Key Takeaways
Lymphopenia is an abnormally low lymphocyte count in the blood, defined in adults as an absolute lymphocyte count below 1.0 x 10⁹/L (1,000 cells/µL). Thresholds are higher in children and depend on age.
- Lymphocytes ▾: Lymphocytes (B cells, T cells, and NK cells) provide the body's targeted immune defense, so a low count raises the risk of recurrent, severe, and opportunistic infections.
- Causes ▾: Lymphopenia almost always points to an underlying cause, grouped into four mechanisms: reduced production, increased destruction, redistribution, and loss.
- Symptoms ▾: The condition is often silent. When symptoms appear, they usually reflect either infections or the underlying disease, not the low count itself.
- Laboratory Investigations ▾: Diagnosis starts with a complete blood count and differential to confirm the absolute lymphocyte count, followed by targeted tests such as flow cytometry, HIV testing, and autoimmune panels.
- Treatment/Management ▾: Treatment targets the cause. Even incidentally discovered low lymphocytes deserve attention, since population studies link them to higher mortality [2][5].
*Click ▾ for more information
Introduction
Lymphopenia, also called lymphocytopenia, means there are fewer lymphocytes than normal in the circulating blood. It sounds like a narrow lab finding, but it carries real weight. Large population studies have shown that even lymphopenia found by chance, in people who feel well, is independently linked to a higher risk of infection and death [2,3,5]. That is why clinicians rarely ignore it.

In fact, incidental absolute lymphopenia (ALC < 1.0 x 10⁹/L) occurs in roughly 1.5% to 2.5% of the general adult population, though this prevalence rises to 5% to 7% in adults over 80 due to immunosenescence [9]. Furthermore, unlike neutrophil counts—where benign ethnic neutropenia is common in certain populations—normal lymphocyte baseline counts remain consistent across racial groups, meaning a low count warrants equal clinical suspicion across all demographics [5].
This article explains what lymphocytes do, how lymphopenia is defined and graded, what causes it, how it presents, and how it is investigated and managed.
What are Lymphocytes?

Lymphocytes are white blood cells that sit at the center of the immune system. Their job is specific immunity: they recognize and attack particular threats, such as a specific virus, bacterium, or cancer cell, rather than reacting to everything at once.
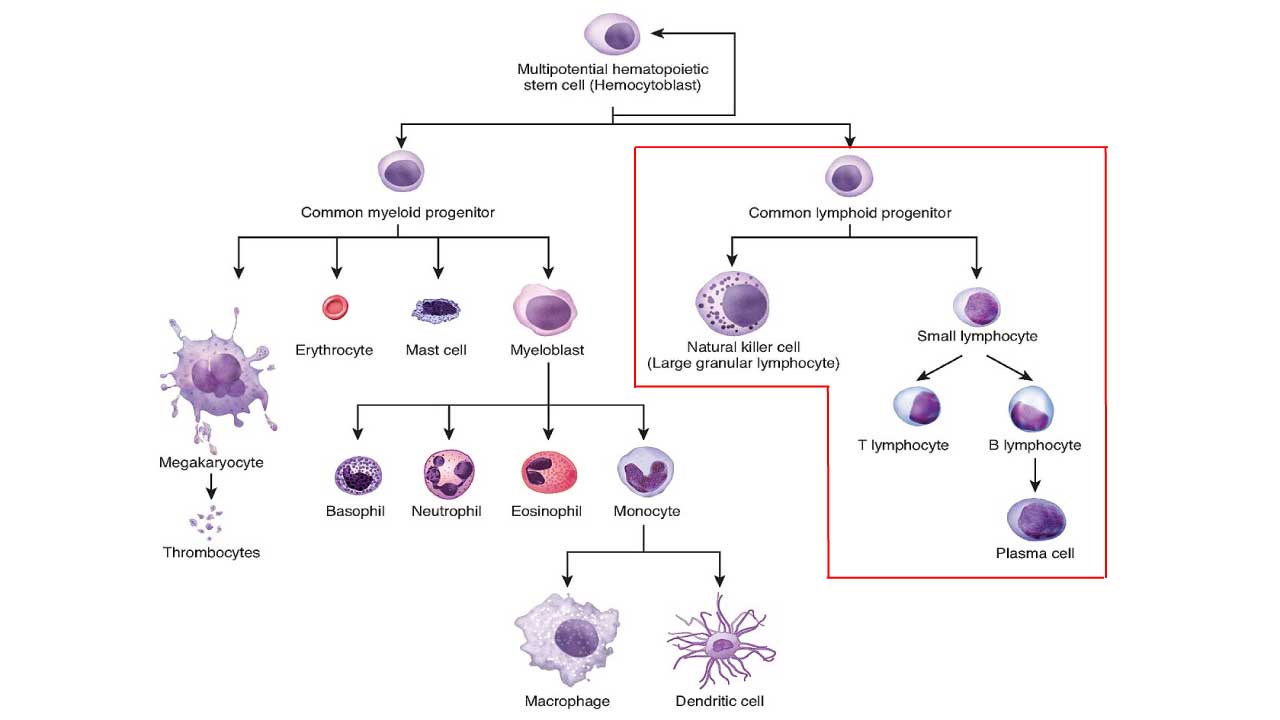
All lymphocytes start in the bone marrow from blood-forming (hematopoietic) stem cells. From there, they take different paths. Some stay in the bone marrow and mature into B lymphocytes (B cells). Others travel to the thymus, a small gland behind the breastbone, and mature into T lymphocytes (T cells). A third group, natural killer (NK) cells, belongs to the faster, non-specific arm of immunity. Once mature, these cells patrol the blood, lymph nodes, spleen, and tonsils, looking for anything foreign or abnormal.
