital transfusion committee and the national hemovigilance system, such as SHOT (Serious Hazards of Transfusion) in the UK or the FDA Biological Product Deviation Reporting system in the US [7]. Reporting is not optional. It drives the system-level changes that prevent the next reaction.
Prevention
Because most AHTRs are caused by human error, prevention sits squarely in the hands of clinical teams [1,8].
- Two patient identifiers. Confirm name and date of birth (or equivalent) at every step.
- Two-person bedside check. Two trained staff verify patient identity, blood group, unit number, and expiry against the wristband and the unit.
- Barcode and electronic identification. Where available, scanning the wristband and the unit reduces clerical error dramatically.
- Avoid WBIT errors. Label the sample tube at the bedside, never in advance.
- Slow start, close observation. Run the first 15 minutes slowly with the patient in view.
- Use only compatible fluids. Normal saline is the default; never co-infuse dextrose.
| Reaction | Onset | Key Features | Hemolysis? |
|---|---|---|---|
| AHTR | Minutes to 24 h | Fever, back pain, hypotension, hemoglobinuria, DIC | Yes |
| FNHTR |
During or shortly after | Fever, chills, no hemolysis | No |
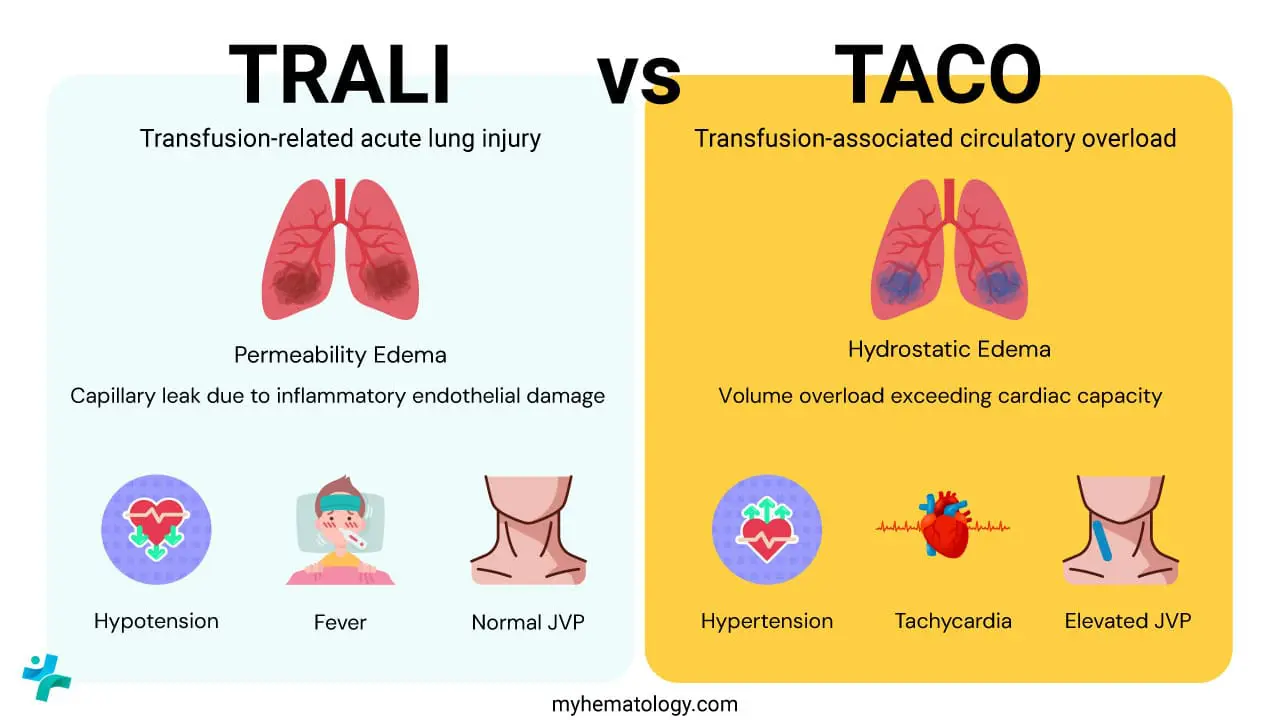
| TRALI | Within 6 h | Acute hypoxia, bilateral lung infiltrates | No |
| TACO | Within 6 h | Pulmonary edema from volume overload, hypertension | No |
| Allergic / Anaphylactic | Minutes | Hives, itching, bronchospasm, hypotension | No |
| Septic transfusion reaction | Minutes to hours | High fever, rigors, shock, positive cultures | Sometimes |
Frequently Asked Questions (FAQs)
What is an acute hemolytic transfusion reaction?
An acute hemolytic transfusion reaction (AHTR) is a medical emergency in which transfused red blood cells are rapidly destroyed inside the recipient's blood vessels, usually within minutes to hours of starting a transfusion. It happens most often when ABO-incompatible blood is given by mistake. Signs include fever, chills, lower back pain, low blood pressure, and dark or red urine. Without quick action it can lead to shock, kidney failure, and death.
What is the most common cause of an Acute Hemolytic Transfusion Reaction (AHTR)?
