Key Takeaways
A coagulation screening panel is a group of blood tests that gives a broad picture of how well blood clots. The standard version has three parts: prothrombin time (PT) with INR, activated partial thromboplastin time (aPTT), and platelet count [2].
- PT/INR ▾: Mainly checks the extrinsic and common clotting pathways and is the standard test for monitoring warfarin.
- aPTT ▾: Checks the intrinsic and common pathways and is used to monitor unfractionated heparin and to flag hemophilia [1].
- Platelet count ▾: Measures clotting cells but not their function. A normal number does not guarantee normal platelet behavior.
- A normal panel does not rule out every bleeding disorder. Mild factor deficiencies, von Willebrand disease, and platelet function problems can all hide behind normal results [2]. A normal panel also cannot exclude the newer "blood thinners" (DOACs), which can sit at full treatment levels while PT and aPTT look normal [5,7].
- Before testing means anything, the sample must be collected correctly. Pre-analytical errors, like an underfilled tube, are the most common cause of misleading results.
*Click ▾ for more information
Introduction
Few systems in the body work as quietly and as urgently as the one that stops you from bleeding. Cut a finger, and within seconds a sequence of cells and proteins seals the wound. The coagulation screening panel is how clinicians check that this system is working. For students, it is also one of the most practical pieces of hematology you will learn, because you will read these results on real patients for the rest of your career.
This guide walks through what the panel measures, how to read it, and where it can mislead you. We will keep the science accurate but plain, defining each technical term as it appears.
A coagulation screening panel is a group of blood tests ordered together to assess clotting ability. It gives a broad overview of hemostasis, the process that stops bleeding while keeping blood flowing normally everywhere else.
Brief Overview of Hemostasis & Coagulation
Before reading results, it helps to know what they are testing.
Hemostasis is the body's way of stopping bleeding at an injured vessel without forming clots where they aren't needed. It depends on three players working together: blood vessels, platelets (tiny cell fragments that form the first plug), and coagulation factors (clotting proteins, mostly made in the liver). The goal is a stable clot that seals the damage, followed by orderly clean-up once the vessel heals.
Overview of the Coagulation Cascade

Textbooks traditionally split clotting into three pathways to explain how laboratory tests work. In the human body, however, hemostasis does not occur in isolated fluid; it happens on cell surfaces via the cell-based model of hemostasis. This process occurs in three overlapping phases: initiation (tissue factor generates a thrombin spark), amplification (thrombin activates platelets and co-factors), and propagation (a massive thrombin burst creates the final fibrin clot) [8]. Despite this reality, the traditional cascade model remains essential for reading lab results: PT tests the extrinsic and common pathways, while aPTT tests the intrinsic and common pathways [2].
Here is the short version:
- Extrinsic pathway: The fast trigger. When tissue is damaged, a protein called Tissue Factor meets Factor VII in the blood and kick-starts clotting. This is the main real-life initiator.
- Intrinsic pathway: The amplifier. Triggered when blood contacts damaged vessel surfaces, it runs through a series of contact factors (XII, XI, IX, VIII) to keep clotting going.
- Common pathway: The shared finish line. Both pathways converge on Factor X. From there, the enzyme thrombin is produced, and thrombin converts fibrinogen into fibrin. Factor XIII then cross-links that fibrin into a strong, stable clot.
The reason this matters for interpretation is simple. PT tests the extrinsic and common pathways. aPTT tests the intrinsic and common pathways. Knowing which test covers which pathway is the key to reading the panel.
Why balance matters
Hemostasis is a balancing act. Too little clotting causes bleeding, ranging from easy bruising to life-threatening hemorrhage, as seen in hemophilia (a clotting factor deficiency) or severe thrombocytopenia (a low platelet count). Too much clotting causes thrombosis, where clots block vessels and trigger deep vein thrombosis, pulmonary embolism, heart attack, or stroke. A healthy system clots only where and when needed, then clears the clot afterward.
Why Clinicians Order a Coagulation Screening Panel
The hemostatic system is complex, so a single panel that surveys several parts of it is genuinely useful. The coagulation screening panel earns its place for a handful of clear reasons.
Spotting a bleeding tendency. This is the most common use. Abnormal bleeding may be inherited (like hemophilia) or acquired (like liver disease or vitamin K deficiency). By checking the extrinsic pathway (PT/INR), the intrinsic pathway (aPTT), and the platelet count together, the panel points to which part of the system may be failing and what to test next [2].