Here is what each main type does:
- B cells drive humoral immunity, the antibody response. When a B cell meets its target antigen, it can become a plasma cell that pumps out antibodies. Those antibodies neutralize the threat or tag it for destruction.
- T cells drive cell-mediated immunity. Helper T cells (CD4+) coordinate the whole response. Cytotoxic T cells (CD8+) directly kill infected or cancerous cells. Regulatory T cells keep the system in check so it does not attack healthy tissue.
- NK cells provide immediate, non-specific defense, killing virus-infected and some tumor cells without needing prior exposure [1].
Why does this matter for lymphopenia? Because the type of lymphocyte that is low tells you a lot about the cause. A drop in CD4+ T cells points toward HIV; a broad drop across all subsets suggests a severe inherited disorder.
Innate vs. Adaptive Immunity
Immune System Basics
Minutes to hours
Days for a first response, faster on repeat
Absolute vs Relative Lymphopenia
Before diagnosing low lymphocytes, you need to know the normal range and the difference between two ways of measuring "low."
Normal Range
The "normal range" for lymphocyte counts can vary slightly between laboratories and is significantly influenced by age.
- Adults: The generally accepted normal range for an Absolute Lymphocyte Count (ALC) in adults is typically between 1.0 x 109/L to 4.8 x 109/L (or 1000 to 4800 cells/µL). Some labs might use a slightly wider or narrower range, so it's always important to refer to the specific reference range provided by the performing laboratory.
- Children: Lymphocyte counts are naturally higher in children, especially in infants and young children, and gradually decrease to adult levels as they age (exact pediatric cutoffs vary by reference source).
- Infants (<2 years): Normal absolute lymphocyte count can be as high as 3.0 x 109/L to 9.5 x 109/L (or 3000 to 9500 cells/µL).
- Children (e.g., 6 years old): The lower limit of normal might be around 1.5 x 109/L (or 1500 cells/µL).
These numbers come from a complete blood count (CBC) with differential, which reports both the percentage and the absolute number of each white blood cell type.
Absolute Lymphopenia
Absolute lymphopenia is diagnosed when the total lymphocyte count, the ALC, falls below the age-specific lower limit. For adults that is typically below 1.0 x 10⁹/L. For children it is higher and age-dependent (for example, below 3.0 x 10⁹/L under age 2). This is the clinically important form, because it reflects a true drop in circulating lymphocytes and a real rise in infection risk.
Relative Lymphopenia
Relative lymphopenia is different. Here the percentage of lymphocytes is low, but the absolute count is still normal. This usually happens because another cell type has surged and diluted the percentage.
