Procedure-at-a-Glance
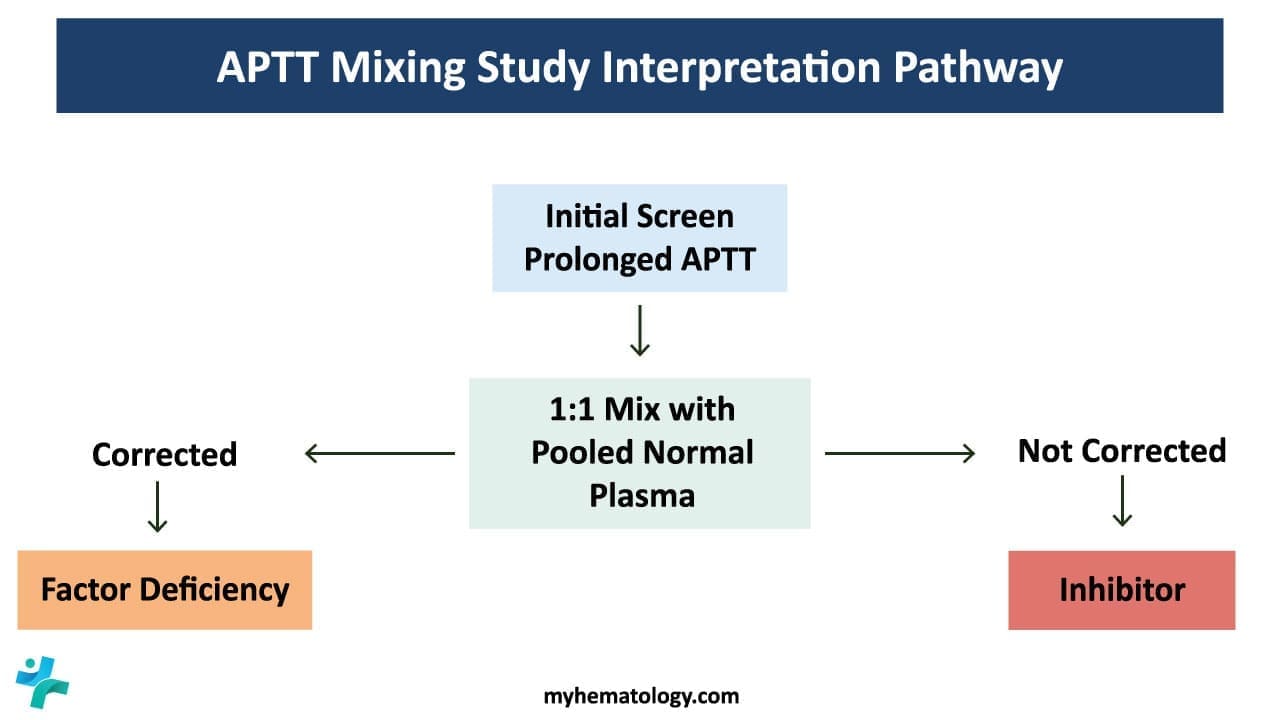
An APTT mixing study is a follow-up coagulation test that mixes patient plasma 1:1 with pooled normal plasma to find out whether a prolonged APTT is caused by a missing clotting factor or by an inhibitor [1].
- Preparation. Prepare a 1:1 mix of patient plasma (PP) and pooled normal plasma (NP).
- Immediate run. Run APTT on NP, PP and the 1:1 mix without delay.
- Incubation. Incubate the 1:1 mix and a second NP aliquot at 37°C for 1 hour (some labs use 2 hours).
- Post-incubation run. Run APTT on the incubated tubes.
- Interpret. Apply Rosner index or percent correction, compare with cutoffs.