The most common cause is human error rather than a failure of laboratory testing. Misidentifying a patient at the bedside, mislabeling a blood sample, or hanging the wrong unit can all lead to ABO-incompatible blood being transfused. Because every adult has natural anti-A or anti-B antibodies (or both), even a small volume of incompatible blood can trigger severe intravascular hemolysis.
How quickly does an AHTR occur?
An AHTR can begin within minutes of starting the transfusion and, by definition, occurs within 24 hours. Severe ABO-mediated reactions usually present in the first 5 to 15 minutes. This is why the first 50 mL of every unit should be given slowly with the patient under close observation.
What is the first thing to do if AHTR is suspected?
Stop the transfusion immediately and keep the intravenous line open with normal saline. Then check the patient's identity and the blood unit label, call for help, and start supportive care while sending samples back to the blood bank. Stopping the transfusion is the single most important action because every additional milliliter of incompatible blood worsens the reaction.
How is AHTR different from TRALI, TACO, or an allergic reaction?
All four can cause symptoms during a transfusion, but the mechanism is different. AHTR involves immune destruction of red cells and shows hemoglobinuria and back pain. TRALI is acute lung injury with low oxygen and lung infiltrates. TACO is heart-failure-style fluid overload. Allergic reactions show hives, itching, or, in severe cases, anaphylaxis without hemolysis. Distinguishing them quickly changes the treatment.
Can an AHTR happen with platelet transfusions?
Yes, although it is less common. ABO-mismatched platelets contain donor plasma with anti-A or anti-B antibodies, which can attack the recipient's red cells. Recent case reports highlight that this risk is real and underrecognized, especially when group O platelets are given to non-O recipients [2].
Glossary of Medical Terms
- Hemolysis — the breaking apart of red blood cells, releasing hemoglobin.
- Intravascular hemolysis — red cell destruction inside blood vessels.
- ABO incompatibility — a mismatch between donor red cell antigens and naturally occurring recipient antibodies.
- Antigen — a surface marker the immune system can recognize as self or foreign.
- Alloantibody — an antibody made against antigens from another person.
- Isohemagglutinin — a naturally occurring anti-A or anti-B antibody, usually IgM.
- Complement cascade — a chain of plasma proteins that punches holes in cell membranes.
- Hemoglobinemia — free hemoglobin in plasma; turns it pink or red.
- Hemoglobinuria — free hemoglobin in urine; turns it dark or red.
- Direct antiglobulin test (DAT / Coombs test) — detects antibody or complement bound to the patient's red cells.
- Crossmatch — the final pre-transfusion compatibility check.
- Disseminated intravascular coagulation (DIC) — simultaneous widespread clotting and bleeding.
- Acute kidney injury (AKI) — a sudden drop in kidney function.
- Anamnestic response — rapid antibody rise on re-exposure to an antigen.
- Hyperhemolysis — destruction of both transfused and the patient's own red cells, especially in sickle cell disease.
- Hemovigilance — surveillance of transfusion-related adverse events.
- Wrong blood in tube (WBIT) — a sample labeled with the wrong patient's details.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Hendrickson, J. E., & Fasano, R. M. (2021). Management of hemolytic transfusion reactions. Hematology. American Society of Hematology. Education Program, 2021(1), 704–709. https://doi.org/10.1182/hematology.2021000308
- Zulkeflee, R. H., Hassan, M. N., Hassan, R., Saidin, N. I. S., Zulkafli, Z., Ramli, M., Abdullah, M., Iberahim, S., Roslan, W., Mohd Noor, N. H., & Wan Ab Rahman, W. S. (2023). Acute hemolytic transfusion reaction following ABO-mismatched platelet transfusion: Two case reports. Transfusion and apheresis science : official journal of the World Apheresis Association : official journal of the European Society for Haemapheresis, 62(3), 103658. https://doi.org/10.1016/j.transci.2023.103658
- Rout P, Harewood J, Ramsey A, et al. Hemolytic Transfusion Reaction. [Updated 2023 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448158/
- Serious Hazards of Transfusion (SHOT) Steering Group. (2025). Annual SHOT Report 2024.
- He, Y., Li, Y., & Wang, Q. (2024). Acute hemolytic transfusion reaction caused by anti-M antibodies: a case report and literature review. Laboratory medicine, 55(6), 795–801. https://doi.org/10.1093/labmed/lmae038
- Panch, S. R., Montemayor-Garcia, C., & Klein, H. G. (2019). Hemolytic Transfusion Reactions. The New England journal of medicine, 381(2), 150–162. https://doi.org/10.1056/NEJMra1802338
- Suddock JT, Crookston KP. Transfusion Reactions. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482202/
- Delaney, M., Wendel, S., Bercovitz, R. S., Cid, J., Cohn, C., Dunbar, N. M., Apelseth, T. O., Popovsky, M., Stanworth, S. J., Tinmouth, A., Van De Watering, L., Waters, J. H., Yazer, M., Ziman, A., & Biomedical Excellence for Safer Transfusion (BEST) Collaborative (2016). Transfusion reactions: prevention, diagnosis, and treatment. Lancet (London, England), 388(10061), 2825–2836. https://doi.org/10.1016/S0140-6736(15)01313-6