To understand this, remember that the "differential" part of a complete blood count tells you the percentage of each white blood cell type. For example, if the total WBC count is very high (e.g., due to a significant increase in neutrophils, a condition called neutrophilia), the percentage of lymphocytes might appear low, even if the absolute lymphocyte count is normal.
Example:
A patient has a total WBC count of 20.0 x 109/L (normal: 4.0-11.0 x 109/L). His lymphocyte percentage is 10% (normal: 20-40%). His Absolute Lymphocyte Count (ALC) would be 10% of 20.0 x 109/L = 2.0 x 109/L.
In this scenario:
The ALC (2.0 x 109/L) is within the normal range for an adult (1.0-4.8 x 109/L). So, there is no absolute lymphopenia (low lymphocytes). However, the lymphocyte percentage (10%) is low compared to the normal percentage (20-40%). This indicates relative lymphopenia. So this patient has relative, not absolute, lymphopenia, usually driven by a spike in neutrophils from a bacterial infection or stress.
For judging immune risk
Always use the absolute count, not the percentage.
Causes of Lymphopenia
A low lymphocyte count is rarely the disease itself. It is a clue. The most useful way to organize the long list of causes is by mechanism: is the body making too few, destroying too many, moving them out of the blood, or losing them altogether? Hold those four buckets in mind and the rest becomes manageable.
Decreased Production of Lymphocytes (Bone Marrow Suppression/Failure)
Here the bone marrow cannot make enough lymphocytes.

- Bone marrow disorders: aplastic anemia, myelodysplastic syndromes (MDS), leukemias, lymphomas, and inherited bone marrow failure. Lymphopenia is common in MDS and carries independent prognostic weight in lower-risk patients [4].
- Medical treatments: traditional chemotherapy and radiation kill dividing lymphocyte precursors. Notably, modern cellular therapies such as CAR-T cell therapy and bispecific T-cell engagers (BiTEs) rely on aggressive "lymphodepleting chemotherapy" (e.g., fludarabine and cyclophosphamide) prior to infusion. This intentionally induces profound, prolonged lymphopenia to create immune space for the engineered cells [10]. Non-steroid immunosuppressants (azathioprine, methotrexate, cyclosporine) also suppress production.
- Congenital immunodeficiencies: genetic disorders present from birth. Severe combined immunodeficiency (SCID) causes very low T and B cell function. DiGeorge syndrome (22q11.2 deletion) underdevelops the thymus, cutting T cells. Wiskott-Aldrich syndrome and ataxia-telangiectasia also impair lymphocytes, and some patients with common variable immunodeficiency (CVID) have low B cells.
- Nutritional deficiencies: severe protein-energy malnutrition is one of the most common causes of weakened immunity worldwide. Shortages of zinc, vitamin B12, and folate also impair lymphocyte development.
- Chronic disease: end-stage kidney disease can lower counts, partly through uremic toxins.
Increased Destruction or Apoptosis of Lymphocytes
Here lymphocytes are made but then destroyed or pushed into programmed cell death (apoptosis).
- Viral infections are a major group, and the mechanism is well studied [6]. HIV directly infects and destroys CD4+ T cells. Influenza causes acute, usually temporary lymphopenia. Measles can cause deep and prolonged drops. Hepatitis B and C and, in some phases, EBV also contribute. Lymphopenia is a general marker of viral pneumonia severity, not something unique to one virus. In COVID-19 it tracks closely with how sick a patient becomes, but the same pattern is seen in influenza [6]. Beyond acute infection, persistent mild-to-moderate lymphopenia and chronic T-cell exhaustion are increasingly recognized as ongoing biomarkers in a subset of patients experiencing Post-Acute Sequelae of SARS-CoV-2 (Long COVID) [11].
- Bacterial infections: sepsis triggers massive lymphocyte apoptosis and redistribution. Persistent lymphopenia in sepsis is now recognized as a sign of immune exhaustion and worse outcomes [7]. Miliary tuberculosis is another cause.
- Autoimmune disease: in systemic lupus erythematosus (SLE), lymphopenia is so common it is part of the diagnostic criteria. Rheumatoid arthritis, myasthenia gravis, and Sjögren's syndrome can also lower counts.