Introduction
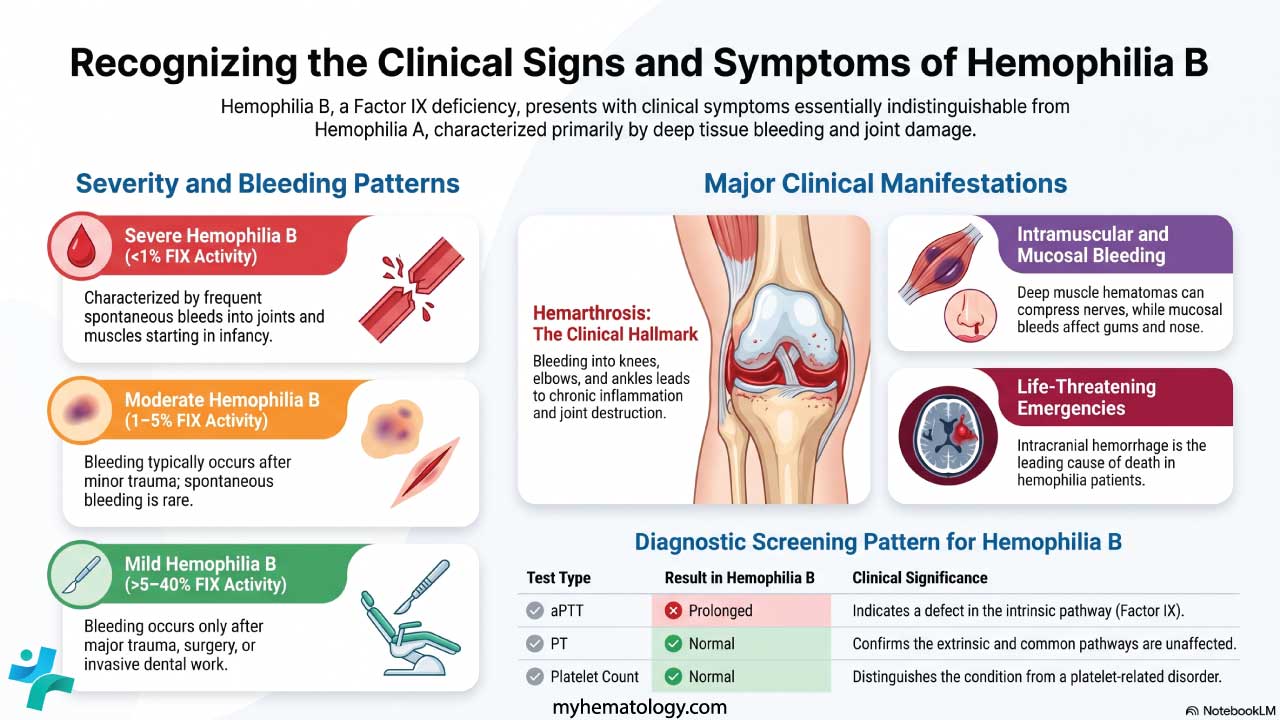
The activated partial thromboplastin time (APTT) screens the intrinsic and common pathways of clotting. When it comes back prolonged but the prothrombin time (PT) is normal, the next question is always the same: is a factor missing, or is something blocking the factors that are there? That is exactly what a mixing study answers.
A mixing study is a simple but powerful bench test. You combine patient plasma with pooled normal plasma, repeat the APTT, and watch what happens. If the clotting time falls back into the normal range, the patient is most likely deficient in a factor. If it stays long, an inhibitor is the prime suspect [1,2].
This distinction matters at the bedside. A factor deficiency, such as hemophilia A, predisposes to bleeding. A lupus anticoagulant, despite the misleading name, predisposes to clotting. Getting the interpretation right shapes whether the patient receives factor replacement, immunosuppression, or anticoagulation [2].
When to Order a Mixing Study
Run a mixing study when all three of these are true:
- The APTT is prolonged on a confirmed, properly collected sample.
- The PT is normal (so the issue is confined to the intrinsic pathway).
- Heparin and direct oral anticoagulants have been excluded as causes [1].
Skipping that third check is one of the most common errors in real labs. We will return to it under troubleshooting.
Principle of the Mixing Study
The mixing study works on a simple piece of math. Pooled normal plasma contains roughly 100% activity of every coagulation factor. Even a 50% mixture with patient plasma still supplies about 50% activity, which is enough for a normal APTT in almost all factor deficiencies [2].
So if patient plasma is just missing a factor, adding normal plasma fixes the problem. The APTT shortens. We call this correction.
If patient plasma contains an inhibitor, an antibody or antibody-like substance that blocks clotting, then the inhibitor will neutralize the factors supplied by the normal plasma too. The APTT stays long. We call this failure to correct [2].
