Key Takeaways
Fibrinolysis is the enzyme-driven process that dissolves a blood clot once it has done its job, restoring blood flow and preventing dangerous clot extension.
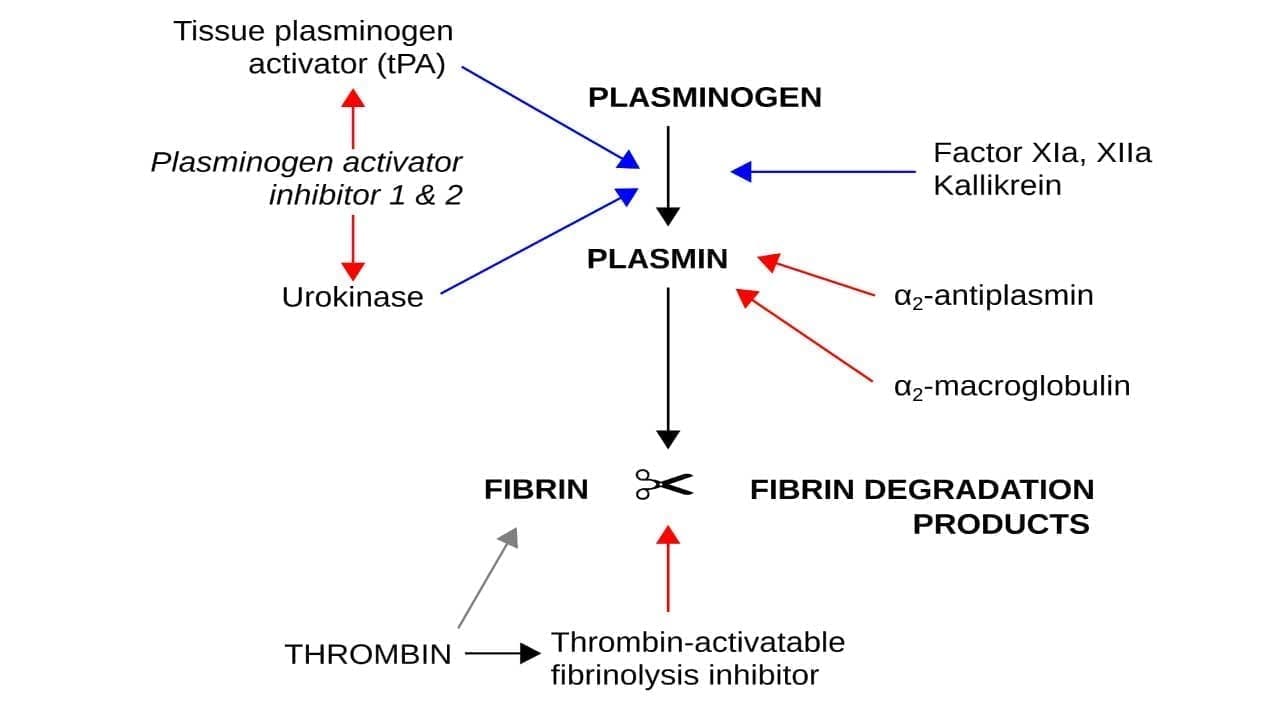
- Essential Players ▾: The central enzyme is plasmin, made on demand from circulating plasminogen by two activators: tPA (mostly at the clot surface) and uPA (mostly in tissues).
- Disorders ▾: An imbalance in fibrinolysis causes disease as too much activity leads to bleeding (hyperfibrinolysis); too little leads to thrombosis (hypofibrinolysis).
- Investigations ▾: Diagnosis relies on specialized tests including the euglobulin clot lysis time, thromboelastography, D-dimer, and specific assays for PAI-1 and α2-antiplasmin.
- Treatment and management ▾: Thrombolytic drugs such as alteplase and tenecteplase harness fibrinolysis to treat ischemic stroke, ST-elevation myocardial infarction (STEMI), and pulmonary embolism [4].
