Procedure At a Glance
The indirect antiglobulin test (IAT), also called the indirect Coombs test, detects free IgG antibodies in plasma that could bind red blood cells [1,3].
- Spin the patient sample to obtain clear serum or plasma.
- Prepare reagent red cells at a 3–5% suspension in saline (or LISS, depending on method).
- Mix patient serum with the red cell suspension.
- Incubate at 37°C — 10–15 minutes with LISS, 15 minutes with PEG, 30–60 minutes with saline alone.
- Wash three to four times with saline. This step is the single most common cause of false results.
- Add AHG (Coombs reagent) — anti-IgG (monospecific) is preferred for routine screening; polyspecific (anti-IgG + anti-C3d) is used in specific situations.
- Centrifuge briefly, then gently resuspend the cell button.
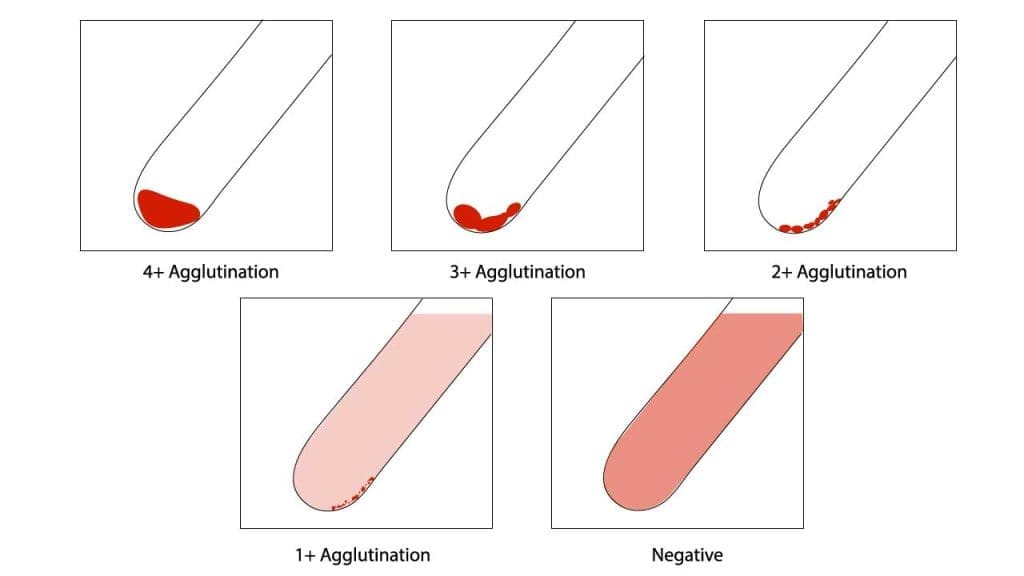
- Read: agglutination or hemolysis at this step is a positive result. Grade 0 to 4+.
- Add Coombs control cells (CCC) to every negative tube. They must agglutinate; if not, the test is invalid and must be repeated.
Introduction
A blood transfusion only works if the donor red cells survive in the recipient. The indirect antiglobulin test, or IAT, is the lab test that protects that survival. It looks for antibodies in the patient's plasma that would attack donor red cells before they are ever transfused [1,3].
The IAT also matters for pregnancy. If a mother carries antibodies against a baby's red cell antigens, those antibodies can cross the placenta and cause HDFN. The same test that protects transfusion recipients also screens every pregnancy for this risk [2,3].
This article walks through the principle, materials, and protocol of the IAT, then explains how to interpret results, why false reactions occur, and what to do about modern drug interference such as daratumumab.
Why the IAT sits at the center of immunohematology
The IAT underpins four routine blood-bank tasks [1,2]:
- Antibody screening — checking a patient's plasma against reagent red cells for any clinically significant antibodies.
- Antibody identification — using a panel of red cells with known antigen profiles to name the specific antibody.
- Crossmatching — confirming a chosen donor unit is compatible.