The same principle drives every variation of the mixing study, including incubation steps and confirmatory tests for lupus anticoagulant.
Materials
- #Platelet-poor plasma (PPP) from the patient. Prepare PPP by centrifuging citrated peripheral blood at 2000 g for 15 minutes at room temperature. PPP must contain fewer than 10 × 10⁹/L platelets [1].
- Commercially available pooled normal plasma.
- Activator–phospholipid solution (pre-warmed to 37°C).
- 0.025 mol/L calcium chloride, pre-warmed to 37°C.
- Glass test tubes, 5 mL.
- 37°C water bath.
- Ice bath or crushed ice.
- Stopwatch and timer.
- Pipettes (100–200 µL) with tips.
#PPP must be kept at room temperature, not on ice, before testing. Cold activates Factor VII and accelerates Factor VIII decay, both of which distort APTT readings [5].
Protocol
Tube Preparation
Label four tubes:
- Tube 1: Normal plasma (NP)
- Tube 2: Patient plasma (PP)
- Tube 3: 1:1 immediate mix (NP + PP)
- Tube 4: 1:1 incubated mix (NP + PP)
Dispense:
- Tube 1: 0.5 mL NP
- Tube 2: 0.5 mL PP
- Tube 3: 0.25 mL NP + 0.25 mL PP
- Tube 4: 0.25 mL NP + 0.25 mL PP
APTT Measurement
Perform the APTT in duplicate on tubes 1, 2, and 3 immediately, following your standard manual APTT protocol. In brief:
- Add the activator–phospholipid solution to each tube and start the timer.
- Incubate at 37°C for 3 minutes with gentle agitation.
- Add 0.025 mol/L CaCl₂ and start the stopwatch.
- Tilt the tube to about 45° and watch for the first sign of clot formation.
- Stop the stopwatch at first clot. Record the time.
For tube 4, incubate the mixed plasma at 37°C for 1 hour (some laboratories use up to 2 hours, per ICSH 2024 guidance) [1]. After incubation, briefly cool tube 4 in an ice bath, then run the APTT as above.
The incubation step exposes time-dependent inhibitors, most importantly anti-Factor VIII antibodies in acquired hemophilia A [2].
Important Note for Prothrombin Time (PT)
While this guide focuses on the APTT, if you are concurrently performing a PT mixing study to investigate the extrinsic pathway, do not incubate the PT mix. Coagulation Factors V and VII are highly heat-labile and degrade rapidly at 37°C. Incubating a PT mix will artificially prolong the clotting time, falsely mimicking an inhibitor [1,8].
How to Interpret APTT Mixing Study
A correctly run mixing study gives you four numbers: the NP APTT, the PP APTT, the immediate mix APTT, and the incubated mix APTT. Two formulas turn those numbers into an answer.
The Rosner Index / Index of Circulating Anticoagulant (ICA)
The Rosner index is formally referred to in modern literature and standardization guidelines as the Index of Circulating Anticoagulant (ICA).
ICA= (1:1 Mix APTT−NP APTT) / PP APTT ×100
Rosner Index (ICA) Calculator
- Below 12: correction → suspect factor deficiency.
- 12 to 15: borderline → repeat or correlate clinically.
- Above 15: no correction → suspect inhibitor. The 2024 ICSH field studies formally validated this 15 cutoff for the ICA to demonstrate failure to correct [1].
Percent Correction
% Correction = (PP APTT - 1:1 Mix APTT) / (PP APTT - NP APTT) x 100
Percent Correction Calculator
- Above 70%: correction.
- Below 50%: no correction.
- 50 to 70%: borderline [1].
Advanced Interpretation: The Delta Indices
To better distinguish time-dependent Factor VIII inhibitors from complex lupus anticoagulants, modern algorithms evaluate the change between the immediate and incubated mix indices (referred to as Δ ICA or Δ percent correction). A substantial increase in the ICA after 1 to 2 hours of incubation strongly points to a time-dependent specific factor inhibitor, such as acquired hemophilia A, rather than a stable LA [1,2].
The 2024 ICSH recommendations endorse using either of these calculations followed by a subtraction step, rather than relying on visual or upper-reference-interval judgment alone [1]. A 2025 evaluation by Kamali and colleagues showed that reagent choice still strongly influences how well any mixing study cutoff performs, so each lab needs to validate its own thresholds [1].