*Click ▾ for more information
Why Fibrinolysis Matters
Every day, your body forms tiny clots to seal microscopic vessel injuries you never feel. Without a way to remove those clots, blood vessels would slowly clog. Fibrinolysis is the cleanup system that prevents this. It also explains why drugs given in the first hours of a stroke can save brain tissue, and why a missing protein no bigger than a few hundred amino acids can cause lifelong bleeding [1].
This article walks through the players, the pathways, the disorders, and the modern treatments that all depend on understanding fibrinolysis.
Hemostasis in Brief
Hemostasis keeps blood flowing freely while sealing leaks the moment a vessel is injured. It rests on a balance between two opposing systems.
Coagulation builds the plug. Platelets rush to the injury and stick together, forming the initial primary plug. The coagulation cascade then converts soluble fibrinogen into fibrin, a mesh that locks the platelet plug into a stable clot. Calcium ions and factor XIIIa cross-link the mesh for extra strength.
Fibrinolysis takes the plug apart. Once tissue underneath has healed, plasminogen is activated to plasmin, which snips the fibrin mesh into soluble fragments. Blood flow returns, and tissue regeneration continues.
When this balance tips toward coagulation, dangerous clots can form inside intact vessels, causing deep vein thrombosis, pulmonary embolism, or stroke. When it tips toward fibrinolysis, clots dissolve too soon and bleeding follows. Both extremes are clinical emergencies [1,7].
The Key Players in Fibrinolysis
Think of fibrinolysis as a small cast with very specific roles: a precursor, an enzyme, two activators, and three brakes.
Plasminogen and Plasmin
Plasminogen is the inactive precursor (a zymogen) that circulates in plasma at roughly 200 mg/L. It binds fibrin with high affinity, which concentrates it exactly where it will be needed. When activated by cleavage of a single peptide bond, it folds into plasmin, a powerful serine protease that cuts fibrin into soluble degradation products [2].
Plasmin is potent, so the body never lets it work freely. Activation, action, and inactivation are all tightly controlled at the clot surface.
The Activators
- Tissue plasminogen activator (tPA) is released from endothelial cells. It is most active when bound to fibrin, which means it generates plasmin almost exclusively at the clot itself. This fibrin specificity is also why tPA is the basis of stroke and heart attack thrombolysis [1,4].
- Urokinase plasminogen activator (uPA) works mainly in tissues and at vessel walls, often via its receptor uPAR. It plays a larger role in tissue remodeling and inflammation than in dissolving intravascular clots.
- Streptokinase is a bacterial protein that activates plasminogen non-specifically. It is cheaper than tPA but carries higher bleeding and immune risks, and is now rarely used in high-income settings.
The Brakes
- α2-antiplasmin is the fastest brake. It binds free plasmin almost instantly, forming an irreversible complex. Patients who lack α2-antiplasmin bleed because plasmin runs unchecked [2].
- Plasminogen activator inhibitor-1 (PAI-1) blocks tPA and uPA before they can activate plasminogen. PAI-2, a related protein, regulates uPA in tissues.
- Thrombin activatable fibrinolysis inhibitor (TAFI) is the molecular link between coagulation and fibrinolysis. Thrombin (especially when bound to thrombomodulin) activates TAFI to TAFIa, which strips C-terminal lysine residues from partially cut fibrin. Those lysines are the docking sites that let more plasminogen bind, so removing them shuts down the positive feedback loop and protects the clot from premature lysis [3].
Supporting Cast
- Fibrin is the substrate, not just scaffolding. Its structure (fiber thickness, density, lysine residues) directly determines how easily plasmin can dismantle it [2,9].
- Annexin A2 sits on endothelial cells and helps tPA and plasminogen meet on the cell surface.
- Lipoprotein(a) competes with plasminogen for fibrin-binding sites, slowing fibrinolysis. High Lp(a) is now recognized as an independent thrombotic risk factor [7].