Monitoring blood thinners. Two classic drugs are tracked with this panel. Warfarin is monitored with PT/INR. Unfractionated heparin is monitored with aPTT. Both need to sit in a range that prevents clots without causing bleeding.
Important Caveat
Newer oral blood thinners are not reliably tracked by this panel.
Checking liver health. The liver makes most clotting factors. When it fails, those factors drop, and PT/INR rises. A prolonged PT is a sensitive early sign of serious liver dysfunction.
Diagnosing DIC. Disseminated intravascular coagulation (DIC) is a life-threatening state where clotting switches on everywhere at once, using up factors and platelets until the patient paradoxically starts bleeding. The classic panel pattern is a prolonged PT and aPTT with a falling platelet count, usually alongside a raised D-dimer (a clot breakdown product) and low fibrinogen [2].
Investigating unexplained bleeding or clots. When someone bruises easily, bleeds from minor cuts, or has an unexplained clot, this panel is often one of the first tests ordered. It narrows the possibilities and guides more specialized testing.
A note on surgery: routine testing is falling out of favor
Older practice was to run a coagulation screening panel on almost everyone before an operation. The evidence no longer supports this. Current guidance, including NICE NG45 and multiple reviews through 2024, recommends against routine coagulation testing in healthy, low-risk patients with no bleeding history [3,4]. A careful bleeding history predicts surgical bleeding risk better than a blanket screen does. Testing is now reserved for patients with a bleeding history, a relevant condition such as liver disease, or those on anticoagulants.
Components of the Panel
Prothrombin Time (PT) and International Normalized Ratio (INR)
What it measures. PT is the time it takes plasma to clot after adding tissue factor (also called thromboplastin) and calcium. It tests the extrinsic pathway (Factor VII) and the common pathway (Factors X, V, II, and I).
How it works. Blood is drawn into a tube with sodium citrate, which holds clotting in check by binding calcium. In the lab, tissue factor and calcium are added back. The added tissue factor switches on Factor VII directly. The time to the first visible clot is recorded in seconds.
The INR. Different labs use reagents of different strengths, so the same sample could give different PT values in different places. The International Normalized Ratio (INR) corrects for this so results mean the same thing everywhere. It is calculated as:
INR = (Patient's PT ÷ Mean Normal PT) raised to the power of the ISI
Here, the Mean Normal PT is the lab's average for healthy people, and the ISI (International Sensitivity Index) describes how sensitive that batch of reagent is. The INR is what makes safe, consistent warfarin dosing possible.
Clinical uses. PT/INR is the primary screen for the extrinsic and common pathways. Its biggest use by far is monitoring warfarin, which blocks the vitamin K–dependent factors (II, VII, IX, X). Because Factor VII has the shortest lifespan, PT reacts early to warfarin and to vitamin K deficiency. PT/INR also tracks liver disease severity and rises in DIC as factors are consumed [1,2].
When PT/INR is prolonged. A prolonged result means clotting through these pathways is slow. Common causes include warfarin therapy, liver disease, vitamin K deficiency, DIC, factor deficiencies, circulating inhibitors, and pre-analytical errors. A shortened PT is rare and usually not meaningful on its own. It can occur when Factor VIII and fibrinogen rise during inflammation, since these proteins climb as part of the body's acute response. Always read PT/INR alongside the patient's history, medications, and other results.
Activated Partial Thromboplastin Time (aPTT)
What it measures. aPTT is the time plasma takes to clot after adding an activator, a partial thromboplastin (phospholipid), and calcium. It tests the intrinsic pathway (Factors XII, XI, IX, VIII) and the common pathway (Factors X, V, II, I).
How it works. As with PT, blood is collected in citrate and the plasma separated. The lab adds an activator to switch on the intrinsic contact factors, then adds calcium to let clotting proceed. The "partial" thromboplastin lacks tissue factor, which is what distinguishes it from the PT reagent.
Clinical uses. aPTT is the main screen for the intrinsic and common pathways. Its key roles are:
- Monitoring unfractionated heparin, which boosts antithrombin to shut down thrombin and Factor Xa. Heparin strongly prolongs aPTT.