Worked Example
A patient has these results:
- PP APTT = 65 s
- NP APTT = 30 s
- 1:1 mix APTT = 38 s
Rosner index = (38 − 30) / 65 × 100 = 12.3 (borderline)
Percent correction = (65 − 38) / (65 − 30) × 100 = 77% (correction)
The two formulas can disagree near the threshold, which is why ICSH suggests using both and then a confirmatory subtraction step.
Putting the Pattern Together
| Immediate mix | Incubated mix | Most likely cause | Clinical significance |
|---|---|---|---|
| Corrects | Corrects | Factor deficiency | Deficiency in Factor VIII, IX, XI, or XII. Normal plasma supplied the missing factor. |
| No correction | No correction | Immediate inhibitor | Most often lupus anticoagulant, or a high-titer specific inhibitor. |
| Corrects | No correction | Time-dependent inhibitor | Classic for Factor VIII inhibitor (acquired hemophilia A). The inhibitor needs warmth and time to neutralize the factor [2]. |
| No correction | Corrects | Pre-analytical artifact | Rare and usually invalid. Repeat the test. |
Differentiating Lupus Anticoagulant from a Specific Factor Inhibitor
Both a lupus anticoagulant (LA) and a specific factor inhibitor produce a non-correcting mixing study. Their clinical meaning is opposite [2,6].
Specific factor inhibitors are antibodies, usually IgG, that target a single coagulation protein such as Factor VIII. Adding more phospholipid does not help, because the antibody attacks a protein, not a lipid.
Lupus anticoagulants are heterogeneous antibodies that bind phospholipid–protein complexes. Because the APTT reagent uses phospholipid to drive the contact pathway, LA interferes with the test itself, not with a real factor.
The Paradox of Lupus Anticoagulant
- In the test tube (in vitro): LA looks like an anticoagulant. It prolongs the APTT.
- In the body (in vivo): LA is procoagulant. It is a hallmark of antiphospholipid syndrome (APS) and drives venous and arterial thrombosis and pregnancy loss [6].
Confirmatory Steps
For a non-correcting mix, the next question is which inhibitor. Two complementary tests now form the standard LA workup [6]:
- Phospholipid neutralization (APTT-PNT or hexagonal phase): Adds excess phospholipid. If the APTT shortens significantly, LA is confirmed.
- dRVVT (dilute Russell viper venom time) with screen, mix, and confirm steps.
Modern guidance treats dRVVT plus an APTT-based LA test as the diagnostic gold standard; no single assay catches all LAs [6].
For a suspected factor inhibitor, the Bethesda assay, or its more specific Nijmegen modification, quantifies inhibitor strength in Bethesda Units (BU) [7]. A titer of 5 BU or more usually classifies the patient as a "high responder" and changes treatment.
Choosing the Right Approach
Most laboratories follow a stepwise approach:
- Confirm the prolonged APTT on a fresh, well-collected sample.
- Rule out heparin (thrombin time) and DOACs (anti-Xa or specific drug levels).
- Run the 1:1 immediate and incubated mix.
- Apply Rosner index or percent correction.
- If non-corrected, proceed to LA testing or factor assays as guided by the clinical picture [1,2].
A 4:1 ratio (4 parts patient plasma to 1 part normal plasma) is more sensitive for weak inhibitors and is recommended in some ICSH algorithms [1].
Advantages of the Manual Mixing Study
- Simplicity and low cost. Few reagents, no specialized analyzer.
- Rapid turnaround. Results within an hour or two.
- Flexibility. Mixing ratios, incubation times, and add-on reagents can be adjusted to the clinical question.
Limitations
- Subjective endpoints. Manual clot detection depends on operator skill.
- Reagent sensitivity dictates utility. Not all APTT reagents are created equal. The reagent's phospholipid composition is the ultimate rate-limiting factor of the assay. If a laboratory utilizes a lupus-insensitive APTT reagent, the mixing study will inherently struggle to detect or rule out a lupus anticoagulant. Furthermore, varying reagents exhibit different sensitivities to DOACs, meaning each lab must validate its own distinct cutoffs [1,6].