The Process of Fibrinolysis
Plasminogen waits in the blood for one of two activation routes. Both end with plasmin chewing through fibrin, but they operate in different places.
tPA Pathway: Action at the Clot
This is the dominant intravascular pathway. Endothelial cells release tPA into the blood. When tPA encounters fibrin, it changes shape and gains the ability to activate plasminogen efficiently. Because tPA strongly prefers fibrin-bound plasminogen, plasmin is generated where it is needed and almost nowhere else. This is the principle behind alteplase and tenecteplase therapy [1,4].
uPA Pathway: Action in Tissues
uPA binds its cell-surface receptor uPAR and activates plasminogen on the membrane of cells lining vessels and within tissue. It contributes less to dissolving large intravascular clots and more to tissue remodeling, wound healing, and cell migration. New plasmin can also activate more uPA in a positive feedback loop, but the loop is contained locally.
Pulling Fibrin Apart
Plasmin cuts fibrin at specific sites, releasing soluble fragments including D-dimer, a marker measured clinically to detect active clotting and breakdown. As plasmin works, partially degraded fibrin exposes new C-terminal lysines that recruit more plasminogen, accelerating lysis unless TAFIa has already removed those lysines.
Why Localization Matters
Fibrinolysis is dangerous if it spreads. The combined action of α2-antiplasmin, PAI-1, TAFIa, and the fibrin-specific behavior of tPA all act to keep plasmin generation tied to the clot. When this localization fails, bleeding follows.
When Fibrinolysis Goes Wrong
A useful way to think about disordered fibrinolysis is to ask: is the system too active, or not active enough?
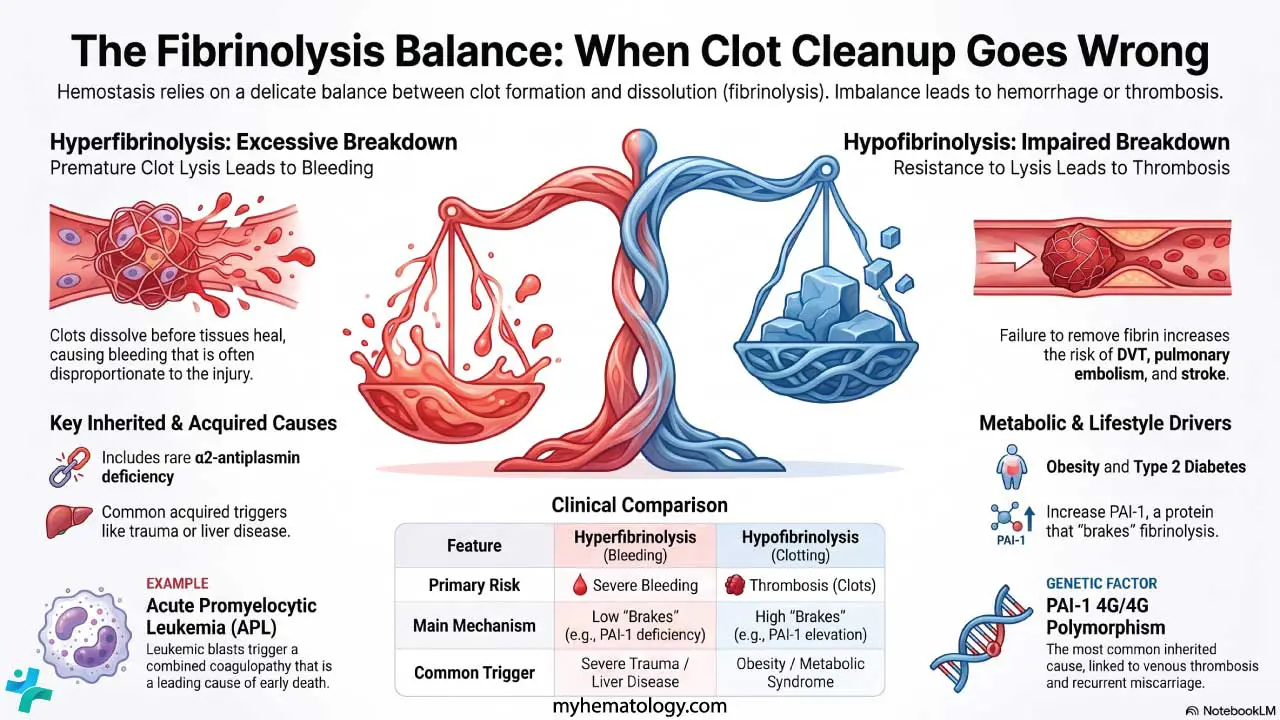
Hyperfibrinolysis: Too Much Breakdown, Too Much Bleeding
Premature clot lysis leads to bleeding that is often disproportionate to the injury.