- Detecting hemophilia A and B, caused by Factor VIII and Factor IX deficiency. Both factors live in the intrinsic pathway, so a deficiency prolongs aPTT and prompts specific factor testing [1].
- Flagging severe von Willebrand disease, which can lower Factor VIII and so prolong aPTT.
- Revealing lupus anticoagulant, an antibody that prolongs aPTT in the test tube but actually raises clotting risk in the body. A prolonged aPTT in someone with clots or recurrent miscarriage should prompt specific testing.
When aPTT is prolonged. Causes include heparin therapy, deficiencies in the intrinsic or common pathway factors, inhibitors (such as lupus anticoagulant or an acquired Factor VIII inhibitor), severe liver disease, severe vitamin K deficiency, and DIC. When the cause isn't obvious, a mixing study comes next. The patient's plasma is mixed with normal plasma. If the result corrects, a factor is missing. If it doesn't correct, an inhibitor is present. That distinction changes management completely.
Critical Caveat
Some inhibitors, specifically Factor VIII inhibitors (acquired hemophilia), are time- and temperature-dependent. An immediate mixing study might falsely correct, masking the problem. If clinical suspicion for an inhibitor is high, labs must perform an "incubated mix" (waiting 1 to 2 hours at 37°C) to ensure a life-threatening inhibitor is not missed [9].
Platelet Count
What it measures. The platelet count is the number of platelets in a set volume of blood. Platelets are anucleated cell fragments from bone marrow megakaryocytes, and they drive primary hemostasis, the first plug at a wound.
How it works. Blood is collected in EDTA and counted by an automated analyzer, then reported per microliter or per liter in the complete blood count.
An important limit: the count measures how many platelets there are, not how well they work.
Clinical uses. The count detects thrombocytopenia (too few platelets) and thrombocytosis (too many). Low counts cause bleeding, especially mucocutaneous bleeding like petechiae, purpura, nosebleeds, and gum bleeding. Causes split into reduced production (bone marrow failure, leukemia, chemotherapy, viral infection), increased destruction or consumption (immune thrombocytopenia, TTP, HUS, heparin-induced thrombocytopenia, DIC), sequestration in an enlarged spleen, and dilution after massive transfusion. High counts may be reactive (responding to infection, inflammation, or iron deficiency) or primary (a myeloproliferative neoplasm such as essential thrombocythemia), the latter carrying real clotting and bleeding risk.
Interpreting the count. As a rough guide:
- 100–150 ×10⁹/L is usually mild and symptom-free
- 50–100 ×10⁹/L may cause easy bruising
- 20–50 ×10⁹/L brings moderate spontaneous bleeding risk
- < 20 ×10⁹/L carries a high risk of serious spontaneous bleeding, including intracranial hemorrhage.
- On the high side, mild rises (450–800 ×10⁹/L) are often reactive, while marked rises (over 1000 ×10⁹/L) raise concern, including a paradoxical bleeding risk from acquired von Willebrand disease.
Reading the Panel: Putting It Together
Interpretation moves from single results, to combined patterns, to the patient in front of you.
Always start with the clinical context
Is the patient bleeding or clotting? What is their history of liver disease, autoimmune conditions, or family bleeding disorders? What medications are they on? Anticoagulants are often the simplest explanation for an abnormal result. Any recent trauma, surgery, sepsis, or transfusion also matters.