- Limited sensitivity for weak inhibitors. A low-titer inhibitor can hide in a 1:1 mix.
- No single cutoff fits all reagents. Each lab must validate its own thresholds.
Troubleshooting
Pre-analytical Errors
Pre-analytical issues account for most "weird" mixing study results [5].
- Heparin contamination: Even a trace of heparin from a line flush prolongs the APTT and the 1:1 mix, mimicking an inhibitor. Confirm with a thrombin time.
- Direct oral anticoagulants (DOACs): Dabigatran, rivaroxaban, apixaban, and edoxaban can all produce a non-correcting pattern in mixing studies, behaving as nonspecific inhibitors. The effect is most pronounced near peak drug levels [4]. Always ask about DOAC use and consider drug-specific assays.
- Inadequate centrifugation: Residual platelets release Platelet Factor 4 and phospholipids that can mask LA, giving a false-negative result [1].
- Hematocrit effect: Hematocrit above 55% over-concentrates the citrate anticoagulant, falsely prolonging the APTT.
- Sample age and temperature: Factor VIII is labile. Plasma left at room temperature too long degrades, producing a falsely prolonged baseline APTT.
Frequently Asked Questions (FAQs)
What is a mixing study and when is it ordered?
A mixing study is a coagulation test that mixes a patient's plasma with pooled normal plasma, usually in a 1:1 ratio, to find out why a clotting test is prolonged. Doctors order it when a patient has an unexplained, isolated prolonged APTT. The result helps separate a clotting factor deficiency from an inhibitor, which guides bleeding versus clotting risk decisions.
How do you interpret a 1:1 mixing study result?
If the mixed plasma's APTT falls back into the normal range, the patient most likely has a factor deficiency, because the normal plasma supplied the missing factor. If the APTT stays prolonged, the patient most likely has an inhibitor that interferes with clotting even in the presence of normal factors. Modern labs confirm correction with a numerical formula such as the Rosner index or percent correction rather than visual judgment.
Why is the mixing study incubated at 37°C for one to two hours?
Some inhibitors, especially Factor VIII antibodies seen in acquired hemophilia A, are time- and temperature-dependent. They neutralize the factor slowly. Without incubation, the immediate mix may falsely appear corrected. Repeating the APTT after incubation exposes these slow-acting inhibitors.
Can blood thinners interfere with a mixing study?
Yes. Heparin and direct oral anticoagulants such as rivaroxaban, apixaban, and dabigatran can all prolong the APTT and the 1:1 mix, mimicking an inhibitor. Labs must rule these out using a thrombin time, anti-Xa assay, or specific DOAC level before reporting a mixing study as inhibitor-positive.
What is the difference between a lupus anticoagulant and a factor inhibitor in a mixing study?
Both fail to correct. The clinical meaning is opposite. A lupus anticoagulant is an antibody against phospholipid-protein complexes and is linked to thrombosis, not bleeding. A specific factor inhibitor, such as anti-Factor VIII, neutralizes a single clotting protein and causes bleeding. A phospholipid neutralization step or dRVVT helps confirm lupus anticoagulant; a Bethesda assay quantifies a factor inhibitor.
Why must Platelet-Poor Plasma be used?
Platelets contain phospholipids that can mask a lupus anticoagulant by mopping it up before testing. If centrifugation is inadequate and platelets remain in the plasma, the test can falsely correct in a patient who genuinely has an inhibitor. ICSH guidance defines PPP as plasma with fewer than 10 × 10⁹/L platelets.
Glossary of Related Medical Terms
- Activated Partial Thromboplastin Time (APTT): A blood test that measures how long plasma takes to clot through the intrinsic and common pathways of coagulation. Used to screen for factor deficiencies and inhibitors.
- Pooled Normal Plasma (PNP): Plasma combined from at least 20 healthy donors. It contains roughly 100% activity of all clotting factors and serves as the "normal" reference in a mixing study.
- Mixing study: A follow-up test in which patient plasma is mixed (usually 1:1) with pooled normal plasma to find out whether a prolonged APTT is caused by a missing factor or by an inhibitor.
- Coagulation factor: A protein in plasma that helps form a blood clot. Examples include Factors VIII, IX, XI, and XII.