Inherited causes are rare:
- α2-antiplasmin deficiency — autosomal recessive; plasmin runs unopposed.
- PAI-1 deficiency — leads to enhanced plasmin generation.
- Quebec platelet disorder — platelets contain excess uPA that lyses clots from within.
Acquired causes are more common:
- Severe trauma with hypoperfusion — triggers an overwhelming fibrinolytic response.
- Advanced liver disease — the liver makes most fibrinolytic regulators, so cirrhosis tips the balance.
- DIC — paradoxically combines widespread clotting with consumption-driven bleeding.
- Acute promyelocytic leukemia (APL) — leukemic blasts release procoagulant and profibrinolytic activity, causing a combined coagulopathy that is the leading cause of early death. All-trans retinoic acid (ATRA) is started immediately on suspicion, even before genetic confirmation.
Hypofibrinolysis: Too Little Breakdown, Too Much Clotting
Impaired clot lysis raises the risk of deep vein thrombosis, pulmonary embolism, and myocardial infarction.
Inherited causes:
- PAI-1 4G/4G polymorphism — the most common inherited cause; produces more PAI-1, suppressing fibrinolysis. Linked to venous thrombosis and recurrent miscarriage.
- Elevated lipoprotein(a) — competes with plasminogen for fibrin, reducing lysis [7].
Acquired causes:
- Obesity, insulin resistance, type 2 diabetes, and metabolic syndrome — adipose tissue is a major source of PAI-1.
- Dyslipidemia — elevated triglycerides correlate with higher PAI-1.
- Chronic inflammation — autoimmune disease raises antifibrinolytic factors.
- Aging — PAI-1 rises with age, contributing to thrombotic cardiovascular disease in older adults.
Investigating Disordered Fibrinolysis
Standard clotting tests usually look normal in fibrinolysis disorders, so a high index of suspicion is essential.
Global assays look at the system as a whole:
- Euglobulin clot lysis time (ECLT) — a shortened time suggests hyperfibrinolysis.
- Thromboelastography (TEG) and ROTEM — point-of-care tests that show clot formation and lysis in real time, used heavily in trauma and cardiac surgery. Increasingly, artificial intelligence and machine learning models are being developed in hemorrhagic trauma care to predict massive transfusion needs and identify coagulopathies [10].
Specific assays measure individual proteins:
- α2-antiplasmin activity and antigen.
- PAI-1 activity and antigen.
- tPA and uPA assays.
Breakdown products:
- D-dimer and fibrin degradation products (FDPs) — sensitive but not specific. They rise in DIC, venous thromboembolism, infection, pregnancy, and aortic dissection.
Genetic testing is added when an inherited disorder is suspected, for example to confirm PAI-1 4G/4G or α2-antiplasmin gene mutations.
Treatment and Management
The goal is always to restore the hemostatic balance. The treatment depends entirely on which way the balance has tipped.
Managing Hyperfibrinolysis
The cornerstone is antifibrinolytic therapy, which blocks plasminogen from binding fibrin:
- Tranexamic acid (TXA) — a lysine analog used in trauma, surgery, postpartum hemorrhage, and heavy menstrual bleeding. The CRASH-2 trial showed that in trauma, TXA reduces death from bleeding when given within 3 hours of injury; later administration may be harmful [6]. Additionally, the CRASH-3 trial demonstrated that TXA improves survival in patients with mild-to-moderate isolated traumatic brain injury when administered promptly, though it is less effective for severe head injuries [11].