- Medications: corticosteroids are a very common cause, acting by both apoptosis and redistribution. Some biologics (alemtuzumab, rituximab, anti-thymocyte globulin) deplete lymphocytes by design.
Redistribution of Lymphocytes
Here the count drops not because cells are gone, but because they have temporarily left the bloodstream for lymphoid tissue.
- Acute stress from trauma, major surgery, burns, or critical illness raises cortisol and shifts lymphocytes out of circulation.
- Corticosteroids do this too, on top of their destructive effect.
- Anaphylaxis can cause a brief redistribution.
Loss of Lymphocytes
Here lymphocytes physically leave the body.
- Protein-losing enteropathy: conditions like severe Crohn's disease, ulcerative colitis, or intestinal lymphangiectasia leak lymphocytes through the gut.
- Chylothorax or chylous ascites: lymph fluid rich in lymphocytes leaks into the chest or abdomen.
When No Cause Is Found: Idiopathic CD4 Lymphocytopenia
Sometimes a thorough workup finds nothing. When CD4+ T cells stay low without explanation, the diagnosis is idiopathic CD4 lymphocytopenia (ICL), a diagnosis of exclusion.
Its formal criteria are worth memorizing: a CD4 count below 300 cells/µL, or CD4 cells making up less than 20% of total T cells, confirmed on more than one occasion, with HIV and other known causes ruled out [8]. However, as Next-Generation Sequencing (NGS) and Whole Exome Sequencing (WES) become standard practice in immunology, the "idiopathic" label is shrinking. Many patients previously diagnosed with ICL are now found to have subtle, late-onset inborn errors of immunity, such as inherited genetic CD4 deficiencies [12,13].
ICL tends to persist; in cohort studies most patients keep low CD4 counts for years and only a minority normalize, with very low initial CD4 or NK counts predicting worse outcomes.

Signs and Symptoms
Lymphopenia is usually silent. When it does cause problems, the symptoms come from one of two places: a weakened immune system, or the underlying disease driving the low count.
From the Weakened Immune System
A low lymphocyte count, especially if severe or prolonged, blunts the body's defenses. The clearest consequence is increased susceptibility to infection, which can show up as:
- Recurrent or unusually severe infections.
- Opportunistic infections that rarely trouble healthy people, such as Pneumocystis jirovecii pneumonia, cytomegalovirus (CMV), atypical mycobacteria, and invasive fungal infections.
- Specific patterns: recurrent herpes simplex or shingles, oral thrush or invasive fungal disease, and stubborn skin or atypical chest infections.
In infants with severe congenital lymphopenia such as SCID, repeated infections can cause failure to thrive. Over the long term, because lymphocytes also police the body for abnormal cells, chronic severe lymphopenia can raise the risk of certain cancers, including some lymphomas and virus-associated tumors.
From the Underlying Cause
Often the patient's actual complaints come from the primary illness, which is why a careful history and exam matter so much:
- Chronic infection or malignancy: fatigue, weight loss, fever, night sweats, malaise.
- Autoimmune disease: joint pain and swelling, the butterfly (malar) rash of SLE, hair loss, dry eyes and mouth in Sjögren's.
- Active infection: cough and breathlessness, diarrhea, skin lesions, swollen lymph nodes or an enlarged spleen.
- Drug-induced cases: often no symptoms at all, found by chance on routine bloods.
- Congenital cases in children: severe infections from early life, chronic diarrhea, poor growth, eczema, and sometimes distinctive facial features or developmental delay.
Laboratory Investigations
Testing has three goals: confirm the low count, judge its severity, and find the cause. The workup moves from simple to specialized, guided by clinical clues.
First-Line Tests
The complete blood count (CBC) with differential is the foundation. It gives the absolute lymphocyte count that confirms the diagnosis and shows whether other cell lines are also low, which would suggest a marrow-wide problem. A high neutrophil count with a low lymphocyte percentage points toward relative lymphopenia.
A peripheral blood smear lets a trained eye check lymphocyte appearance. Atypical lymphocytes suggest viral infections such as EBV or CMV; immature cells (blasts) or abnormal forms can flag a marrow disorder or malignancy.
