Key Takeaways
The PT/INR is a screening blood test that measures how long plasma takes to clot via the extrinsic and common pathways of the coagulation cascade, reflecting the activity of Factors I, II, V, VII, and X [7].
- PT/INR is the standard test for monitoring warfarin but is not appropriate for monitoring direct oral anticoagulants (DOACs) such as apixaban, rivaroxaban, edoxaban, or dabigatran [1].
- A prolonged PT/INR points to vitamin K deficiency, liver disease, warfarin therapy, disseminated intravascular coagulation, or a deficiency of Factor II, V, VII, or X [7].
- Sample quality matters: a 3.2% sodium citrate tube must be filled to ≥90%, with a 9:1 blood-to-citrate ratio, to avoid falsely prolonged results [2].
Introduction
The prothrombin time, almost always reported alongside the International Normalized Ratio (INR), is one of the most ordered tests in any hospital lab. It tells clinicians how quickly a patient's blood forms a clot through the extrinsic arm of the coagulation cascade. PT/INR is used to investigate unexplained bleeding, screen patients before surgery, assess liver function, and most commonly to monitor warfarin therapy [7].
This article walks through the principle, the lab protocol, and how to read the result, including the common pitfalls.
Principle of PT/INR
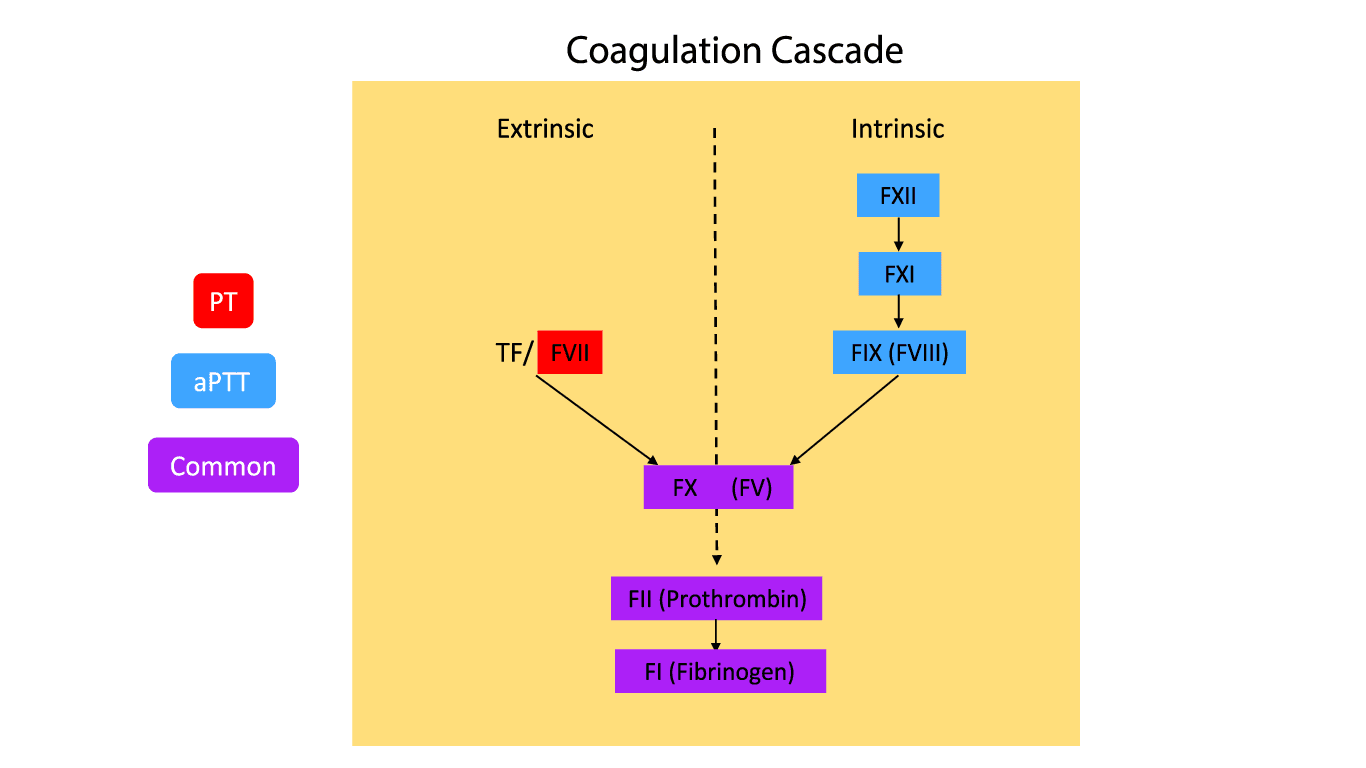
The PT/INR is built on a simple idea. Add tissue factor and calcium to platelet-poor plasma, and time how long it takes a fibrin clot to form. Tissue factor activates the extrinsic pathway, which then drives the common pathway to produce thrombin and, finally, fibrin.