- Epsilon-aminocaproic acid (EACA) — similar mechanism, used in surgical and inherited bleeding contexts.
Supportive care matters in severe bleeding: packed red blood cells for anemia, fresh frozen plasma to replace clotting factors, and platelet transfusion for thrombocytopenia. The underlying cause (trauma, liver failure, DIC, APL) must be treated in parallel.
Managing Hypofibrinolysis
Long-term anticoagulation prevents future clots:
- Direct oral anticoagulants (DOACs) — apixaban, rivaroxaban, edoxaban, dabigatran. When hyperfibrinolysis or emergency bleeding occurs, specific reversal agents such as idarucizumab (for dabigatran) and andexanet alfa (for factor Xa inhibitors) are critical adjuncts to restore hemostatic balance [12].
- Factor XI and XII inhibitors (e.g., asundexian, abelacimab) — emerging classes of anticoagulants that decouple hemostasis from thrombosis. They prevent clots without significantly increasing bleeding risk because they leave the body's native fibrinolytic and primary coagulation systems largely intact [13].
- Warfarin — vitamin K antagonist, still used where DOACs are unsuitable.
- Heparin (unfractionated and low-molecular-weight) — for short-term and inpatient management.
Thrombolytic therapy is reserved for life-threatening events such as ischemic stroke, STEMI, or massive pulmonary embolism. Modern options include:
- Alteplase (recombinant tPA) — long the standard agent for stroke within 4.5 hours [4].
- Tenecteplase (TNK) — a genetically modified tPA with greater fibrin specificity and a longer half-life. Given as a single bolus rather than an infusion, it is increasingly surpassing alteplase as the standard of care for acute ischemic stroke in major guidelines [14]. Its single-bolus nature enables rapid pre-hospital administration in mobile stroke units. Furthermore, for severe strokes involving large vessel occlusions, chemical thrombolysis with TNK is now routinely administered concurrently before mechanical thrombectomy (endovascular clot retrieval) because it significantly improves initial reperfusion rates and functional outcomes [15].
- Reteplase — used in STEMI, given as two boluses.
- Urokinase — older agent, still used in some catheter-directed protocols.
- Streptokinase — largely replaced in high-income countries due to immunogenicity.
For pulmonary embolism, catheter-directed and ultrasound-facilitated low-dose thrombolysis can deliver the drug straight to the clot, reducing systemic bleeding risk. Newer agents such as recombinant non-immunogenic staphylokinase are under investigation [9].
Lifestyle and comorbidity management is essential. Weight loss, exercise, and treatment of diabetes and dyslipidemia all reduce PAI-1 and improve fibrinolytic potential.
Beyond Fibrin: Why Some Clots Resist Lysis
A practical limitation of all current thrombolytics is that they target fibrin only. Real clots also contain platelet aggregates, neutrophil extracellular traps (NETs), extracellular DNA, von Willebrand factor multimers, and matrix proteins. These non-fibrin components can make up half or more of a clot and remain after plasmin has done its work. Adjuncts such as DNase and ADAMTS13 are being studied to address this gap, though none are yet standard care [9]. Understanding clot composition helps explain why thrombolysis sometimes fails despite correct dosing and timing.
Frequently Asked Questions (FAQs)
What is fibrinolysis in simple terms?
Fibrinolysis is the body's natural process of dissolving a blood clot once a wound has healed. The enzyme plasmin cuts the fibrin mesh holding the clot together, restoring normal blood flow and preventing clots from blocking blood vessels.
What is the difference between fibrinolysis and thrombolysis?
Fibrinolysis is the body's own clot-dissolving process and runs continuously. Thrombolysis is a medical treatment that uses drugs such as alteplase or tenecteplase to dissolve a dangerous clot quickly during emergencies like ischemic stroke or heart attack. Thrombolysis works by giving fibrinolysis a powerful boost.
What drugs are used for thrombolysis?
The main thrombolytic drugs are alteplase (recombinant tPA), tenecteplase, reteplase, urokinase, and streptokinase. Tenecteplase is increasingly preferred for acute ischemic stroke because it is given as a single bolus, has a longer half-life, and is non-inferior to alteplase in major trials [4,5].