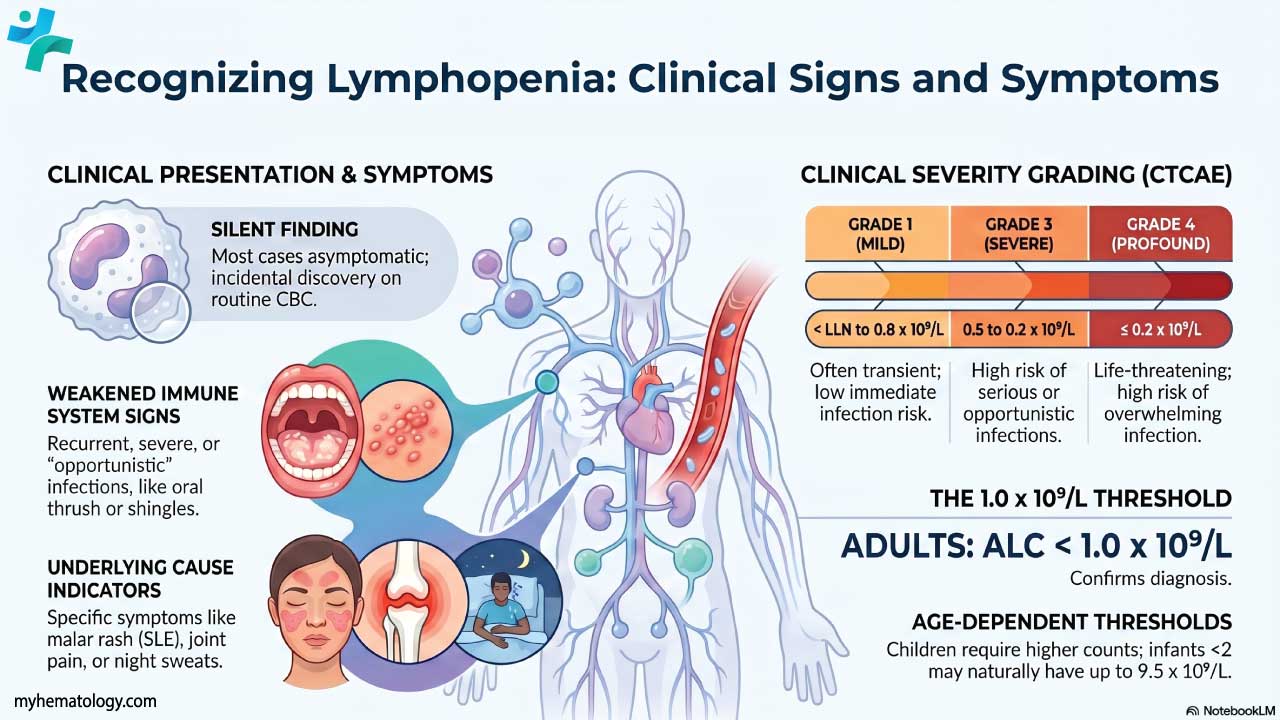
Assessing Severity: CTCAE Grading
Clinicians often grade severity using the Common Terminology Criteria for Adverse Events (CTCAE), especially in cancer care.
| Grade | Absolute Lymphocyte Count | Clinical Significance |
|---|---|---|
|
Grade 1
Mild
|
< LLN to 0.8 × 10⁹/L | Often incidental or transient. Low immediate infection risk. |
|
Grade 2
Moderate
|
0.8 to 0.5 × 10⁹/L | Watch for infection; may prompt a cause workup. |
|
Grade 3
Severe
|
0.5 to 0.2 × 10⁹/L | Real risk of serious or opportunistic infection; may need drug dose changes and preventive antimicrobials. |
|
Grade 4
Life-Threatening
|
≤ 0.2 × 10⁹/L | Profound lymphopenia. High risk of overwhelming infection; needs urgent management. |
|
Grade 5
Death
|
Death | Death related to the lymphopenia, typically via infection. |
Targeted Tests Based on Suspicion
Once lymphopenia is confirmed, the next tests follow the clinical picture:
- Flow cytometry (lymphocyte subsets) counts CD4+ and CD8+ T cells, B cells, and NK cells. This pinpoints which population is low, for example isolated CD4 loss in HIV or a broad deficit in SCID.