In sequence:
- Tissue factor (Factor III) combines with Factor VII and calcium to form the TF–FVIIa complex.
- The TF–FVIIa complex activates Factor X directly (and Factor IX as an amplification step).
- Factor Xa, with Factor Va as a cofactor, converts prothrombin (Factor II) to thrombin.
- Thrombin cleaves fibrinogen (Factor I) to fibrin, which polymerizes into a clot.
The PT therefore probes Factors I, II, V, VII, and X. A deficiency or inhibition of any of these can prolong the result. Factor VII has the shortest half-life of the vitamin K–dependent factors, which is why warfarin prolongs the PT before it prolongs the aPTT.
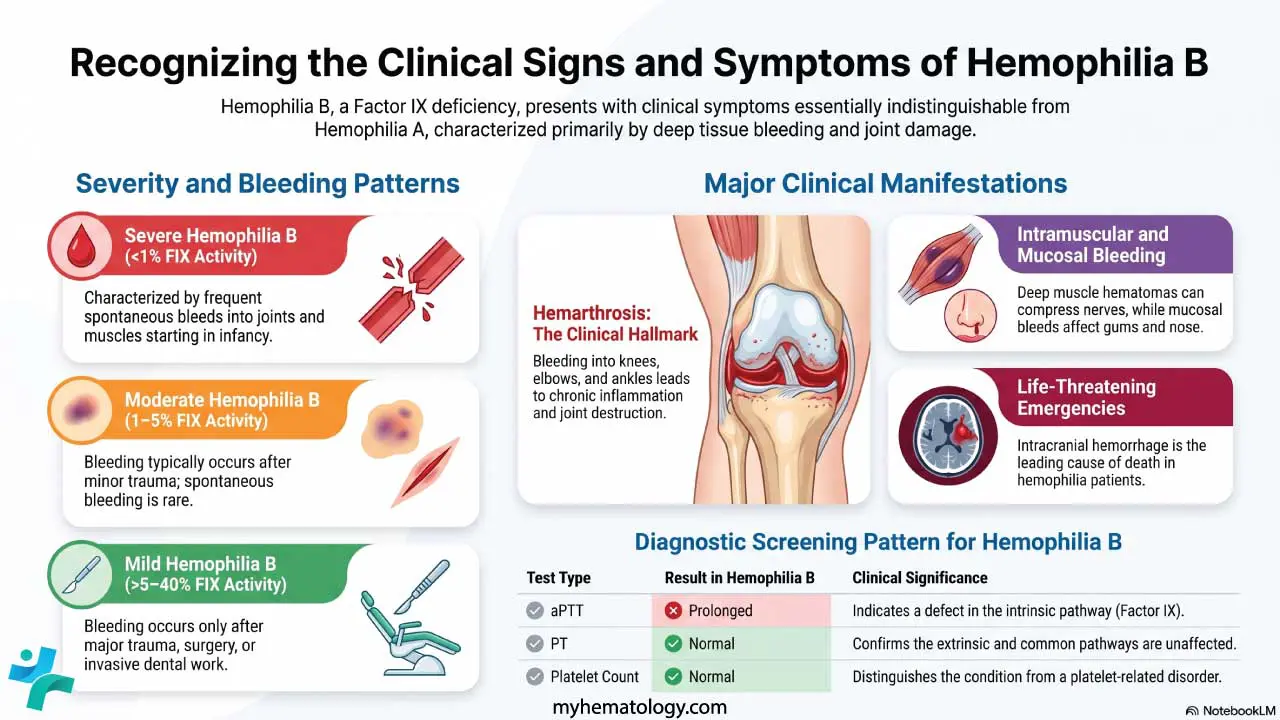
While the extrinsic complex activates Factor IX (the Josso loop), the PT assay is fundamentally insensitive to Factor IX deficiency; isolating a Factor IX defect requires an activated partial thromboplastin time (aPTT) test [9].