- Inhibitor: An antibody, usually IgG, that blocks or destroys a coagulation factor. Inhibitors can cause severe bleeding.
- Lupus Anticoagulant (LA): An antibody that targets phospholipid-protein complexes. It prolongs clotting tests in the lab but raises clot risk in the body.
- Factor VIII Inhibitor: A specific antibody against Factor VIII. Often time- and temperature-dependent, meaning it needs warmth and time to fully inactivate the factor.
- Platelet-Poor Plasma (PPP): Plasma with a platelet count below 10 × 10⁹/L. Required for coagulation testing because residual platelets can release substances that mask LA.
- Rosner Index: A formula that gives a numerical answer to "did the mix correct?" Values below 12 suggest correction; above 15 suggest an inhibitor.
- Percent Correction: An alternative formula that expresses how much of the original APTT prolongation was rescued by adding normal plasma.
- Bethesda Assay: A quantitative test that measures inhibitor strength in Bethesda Units (BU). Used after a non-correcting mix to confirm and grade a factor inhibitor.
- Direct Oral Anticoagulant (DOAC): Modern oral blood thinners such as dabigatran, rivaroxaban, apixaban, and edoxaban. They can interfere with mixing studies by mimicking an inhibitor.
- Antiphospholipid Syndrome (APS): An autoimmune condition linked to LA and other antiphospholipid antibodies, causing both arterial and venous clots.
- Thrombin Time (TT): A clotting test that is very sensitive to heparin; used to rule out heparin contamination in samples with unexpected results.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Adcock, D. M., Moore, G. W., Kershaw, G. W., Montalvao, S. A. L., & Gosselin, R. C. (2024). International Council for Standardization in Haematology (ICSH) recommendations for the performance and interpretation of activated partial thromboplastin time and prothrombin time mixing tests. International journal of laboratory hematology, 46(5), 777–788. https://doi.org/10.1111/ijlh.14344
- Favaloro E. J. (2020). Coagulation mixing studies: Utility, algorithmic strategies and limitations for lupus anticoagulant testing or follow up of abnormal coagulation tests. American journal of hematology, 95(1), 117–128. https://doi.org/10.1002/ajh.25669
- Kershaw, G., & Orellana, D. (2013). Mixing tests: diagnostic aides in the investigation of prolonged prothrombin times and activated partial thromboplastin times. Seminars in thrombosis and hemostasis, 39(3), 283–290. https://doi.org/10.1055/s-0033-1336832
- Gosselin, R. C., Adcock, D. M., & Douxfils, J. (2019). An update on laboratory assessment for direct oral anticoagulants (DOACs). International journal of laboratory hematology, 41 Suppl 1, 33–39. https://doi.org/10.1111/ijlh.12992
- Adcock Funk, D. M., Lippi, G., & Favaloro, E. J. (2012). Quality standards for sample processing, transportation, and storage in hemostasis testing. Seminars in thrombosis and hemostasis, 38(6), 576–585. https://doi.org/10.1055/s-0032-1319768
- Devreese, K. M. J., de Groot, P. G., de Laat, B., Erkan, D., Favaloro, E. J., Mackie, I., Martinuzzo, M., Ortel, T. L., Pengo, V., Rand, J. H., Tripodi, A., Wahl, D., & Cohen, H. (2020). Guidance from the Scientific and Standardization Committee for lupus anticoagulant/antiphospholipid antibodies of the International Society on Thrombosis and Haemostasis: Update of the guidelines for lupus anticoagulant detection and interpretation. Journal of thrombosis and haemostasis : JTH, 18(11), 2828–2839. https://doi.org/10.1111/jth.15047
- Verbruggen, B., Novakova, I., Wessels, H., Boezeman, J., van den Berg, M., & Mauser-Bunschoten, E. (1995). The Nijmegen modification of the Bethesda assay for factor VIII:C inhibitors: Improved specificity and reliability. Thrombosis and Haemostasis, 73(2), 247–251. https://doi.org/10.1055/s-0038-1653759
- Kamal, A. H., Tefferi, A., & Pruthi, R. K. (2007). How to interpret and pursue an abnormal prothrombin time, activated partial thromboplastin time, and bleeding time in adults. Mayo Clinic proceedings, 82(7), 864–873. https://doi.org/10.4065/82.7.864