- Immunoglobulin levels (IgG, IgA, IgM) check B cell output; low levels suggest conditions like CVID.
- Vaccine titers and proliferation assays test whether the immune cells actually work, not just whether they are present.
- Infection screening: HIV testing is essential given its classic link to CD4 loss. Viral serologies (CMV, EBV, hepatitis, SARS-CoV-2), TB testing, and cultures follow as indicated.
- Autoimmune markers: ANA as a screen, then specific antibodies (anti-dsDNA, anti-Sm for SLE; anti-Ro/La for Sjögren's; RF and anti-CCP for rheumatoid arthritis).
- Bone marrow aspiration and biopsy when a primary marrow disorder is suspected.
- Imaging (chest and abdominal CT) for thymic abnormalities, opportunistic infection, or malignancy.
- Genetic testing for suspected congenital immunodeficiencies.
- Medication review. Not a lab test, but often the fastest route to a diagnosis.
- Next-Generation Genetic Sequencing (NGS) is increasingly utilized in adults with unexplained, severe, or persistent lymphopenia to rule out late-onset inborn errors of immunity before settling on a diagnosis of idiopathic CD4 lymphocytopenia [12].
Treatment and Management of Lymphopenia
Management rests on two pillars: fix the cause, and protect the patient while the count is low. Which pillar dominates depends on severity.
Treat the Underlying Cause
This is the heart of management, because correcting the root problem usually corrects the count.
- Adjust offending drugs. If steroids are responsible, a gradual taper may help, weighed against why the steroid was needed. Chemotherapy and immunosuppressant doses may be modified by the treating specialist. Lymphocyte-depleting biologics require monitoring and prevention.
- Treat infections. Antiretroviral therapy can substantially restore CD4 counts in HIV. Treating sepsis or specific viral and fungal infections resolves infection-driven lymphopenia.
- Control autoimmune disease. Bringing conditions like SLE under control often lifts the count.
- Treat malignancy and correct nutrition. Cancer-directed therapy and reversal of malnutrition or micronutrient deficiencies both help restore lymphocyte production.
Protect the Patient (Supportive Care)
When immune risk is high, these measures reduce harm:
- Preventive antimicrobials. Antivirals (such as acyclovir) for high-risk patients, and trimethoprim-sulfamethoxazole to prevent Pneumocystis pneumonia in severe T cell deficiency.
- Immunoglobulin replacement (IVIG or SCIG) when low antibody levels accompany recurrent bacterial infections. Note: this supplies antibodies, it does not raise the lymphocyte count.
- A note on G-CSF: it raises neutrophils, not lymphocytes, so it is not a treatment for lymphopenia itself.
- Vaccination, carefully. Killed or inactivated vaccines are generally safe and encouraged. Live attenuated vaccines (MMR, varicella, rotavirus, live flu) are generally avoided in severe lymphopenia because of infection risk, a decision best left to a specialist.
- Everyday infection control. Hand hygiene, avoiding sick contacts and crowds, masking in risky settings, and food precautions for the most vulnerable.
For Severe Cases
- Hematopoietic stem cell transplantation (HSCT) is the definitive treatment for severe inherited immunodeficiencies like SCID and for some marrow failures.
- Gene therapy aims to correct the underlying genetic defect and has succeeded in certain SCID types, though it remains specialized.
- Thymic transplantation can restore T cell development in severe thymic aplasia, such as complete DiGeorge syndrome.
Monitoring
Recovery is tracked with serial CBCs, repeat lymphocyte subset analysis where relevant (especially CD4 counts in HIV or after transplant), and close clinical watch for new infections.

Frequently Asked Questions (FAQ)
What is lymphopenia, and at what number is it diagnosed?
Lymphopenia means an abnormally low number of lymphocytes, the white blood cells that run your targeted immune defense. In adults it is usually defined as an absolute lymphocyte count below 1.0 x 10⁹/L (1,000 cells per microliter). The threshold is higher in children and varies by age, so results are always read against age-specific reference ranges.