Why does tranexamic acid stop bleeding?
Tranexamic acid blocks plasminogen from binding to fibrin, so plasmin cannot form efficiently at the clot surface. This protects clots from premature breakdown. It is used in trauma, surgical bleeding, postpartum hemorrhage, and heavy menstrual bleeding. In trauma, it works best when given within 3 hours of injury [6].
What disorders are linked to abnormal fibrinolysis?
Hyperfibrinolysis causes bleeding and is seen in α2-antiplasmin deficiency, Quebec platelet disorder, severe trauma, advanced liver disease, DIC, and acute promyelocytic leukemia. Hypofibrinolysis raises clotting risk and is linked to PAI-1 4G/4G polymorphism, elevated lipoprotein(a), obesity, type 2 diabetes, and metabolic syndrome.
How is disordered fibrinolysis diagnosed?
Routine clotting tests like prothrombin time and APTT are usually normal. Specialized tests are needed: the euglobulin clot lysis time, thromboelastography (TEG) and ROTEM, individual assays for α2-antiplasmin and PAI-1, and D-dimer to detect ongoing clot breakdown. Genetic testing is added when an inherited disorder is suspected.ding problems.
Glossary of Related Medical Terms
- Fibrinolysis — the body's enzyme-driven process of dissolving a blood clot once it is no longer needed.
- Plasminogen — an inactive precursor protein circulating in blood; converted into plasmin to break down clots.
- Plasmin — the active enzyme that cuts fibrin strands and dissolves the clot.
- Fibrin — the protein mesh that holds a blood clot together.
- tPA (tissue plasminogen activator) — the main enzyme that activates plasminogen at the surface of a clot; also a drug used for stroke and heart attack.
- uPA (urokinase plasminogen activator) — an activator of plasminogen that works mainly in tissues and at vessel walls.
- Tenecteplase (TNK) — a modified, longer-acting form of tPA used as a thrombolytic drug.
- PAI-1 (plasminogen activator inhibitor-1) — the main brake on tPA and uPA; high levels reduce clot breakdown.
- α2-antiplasmin — the body's fastest-acting brake on plasmin itself.
- TAFI (thrombin activatable fibrinolysis inhibitor) — an enzyme switched on by thrombin that protects clots from premature breakdown.
- Hyperfibrinolysis — clots break down too fast, causing bleeding.
- Hypofibrinolysis — clots break down too slowly, raising clotting risk.
- Thrombolysis — the medical use of drugs to dissolve a dangerous clot.
- D-dimer — a fibrin breakdown fragment measured in blood; rises when clotting and fibrinolysis are both active.
- DIC (disseminated intravascular coagulation) — a serious condition where clotting and bleeding occur at the same time throughout the body.
- Tranexamic acid (TXA) — a drug that blocks plasminogen from binding fibrin, reducing bleeding.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Mutch, N. J., & Medcalf, R. L. (2023). The fibrinolysis renaissance. Journal of thrombosis and haemostasis : JTH, 21(12), 3304–3316. https://doi.org/10.1016/j.jtha.2023.09.012
- Risman, R. A., Kirby, N. C., Bannish, B. E., Hudson, N. E., & Tutwiler, V. (2023). Fibrinolysis: an illustrated review. Research and practice in thrombosis and haemostasis, 7(2), 100081. https://doi.org/10.1016/j.rpth.2023.100081
- Sillen, M., & Declerck, P. J. (2021). Thrombin Activatable Fibrinolysis Inhibitor (TAFI): An Updated Narrative Review. International Journal of Molecular Sciences, 22(7), 3670. https://doi.org/10.3390/ijms22073670