Know your reference ranges
Use your own lab's ranges, since reagents and instruments vary. Typical approximate adult ranges are:
- PT: 10–14 seconds
- INR: 0.8–1.2 (when not on anticoagulants)
- aPTT: 25–40 seconds
- Platelet count: 150–450 ×10⁹/L
Common patterns at a glance
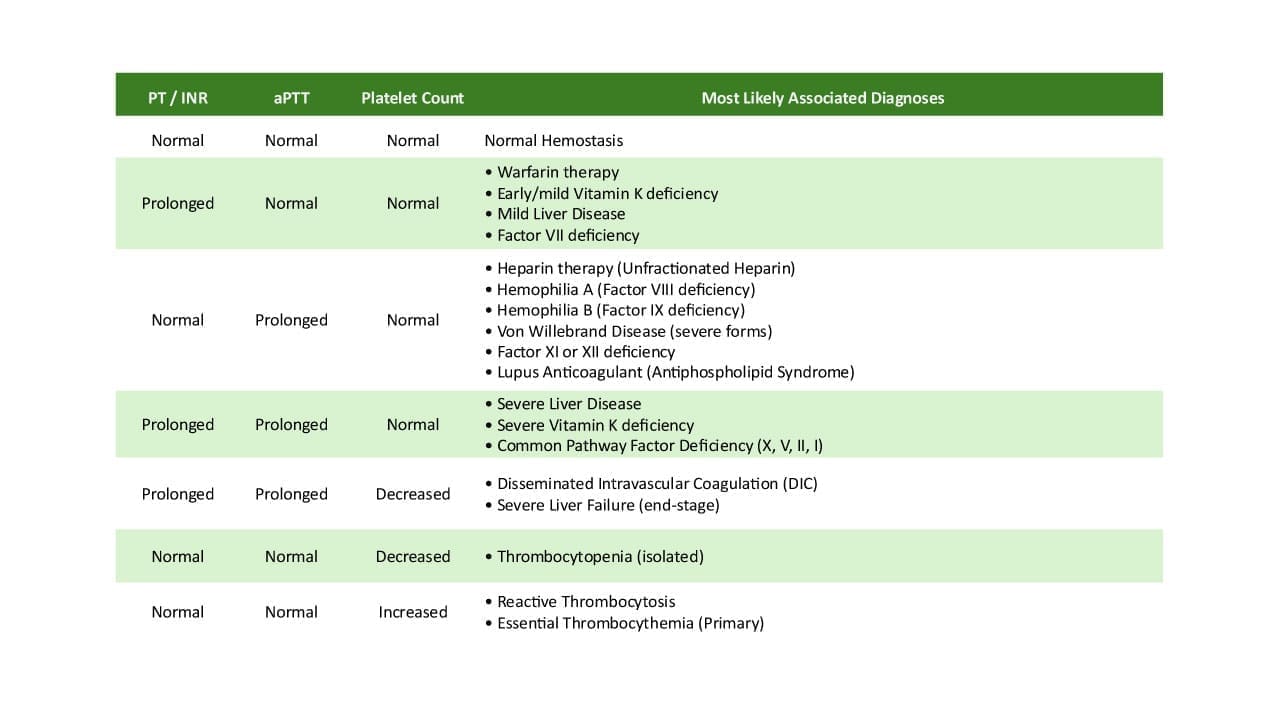
- All normal: Reassuring, but it does not exclude every bleeding disorder. Mild factor deficiencies, platelet function disorders, and mild von Willebrand disease can still cause bleeding [2].
- Prolonged PT, normal aPTT: Points to the extrinsic pathway. Think warfarin first, then vitamin K deficiency, early liver disease, or rare Factor VII deficiency.
- Normal PT, prolonged aPTT: Points to the intrinsic pathway. Think heparin, hemophilia A or B, von Willebrand disease, or an inhibitor like lupus anticoagulant. A mixing study sorts deficiency from inhibitor.
- Both PT and aPTT prolonged, normal platelets: Points to the common pathway or a broad problem like severe liver disease or severe vitamin K deficiency.
- Both prolonged, low platelets: The classic DIC pattern. Treat as urgent and look for the cause (sepsis, trauma, malignancy, obstetric complications).
- Normal PT and aPTT, low platelets: A primary platelet problem. Consider production, destruction, sequestration, or dilution, and always confirm with a blood smear to exclude pseudothrombocytopenia (clumping in the EDTA tube).
- Normal PT and aPTT, high platelets: Thrombocytosis, usually reactive, occasionally primary.
The Modern Blind Spot: DOACs and the Standard Panel
This section addresses a point the classic teaching often misses, and it matters for patient safety.
Direct oral anticoagulants (DOACs), such as apixaban, rivaroxaban, and dabigatran, are now among the most common blood thinners. Unlike warfarin and heparin, they are not reliably measured by PT and aPTT. A patient can be fully anticoagulated on a DOAC and still show a normal PT and a normal aPTT [5].
The numbers make the point. In one study, 80% of samples with a normal aPTT and 50% with a normal PT still carried a surgically relevant level of rivaroxaban [7]. The effects also differ by drug. Dabigatran tends to prolong aPTT but a normal aPTT does not exclude it. Rivaroxaban and edoxaban can prolong PT, while apixaban barely affects either test [6].