Is lymphopenia dangerous?
It depends on how low the count is and why. Mild or temporary lymphopenia, such as after a viral infection or a course of steroids, often resolves on its own. Severe or persistent lymphopenia is more serious because it leaves the body open to recurrent and opportunistic infections, and large population studies have linked even incidentally found lymphopenia to higher overall mortality. The underlying cause matters more than the number alone.
What causes a low lymphocyte count?
Causes fall into four mechanisms: reduced production (bone marrow disease, chemotherapy, congenital immune disorders), increased destruction (HIV, severe COVID-19, autoimmune disease, certain drugs), redistribution out of the bloodstream (acute stress, steroids), and loss from the body (some gut diseases, lymphatic leaks). Identifying which mechanism is at play guides the workup.
How is the cause of lymphopenia found?
The first step is a complete blood count with differential to confirm the low absolute lymphocyte count. From there, testing is guided by clinical clues and may include flow cytometry to identify which lymphocyte subset is low, HIV testing, autoimmune antibody panels, immunoglobulin levels, and sometimes a bone marrow biopsy or genetic testing.
Can stress, poor sleep, intense exercise, or not eating enough lower my lymphocytes?
Yes, but usually only mildly and temporarily. Physical or psychological stress, sleep deprivation, and prolonged intense exercise can all shift lymphocytes out of the bloodstream for a short period. Severe or long-term malnutrition is different: it genuinely impairs lymphocyte production and is one of the most common causes of weakened immunity worldwide.
Can lymphopenia be treated?
Treatment targets the cause rather than the number. Stopping or adjusting a triggering drug, treating an infection such as HIV with antiretroviral therapy, or controlling an autoimmune disease often restores the count. When the immune risk is high, doctors add protective measures like preventive antibiotics or antibody (immunoglobulin) replacement. Severe inherited cases may need a stem cell transplant or gene therapy.
Glossary of Related Medical Terms
- Lymphocyte: A type of white blood cell that drives targeted immune defense. The main types are B cells, T cells, and natural killer (NK) cells.
- Lymphopenia (lymphocytopenia): An abnormally low number of lymphocytes in the blood. In adults, usually an absolute count below 1.0 x 10⁹/L.
- Absolute Lymphocyte Count (ALC): The actual number of lymphocytes per liter (or microliter) of blood, as opposed to their percentage. The number that matters most clinically.
- Apoptosis: Programmed cell death; a controlled "self-destruct" process cells use, which can be triggered abnormally in some causes of lymphopenia.
- Humoral immunity: Defense carried out by antibodies, which are made by B cells.
- Cell-mediated immunity: Defense carried out directly by T cells rather than by antibodies.
- CD4+ T cell (helper T cell): A T cell that coordinates the immune response. The cell HIV targets.
- CD8+ T cell (cytotoxic T cell): A T cell that directly kills infected or cancerous cells.
- Flow cytometry / lymphocyte subset analysis: A lab test that counts specific lymphocyte populations (CD4, CD8, B cells, NK cells) to find which type is deficient.
- Hypogammaglobulinemia: Low blood levels of antibodies (immunoglobulins), often a sign of poor B cell function.
- Opportunistic infection: An infection caused by an organism that usually does not cause disease in people with healthy immune systems.
- Idiopathic CD4 lymphocytopenia (ICL): Persistently low CD4 T cells with no identifiable cause and no HIV infection; a diagnosis of exclusion.
- CTCAE: Common Terminology Criteria for Adverse Events, a standardized system (Grades 1–5) used to rate the severity of lab abnormalities like lymphopenia.