- Antigen typing for some blood group systems where direct typing is unreliable.
Principle of Indirect Coombs Test (IAT)
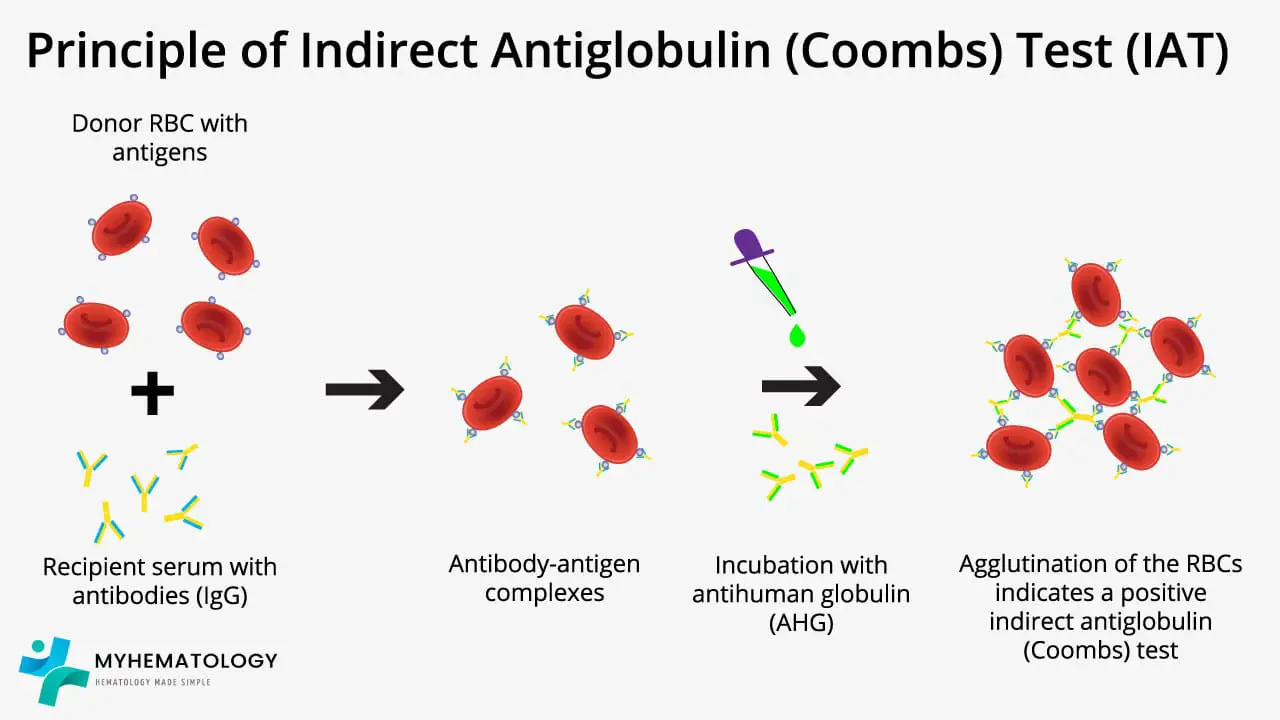
The IAT detects IgG antibodies that bind red cells but cannot, by themselves, cause visible clumping [3].
Here is why a bridge is needed. IgG molecules are small and red cells repel each other through surface negative charge, creating an electrostatic repulsion known as the zeta potential [1]. Even when many IgG molecules coat a red cell, two coated cells stay far enough apart that no agglutination is seen. The cell is "sensitized" but invisibly so [1,3].
AHG fixes that. AHG is an antibody (raised in animals or produced as a monoclonal) that targets human IgG. When added to sensitized red cells, each AHG molecule grabs the IgG on one cell with one arm and the IgG on a neighboring cell with the other. That cross-link bridges the gap and produces visible agglutination — the "positive" you read at the bench [1,3].