Materials
- #Platelet poor plasma (PPP) of patient and control. PPP is prepared by centrifuging the peripheral blood at 2000 g for 15 minutes at room temperature.
- *Thromboplastin reagent (containing tissue factor and phospholipid; rabbit-brain or recombinant human).
- *0.025 mol/L calcium chloride (CaCl2)
- *Glass tubes 5 ml
- *Water bath
- Stop watch
- Pipettes 100 - 200 uL and tips
*These items must be at 37°C.
#PPP must be kept at room temperature to prevent activation of factor VIII which may cause an inaccurate timing result.
Protocol
Method differs slightly according to the manufacturer's protocol.
The test is performed with the tubes in a 37°C water bath, removing them only briefly to check for clot formation.
- Pipette 0.1 mL of patient plasma into a labeled tube and 0.1 mL of control plasma into a second tube. Incubate for 1–3 minutes.
- Add 0.1 mL of thromboplastin to each tube. Incubate for 1–3 minutes.
- Have the stopwatch ready. Add 0.1 mL of CaCl₂ and start the timer immediately.
- Mix gently by tilting each tube to about 45° and agitating lightly.
- Briefly remove the tube from the bath at intervals to inspect for the first wisp of clot formation.
- Stop the timer at the first sign of a clot. Record the time.
- Run patient and control in duplicate and report the mean.
Some commercial kits combine thromboplastin with CaCl₂. In that case, the calcium step is built into the reagent — add the combined reagent and start the timer at that point.
| Variable | Requirement | Why It Matters |
|---|---|---|
|
Tube type
|
3.2% buffered sodium citrate (light blue top) | 3.8% citrate gives different fibrinogen and PT results [2] |
|
Fill volume
|
≥90% of tube draw volume | Underfilling alters the 9:1 blood-to-citrate ratio and falsely prolongs PT |
|
Hematocrit
|
<55% | Hct >55% reduces plasma volume relative to citrate; needs adjusted-volume tube [3] |
|
Order of draw
|
Coagulation tube after a discard tube if a butterfly is used | Avoids underfilling from line dead space |
|
Storage
|
Test within 24 h if refrigerated; avoid room-temp >4 h | Factor V and VIII degrade; FVII can activate in cold |
|
Sample integrity
|
No hemolysis, lipemia, or visible clot | All three can falsely shorten or prolong the result |
In polycythemia (hematocrit > 55%), the reduced plasma volume leaves the standard amount of liquid citrate in the tube excessive. This excess citrate over-chelates the calcium added back during the assay, artificially prolonging the clotting time. The lab must use an adjusted-volume tube, calculating the required citrate volume (C) using the CLSI formula [2]:
C=1.85×10−3×(100−Hct)×Vblood
When an unexpected prolonged PT comes back, the first move is to check the sample, not the patient.