The practical lesson: a normal coagulation screening panel does not mean a patient is free of a DOAC, and it does not mean they are safe to undergo an invasive procedure. When a DOAC level needs to be known, specific assays such as anti-Xa activity or a dilute thrombin time are required [6].
Beyond the Standard Panel: TEG and ROTEM
The classic screening panel has a major limitation: it tests isolated plasma and stops the moment the first strand of fibrin forms. In acute, high-bleeding-risk settings like trauma, major surgery, and obstetrics, clinicians frequently rely on viscoelastic testing, namely thromboelastography (TEG) and rotational thromboelastometry (ROTEM). These assays measure whole blood in real-time, generating a graph that displays how fast the clot forms, its maximum structural strength, and whether it breaks down too quickly (hyperfibrinolysis) [10].
When Results Mislead: Factors Affecting the Panel
Accurate interpretation depends on an accurate sample. Coagulation tests are sensitive, and most errors happen before analysis even begins.
Pre-analytical errors (the most common)
These occur between the blood draw and testing.
- Difficult or traumatic draws can activate clotting or cause hemolysis, skewing results in either direction.
- The blood-to-citrate ratio (9:1) must be right. An underfilled tube leaves excess citrate, which binds too much calcium and falsely prolongs PT and aPTT. This is one of the most common errors. An overfilled tube can allow microclots that consume factors.
- Heparin contamination from a flushed IV line can markedly prolong aPTT.
- High hematocrit (over about 55–60%) reduces plasma volume, leaving relatively too much citrate and falsely prolonging results.
- Delays and poor handling matter because labile factors (V and VIII) degrade over time, and inadequate centrifugation leaves platelet fragments that distort results.
- Hemolysis, high bilirubin, and high lipids can all interfere with the analyzer's clot detection.
Analytical factors
Reagent strength varies (which is exactly why INR exists), and reagents degrade if stored poorly or expired. Labs must calibrate instruments and run quality controls. Different clot-detection methods carry different sensitivities.
Patient-related factors
Beyond the drugs and diseases already covered, remember that pregnancy is a hypercoagulable state that can slightly shorten clotting times, and neonates have naturally lower vitamin K–dependent factors, reaching adult levels by around six months. Renal failure can impair platelet function, and many systemic illnesses, from sepsis to thyroid disorders, can shift results.
Frequently Asked Questions (FAQs)
What does a coagulation screening panel actually test?
A coagulation screening panel measures how well your blood forms clots. The standard version includes three parts: prothrombin time (PT) with INR, activated partial thromboplastin time (aPTT), and platelet count. Together they give a broad picture of the clotting system and help doctors decide whether more specific tests are needed.
What is the difference between PT and aPTT?
PT checks the extrinsic and common clotting pathways and is mainly used to monitor the drug warfarin and to assess liver function. aPTT checks the intrinsic and common pathways and is used to monitor unfractionated heparin and to help detect hemophilia. When both are prolonged, the problem usually lies in the shared "common pathway" or reflects a widespread issue like severe liver disease or DIC.
Can the panel detect every bleeding disorder?
No. A normal panel does not rule out all bleeding problems. Mild factor deficiencies, platelet function disorders, and mild von Willebrand disease can all cause bleeding while PT, aPTT, and platelet count look normal. If a person clearly bleeds abnormally, further specialized testing is needed even when the screen is normal.
Will the panel show whether someone is on a blood thinner?
Not reliably for the newer drugs. The panel works well for warfarin (via INR) and unfractionated heparin (via aPTT). But direct oral anticoagulants (DOACs) like apixaban and rivaroxaban can be present at full treatment levels while PT and aPTT still look normal. Detecting these drugs requires specific assays such as anti-Xa activity.
Why might a test result be wrong even when clotting is normal?
Most coagulation errors happen before testing begins. A tube filled below the line, a difficult blood draw, contamination from a heparin line, or a delay in processing can all falsely prolong or shorten results. This is why an unexpected result is often repeated before any diagnosis is made.
Is this panel always needed before surgery?
Not for everyone. Current guidance recommends against routinely testing healthy, low-risk patients with no bleeding history. A careful history of bleeding tendencies predicts surgical bleeding risk better than a screening panel does. Testing is reserved for patients with a bleeding history, a relevant medical condition, or those on anticoagulants.