- Lin, J., Zuo, W., Jin, H., He, Q., Chen, S., Hu, B., & Wan, Y. (2025). Thrombolysis for acute ischaemic stroke: development and update. Brain communications, 7(3), fcaf164. https://doi.org/10.1093/braincomms/fcaf164
- Menon, B. K., Buck, B. H., Singh, N., Deschaintre, Y., Almekhlafi, M. A., Coutts, S. B., Thirunavukkarasu, S., Khosravani, H., Appireddy, R., Moreau, F., Gubitz, G., Tkach, A., Catanese, L., Dowlatshahi, D., Medvedev, G., Mandzia, J., Pikula, A., Shankar, J., Williams, H., Field, T. S., … AcT Trial Investigators (2022). Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet (London, England), 400(10347), 161–169. https://doi.org/10.1016/S0140-6736(22)01054-6
- CRASH-2 trial collaborators, Shakur, H., Roberts, I., Bautista, R., Caballero, J., Coats, T., Dewan, Y., El-Sayed, H., Gogichaishvili, T., Gupta, S., Herrera, J., Hunt, B., Iribhogbe, P., Izurieta, M., Khamis, H., Komolafe, E., Marrero, M. A., Mejía-Mantilla, J., Miranda, J., Morales, C., … Yutthakasemsunt, S. (2010). Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England), 376(9734), 23–32. https://doi.org/10.1016/S0140-6736(10)60835-5
- Chapin, J. C., & Hajjar, K. A. (2015). Fibrinolysis and the control of blood coagulation. Blood reviews, 29(1), 17–24. https://doi.org/10.1016/j.blre.2014.09.003
- Longstaff, C., & Kolev, K. (2015). Basic mechanisms and regulation of fibrinolysis. Journal of thrombosis and haemostasis : JTH, 13 Suppl 1, S98–S105. https://doi.org/10.1111/jth.12935
- Shibeko, A. M., Nikitin, N. S., Podoplelova, N. A., Manuvera, V. A., & Lazarev, V. N. (2026). Beyond Direct Fibrinolysis: Novel Approaches to Thrombolysis. Pharmaceuticals, 19(1), 10. https://doi.org/10.3390/ph19010010
- Peng, H. T., Siddiqui, M. M., Rhind, S. G., Zhang, J., da Luz, L. T., & Beckett, A. (2023). Artificial intelligence and machine learning for hemorrhagic trauma care. Military Medical Research, 10(1), 6. https://doi.org/10.1186/s40779-023-00444-0
- CRASH-3 trial collaborators (2019). Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet (London, England), 394(10210), 1713–1723. https://doi.org/10.1016/S0140-6736(19)32233-0
- Tomaselli, G. F., Mahaffey, K. W., Cuker, A., Dobesh, P. P., Doherty, J. U., Eikelboom, J. W., Florido, R., Gluckman, T. J., Hucker, W. J., Mehran, R., Messé, S. R., Perino, A. C., Rodriguez, F., Sarode, R., Siegal, D. M., & Wiggins, B. S. (2020). 2020 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology, 76(5), 594–622. https://doi.org/10.1016/j.jacc.2020.04.053
- Weitz, J. I., & Fredenburgh, J. C. (2017). Factors XI and XII as Targets for New Anticoagulants. Frontiers in medicine, 4, 19. https://doi.org/10.3389/fmed.2017.00019
- Alamowitch, S., Turc, G., Palaiodimou, L., Bivard, A., Cameron, A., De Marchis, G. M., Fromm, A., Kõrv, J., Roaldsen, M. B., Katsanos, A. H., & Tsivgoulis, G. (2023). European Stroke Organisation (ESO) expedited recommendation on tenecteplase for acute ischaemic stroke. European stroke journal, 8(1), 8–54. https://doi.org/10.1177/23969873221150022
- Campbell, B. C. V., Mitchell, P. J., Churilov, L., Yassi, N., Kleinig, T. J., Dowling, R. J., Yan, B., Bush, S. J., Dewey, H. M., Thijs, V., Scroop, R., Simpson, M., Brooks, M., Asadi, H., Wu, T. Y., Shah, D. G., Wijeratne, T., Ang, T., Miteff, F., Levi, C. R., … EXTEND-IA TNK Investigators (2018). Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. The New England journal of medicine, 378(17), 1573–1582. https://doi.org/10.1056/NEJMoa1716405