Interpretation
| Parameter | Typical Range | Notes | |
|---|---|---|---|
| Prothrombin time (PT) | ~11–13 seconds | Reagent- and instrument-specific; each lab establishes its own | |
| INR No anticoagulant | 0.8–1.2 | Standard reference [7] | |
| INR Warfarin — most indications | 2.0–3.0 | Atrial fibrillation, VTE, bioprosthetic valves [7] | |
| INR Mechanical valve / APS | 2.5–3.5 | Higher target due to thrombotic risk [7] |
Why We Need the INR
Reference ranges vary because thromboplastin reagents differ in their sensitivity to clotting factor deficiencies. That is precisely the problem the INR was designed to solve.
Causes of a Prolonged PT/INR
- Warfarin and other vitamin K antagonists — the commonest cause in clinical practice [7].
- Vitamin K deficiency (poor intake, malabsorption, prolonged broad-spectrum antibiotics, neonates).
- Liver disease, because the liver synthesizes Factors II, V, VII, IX, and X.
- Disseminated intravascular coagulation (DIC), where clotting factors are consumed faster than they are made.
- Isolated factor deficiencies of II, V, VII, or X (rare; congenital or acquired).
- Direct factor Xa inhibitors (rivaroxaban, edoxaban) can prolong the PT, but the effect is reagent-dependent and unreliable for monitoring [1].
An isolated prolonged PT (with normal aPTT) most often points to Factor VII deficiency or early warfarin effect. A shortened PT can be seen after recombinant Factor VIIa administration.
PT/INR in Liver Disease
A cirrhotic patient with INR 1.8 is not equivalent in bleeding risk to a warfarin patient with INR 1.8. In cirrhosis, both pro- and anticoagulant proteins fall in parallel, producing a rebalanced hemostasis. The INR remains a useful prognostic marker (it is part of the MELD score), but it is not a reliable predictor of bleeding risk in chronic liver disease.
The International Normalized Ratio (INR)
Why the INR Exists
A PT measured with a sensitive recombinant human thromboplastin can be very different from one measured with a less sensitive rabbit-brain reagent, even on the same patient. Before INR was introduced, warfarin doses set in one country could be wildly off in another. The INR fixes this by mathematically correcting for reagent sensitivity.
How the INR Is Calculated
INR = (Patient PT/Mean Normal PT)ISI
- Mean Normal PT (MNPT) is the geometric mean PT of at least 20 healthy donors run on the same reagent and instrument.
- ISI (International Sensitivity Index) is a number assigned to every thromboplastin batch, calibrated against the WHO international reference. The lower the ISI, the more sensitive the reagent.
Worked example. Patient PT = 28 s. MNPT = 12 s. ISI = 1.0. INR = (28/12)1.0 = 2.33.
If the same lab switches to a less sensitive reagent with ISI = 1.4, the same plasma might give a raw PT of 22 s against an MNPT of 12 s: INR = (22/12)1.4 ≈ 2.34.
The INR stays roughly the same across reagents — which is the entire point.
Interactive INR Calculator
PT/INR Is for Warfarin, Not DOACs
Direct oral anticoagulants — apixaban, rivaroxaban, edoxaban, dabigatran — have predictable pharmacokinetics, a wide therapeutic window, and do not require routine monitoring. PT/INR is also unreliable for them [1]:
- Apixaban can produce minimal or no PT prolongation even at peak therapeutic levels.
- Rivaroxaban and edoxaban prolong the PT, but the effect is highly reagent-dependent.
- Dabigatran primarily affects thrombin time and aPTT, not PT.
When a DOAC effect genuinely needs to be measured for instance, before emergency surgery, in suspected overdose, or in massive bleeding, laboratories use drug-specific calibrated anti-Xa assays (for the Xa inhibitors) or dilute thrombin time (for dabigatran), not PT/INR [1].