Glossary of Related Medical Terms
- Hemostasis: The body's process for stopping bleeding at an injured blood vessel while keeping blood flowing normally everywhere else.
- Coagulation cascade: A chain reaction of clotting proteins (factors) that ends in a stable clot. It is partly a laboratory model of how clotting is tested, not a perfect map of clotting in the body.
- Coagulation factor: A protein in blood that helps form a clot. Most are made in the liver. They are numbered with Roman numerals (I through XIII).
- Prothrombin time (PT): A test of how fast blood clots through the extrinsic and common pathways. Mainly used to monitor warfarin and check liver function.
- INR (International Normalized Ratio): A standardized version of the PT so results mean the same thing across different labs. Used to dose warfarin safely.
- aPTT (activated partial thromboplastin time): A test of the intrinsic and common pathways. Used to monitor unfractionated heparin and to detect hemophilia.
- Platelet: A tiny cell fragment that forms the first plug at a wound. Made in the bone marrow.
- Thrombocytopenia: A low platelet count, which raises bleeding risk.
- Thrombocytosis: A high platelet count, which can raise clotting risk.
- Thrombosis: A blood clot forming inside a vessel where it shouldn't, blocking blood flow.
- DIC (disseminated intravascular coagulation): A dangerous condition where clotting is switched on everywhere at once, using up clotting factors and platelets, which then causes bleeding.
- DOAC (direct oral anticoagulant): A newer class of "blood thinners" (such as apixaban, rivaroxaban, dabigatran) that the standard panel does not reliably measure.
- D-dimer: A breakdown product of clots. High levels suggest active clot formation and breakdown, as in DIC or a suspected clot.
- Mixing study: A follow-up test that mixes a patient's plasma with normal plasma to tell whether a prolonged result is from a missing factor or from an inhibitor.
- Lupus anticoagulant: An antibody that makes the aPTT look prolonged in the lab but actually raises clotting risk in the body.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Raber MN. Coagulation Tests. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 157. Available from: https://www.ncbi.nlm.nih.gov/books/NBK265/
- Zaidi SRH, Rout P. Interpretation of Blood Clotting Studies and Values (PT, PTT, aPTT, INR, Anti-Factor Xa, D-Dimer) [Updated 2025 Oct 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK604215/
- van Veen, J. J., Spahn, D. R., & Makris, M. (2011). Routine preoperative coagulation tests: an outdated practice?. British journal of anaesthesia, 106(1), 1–3. https://doi.org/10.1093/bja/aeq357
- National Institute for Health and Care Excellence. (2016). Routine preoperative tests for elective surgery (NICE Guideline NG45). https://www.nice.org.uk/guidance/ng45
- Adcock, D. M., & Gosselin, R. C. (2017). The danger of relying on the APTT and PT in patients on DOAC therapy, a potential patient safety issue. International journal of laboratory hematology, 39 Suppl 1, 37–40. https://doi.org/10.1111/ijlh.12658
- Bazydlo, L. A. L., Marin, M. J., Merrill, A. E., Man, L. M., Oladipo, O. O., & Harris, N. S. (2025). ADLM Guidance Document on Coagulation Testing in Patients Using Direct Oral Anticoagulants. The journal of applied laboratory medicine, 10(6), 1675–1690. https://doi.org/10.1093/jalm/jfaf155
- Kaserer, A., Schedler, A., Seifert, B., Spahn, D. R., Studt, J. D., & Stein, P. (2019). Standard coagulation assays alone are not sufficient to exclude surgically relevant rivaroxaban plasma concentrations. Perioperative medicine (London, England), 8, 15. https://doi.org/10.1186/s13741-019-0128-9
- Hoffman, M., & Monroe, D. M., 3rd (2001). A cell-based model of hemostasis. Thrombosis and haemostasis, 85(6), 958–965. https://doi.org/10.1055/s-0037-1615947
- Kershaw, G., & Orellana, D. (2013). Mixing tests: Diagnostic aides in the investigation of prolonged prothrombin times and activated partial thromboplastin times. Seminars in Thrombosis and Hemostasis, 39(3), 283–290. https://doi.org/10.1055/s-0033-1336832
- Whiting, D., & DiNardo, J. A. (2014). TEG and ROTEM: Technology and clinical applications. American Journal of Hematology, 89(2), 228–232. https://doi.org/10.1002/ajh.23599