- Prophylactic antimicrobials: Medicines given to prevent infection before it occurs, used in people at high risk.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Janeway CA Jr, Travers P, Walport M, et al. Immunobiology: The Immune System in Health and Disease. 5th edition. New York: Garland Science; 2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK10757/
- Warny, M., Helby, J., Nordestgaard, B. G., Birgens, H., & Bojesen, S. E. (2020). Incidental lymphopenia and mortality: a prospective cohort study. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 192(2), E25–E33. https://doi.org/10.1503/cmaj.191024
- Warny, M., Helby, J., Nordestgaard, B. G., Birgens, H., & Bojesen, S. E. (2018). Lymphopenia and risk of infection and infection-related death in 98,344 individuals from a prospective Danish population-based study. PLoS medicine, 15(11), e1002685. https://doi.org/10.1371/journal.pmed.1002685
- Silzle, T., Blum, S., Schuler, E., Kaivers, J., Rudelius, M., Hildebrandt, B., Gattermann, N., Haas, R., & Germing, U. (2019). Lymphopenia at diagnosis is highly prevalent in myelodysplastic syndromes and has an independent negative prognostic value in IPSS-R-low-risk patients. Blood cancer journal, 9(8), 63. https://doi.org/10.1038/s41408-019-0223-7
- Zidar, D. A., Al-Kindi, S. G., Liu, Y., Krieger, N. I., Perzynski, A. T., Osnard, M., Nmai, C., Anthony, D. D., Lederman, M. M., Freeman, M. L., Bonomo, R. A., Simon, D. I., & Dalton, J. E. (2019). Association of Lymphopenia With Risk of Mortality Among Adults in the US General Population. JAMA network open, 2(12), e1916526. https://doi.org/10.1001/jamanetworkopen.2019.16526
- Guo, Z., Zhang, Z., Prajapati, M., & Li, Y. (2021). Lymphopenia Caused by Virus Infections and the Mechanisms Beyond. Viruses, 13(9), 1876. https://doi.org/10.3390/v13091876
- Wang, Z., Zhang, W., Chen, L., Lu, X., & Tu, Y. (2024). Lymphopenia in sepsis: a narrative review. Critical care (London, England), 28(1), 315. https://doi.org/10.1186/s13054-024-05099-4
- Yarmohammadi, H., & Cunningham-Rundles, C. (2017). Idiopathic CD4 lymphocytopenia: Pathogenesis, etiologies, clinical presentations and treatment strategies. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology, 119(4), 374–378. https://doi.org/10.1016/j.anai.2017.07.021
- Valiathan, R., Ashman, M., & Asthana, D. (2016). Effects of Ageing on the Immune System: Infants to Elderly. Scandinavian journal of immunology, 83(4), 255–266. https://doi.org/10.1111/sji.12413
- Hirayama, A. V., Gauthier, J., Hay, K. A., Voutsinas, J. M., Wu, Q., Gooley, T., Li, D., Cherian, S., Chen, X., Pender, B. S., Hawkins, R. M., Vakil, A., Steinmetz, R. N., Acharya, U. H., Cassaday, R. D., Chapuis, A. G., Dhawale, T. M., Hendrie, P. C., Kiem, H. P., Lynch, R. C., … Turtle, C. J. (2019). The response to lymphodepletion impacts PFS in patients with aggressive non-Hodgkin lymphoma treated with CD19 CAR T cells. Blood, 133(17), 1876–1887. https://doi.org/10.1182/blood-2018-11-887067
- Phetsouphanh, C., Darley, D. R., Wilson, D. B., Howe, A., Munier, C. M. L., Patel, S. K., Juno, J. A., Burrell, L. M., Kent, S. J., Dore, G. J., Kelleher, A. D., & Matthews, G. V. (2022). Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nature immunology, 23(2), 210–216. https://doi.org/10.1038/s41590-021-01113-x
- Guérin, A., Moncada-Vélez, M., Jackson, K., Ogishi, M., Rosain, J., Mancini, M., Langlais, D., Nunez, A., Webster, S., Goyette, J., Khan, T., Marr, N., Avery, D. T., Rao, G., Waterboer, T., Michels, B., Neves, E., Iracema Morais, C., London, J., Mestrallet, S., … Tangye, S. G. (2024). Helper T cell immunity in humans with inherited CD4 deficiency. The Journal of experimental medicine, 221(5), e20231044. https://doi.org/10.1084/jem.20231044
- Routy, J. P., & Isnard, S. (2021). Beyond the Absence of CD4 T-Cell Count: A Novel Genetic CD4 T-Cell Deficiency Disorder With a Contingency Plan. The Journal of infectious diseases, 223(4), 547–549. https://doi.org/10.1093/infdis/jiab026