In modern clinical practice, these specific assays are primarily ordered to confirm drug clearance or to guide the administration of targeted DOAC reversal agents such as andexanet alfa for apixaban and rivaroxaban, or idarucizumab for dabigatran prior to emergency surgical intervention or during life-threatening bleeding [10].
Point-of-Care INR Testing
Patients on long-term warfarin no longer have to drive to a lab every two weeks. Portable devices such as the CoaguChek measure an INR from a fingerstick capillary sample in about a minute. Two evidence-based models exist [4]:
- Patient self-testing (PST): the patient measures the INR at home and reports it to a clinician, who adjusts the dose.
- Patient self-management (PSM): the patient measures and adjusts the warfarin dose themselves, following a protocol agreed with their team.
Both improve time in therapeutic range in selected, well-trained patients. Annual clinic review and quality-control checks of the device remain important. POC INR is not used for DOACs.
Mixing Studies — What Comes Next
If a PT is prolonged and the cause is unclear, the next test is usually a 1:1 mixing study: patient plasma mixed with pooled normal plasma. If the PT corrects into the normal range, a factor deficiency is likely. If it fails to correct, an inhibitor (such as a specific factor inhibitor or, occasionally, a lupus anticoagulant) is suspected. The 2024 ICSH guidance gives detailed criteria for incubation and interpretation [3].
Symptoms of a High INR
A high INR means blood is clotting too slowly, raising the risk of bleeding. Warning signs that a warfarin patient — or their caregiver — should act on:
- Easy or unexplained bruising
- Frequent or prolonged nosebleeds
- Bleeding gums when brushing
- Heavy or prolonged menstrual bleeding
- Blood in urine (red or cola-colored) or stool (red or black, tarry)
- Prolonged bleeding from small cuts
- Vomiting blood or coffee-ground material — a medical emergency
Any of these in a patient on warfarin warrants an urgent INR check.
INR and Surgery
Bleeding risk during surgery rises sharply once INR exceeds about 1.5. As a general rule:
- INR < 1.5 — most procedures can proceed.
- INR 1.5–2.0 — case-by-case; oral or IV vitamin K may be used to bring the INR down.
- INR > 2.0 — elective surgery is usually postponed.
High-bleeding-risk procedures (neurosurgery, intraocular surgery, spinal anesthesia) generally require a tighter target than 1.5. Bridging strategies for warfarin patients undergoing surgery depend on individual thromboembolic risk and are decided in advance by the surgical and anticoagulation teams.
Frequently Asked Questions (FAQs)
What is PT/INR used for?
PT/INR screens for problems in the extrinsic and common coagulation pathways and is the standard test for monitoring warfarin therapy. It is also used to investigate bleeding disorders, assess liver function, and check clotting before surgery.
What is a normal PT/INR value?
For someone not on anticoagulants, INR is usually 0.8 to 1.2, and PT is roughly 11 to 13 seconds (lab-dependent). On warfarin, the target is usually INR 2.0 to 3.0, or 2.5 to 3.5 for a mechanical heart valve.
Can PT/INR be used to monitor DOACs?
No. Apixaban, rivaroxaban, edoxaban, and dabigatran do not require routine monitoring, and PT/INR is unreliable for measuring their effect. When measurement is genuinely needed, drug-specific anti-Xa assays or dilute thrombin time are used [1].
What can falsely prolong the PT?
Underfilled citrate tubes, hematocrit above 55%, hemolysis, prolonged transport, and contamination with heparin from an indwelling line can all falsely prolong the PT. The first response to an unexpectedly prolonged PT is usually to repeat the test on a fresh sample.
What INR is safe for surgery?
An INR below 1.5 is generally acceptable for most surgeries. Between 1.5 and 2.0, vitamin K may be used to lower it; above 2.0, elective surgery is usually postponed.
Can patients check their own INR at home?
Yes. Point-of-care devices give an INR from a fingerstick in about a minute. Patient self-testing and self-management both improve time in therapeutic range in selected, trained patients [4]. They are not used for DOACs.
Glossary of Related Medical Terms
- Coagulation cascade — the chain reaction of clotting proteins that ends in fibrin formation.
- Extrinsic pathway — the arm of the cascade triggered by tissue factor; what PT measures.
- Common pathway — the shared final steps (Factor X → thrombin → fibrin).
- Tissue factor (Factor III) — the protein released from injured tissue that initiates the extrinsic pathway.
- Thromboplastin — the lab reagent containing tissue factor and phospholipid.
- ISI (International Sensitivity Index) — a sensitivity number assigned to each thromboplastin batch; used as the exponent in the INR formula.
- INR — a standardized form of the PT result that allows comparison between labs.
- Vitamin K antagonist (VKA) — drugs (e.g., warfarin) that block vitamin K recycling, lowering active Factors II, VII, IX, and X.
- DOAC — direct oral anticoagulant (apixaban, rivaroxaban, edoxaban, dabigatran); does not require PT/INR monitoring.
- Platelet-poor plasma (PPP) — plasma centrifuged to remove platelets; the standard PT sample.
- Mean Normal PT (MNPT) — geometric mean PT of healthy donors on the same reagent and instrument.
- Mixing study — 1:1 patient-to-normal plasma mix used to distinguish factor deficiency from inhibitor.
- Time in therapeutic range (TTR) — the percentage of time a warfarin patient's INR sits within target.
- Hypoprothrombinemia — low Factor II levels, leading to bleeding tendency.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Mithoowani, S., & Siegal, D. (2024). DOACs: role of anti-Xa and drug level monitoring. Hematology. American Society of Hematology. Education Program, 2024(1), 178–185. https://doi.org/10.1182/hematology.2024000666
- Clinical and Laboratory Standards Institute. (2024). Collection, transport, and processing of blood specimens for testing plasma-based coagulation assays (6th ed., CLSI standard H21).
- Adcock, D. M., Moore, G. W., Kershaw, G. W., Montalvao, S. A. L., & Gosselin, R. C. (2024). International Council for Standardization in Haematology (ICSH) recommendations for the performance and interpretation of activated partial thromboplastin time and prothrombin time mixing tests. International journal of laboratory hematology, 46(5), 777–788. https://doi.org/10.1111/ijlh.14344
- Heneghan, C. J., Garcia-Alamino, J. M., Spencer, E. A., Ward, A. M., Perera, R., Bankhead, C., Alonso-Coello, P., Fitzmaurice, D., Mahtani, K. R., & Onakpoya, I. J. (2016). Self-monitoring and self-management of oral anticoagulation. The Cochrane database of systematic reviews, 7(7), CD003839. https://doi.org/10.1002/14651858.CD003839.pub3
- Dorgalaleh, A., Favaloro, E. J., Bahraini, M., & Rad, F. (2021). Standardization of Prothrombin Time/International Normalized Ratio (PT/INR). International journal of laboratory hematology, 43(1), 21–28. https://doi.org/10.1111/ijlh.13349
- Tripodi A. (2015). Liver Disease and Hemostatic (Dys)function. Seminars in thrombosis and hemostasis, 41(5), 462–467. https://doi.org/10.1055/s-0035-1550440
- Shikdar S, Vashisht R, Zubair M, et al. International Normalized Ratio: Assessment, Monitoring, and Clinical Implications. [Updated 2025 Feb 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507707/
- Bain BJ, Bates I, Laffan MA. Dacie and Lewis Practical Haematology: Expert Consult: Online and Print 12th Edition (Elsevier). 2016.
- Chaudhry R, Killeen RB, Babiker HM. Physiology, Coagulation Pathways. [Updated 2025 Jun 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482253/
- van Es, N., De Caterina, R., & Weitz, J. I. (2023). Reversal agents for current and forthcoming direct oral anticoagulants. European heart journal, 44(20), 1795–1806. https://doi.org/10.1093/eurheartj/ehad123