The IAT is built around this bridge. Patient serum is incubated with reagent red cells; any matching antibodies bind during incubation. The cells are washed to remove unbound proteins, AHG is added, and agglutination reveals the antibody [1].
Practical points
First, the IAT is optimized for IgG. IgM antibodies are large enough to agglutinate red cells without AHG and are usually detected at earlier reading phases, not at the AHG phase [1,3]. Second, reagent screening cells are commercial group O cells with a defined antigen profile and are not "universal donor" units. The group O choice removes ABO interference so antibodies to other blood groups are not masked.
Materials
- Patient serum or plasma
- Normal saline (0.9% NaCl) or low ionic strength solution (LISS)
- Reagent red cells, 3–5% suspension in saline or LISS
- For compatibility testing: commercial reagent screening cells (typically two- or three-cell sets) or donor red cells for crossmatch
- For autoimmune hemolytic anemia (AIHA) workup: the patient's own washed red cells
- Antihuman globulin (AHG):
- Anti-IgG (monospecific) — preferred for routine screening; avoids clinically insignificant complement reactions
- Polyspecific (anti-IgG + anti-C3d) — used in specific workups
- Coombs control cells (CCC) — IgG-coated reagent red cells (commonly anti-D coated D-positive cells)
- Test tubes, calibrated pipettes, serofuge
- Optional enhancers: 22% bovine albumin or PEG (legacy or specialized use)
Protocol (Tube Method)
This is the classic tube method. Most modern labs run column agglutination (gel) or solid-phase as their routine method, but the tube principle still matters because it makes every step explicit [1,2].
- Centrifuge the patient sample and collect clear serum or plasma.
- If using the patient's own red cells (AIHA workup), wash 5 mL of red cells with saline three times, then resuspend to 3–5% in saline.
- For each reagent cell to be tested, label one tube. Add two drops of patient serum and one drop of the 3–5% reagent red cell suspension.
- If using LISS: add the appropriate volume of LISS additive per manufacturer instructions (typically equal to the serum volume), then incubate at 37°C for 10–15 minutes [1]. If using saline only: incubate at 37°C for 30–60 minutes. If using PEG: add the appropriate volume of PEG (typically equal to the serum volume), incubate at 37°C for 15 minutes, and skip a 37°C reading. Do not centrifuge PEG tubes after the 37°C incubation and before washing, as PEG can cause nonspecific aggregation that mimics true agglutination [1].
- After incubation, wash the cells with saline three to four times. Decant the supernatant completely after the last wash, leaving only the cell button. Inadequate washing is the leading technical cause of incorrect results [1].
- Add two drops of AHG to the cell button. Tilt to mix thoroughly.
- Centrifuge briefly (15–30 seconds at ~1000 × g, or per manufacturer instructions).
- Gently resuspend the cell button and read macroscopically. Grade agglutination 0 to 4+. Hemolysis at this stage also counts as a positive reaction — some antibodies (for example anti-Jkᵃ) destroy cells rather than clump them [1].
- For every tube that reads negative, add Coombs control cells (CCC) and re-centrifuge. CCC must agglutinate. If they do not, the test is invalid, usually because AHG was missed, was inactive, or was neutralized by inadequate washing [1].
Interpretation
| Result | Interpretation |
|---|---|
| Agglutination or hemolysis at AHG phase (positive) | Antibody against the corresponding red cell antigen is present |
| Negative AHG, valid CCC | No detectable antibody against the tested cells |
| Negative AHG, negative CCC | Test invalid — repeat |
| Pan-reactive (positive with all reagent cells) | Consider autoantibody, drug interference (e.g., daratumumab), or rouleaux |
Function of Coombs Control Cells (CCC)
CCC are reagent red cells already coated with IgG. They confirm two things: that the AHG was added and active, and that washing was adequate enough to leave the AHG free to react. A negative AHG result without a positive CCC tells you nothing because the negative could just mean the AHG never had a chance to work [1].
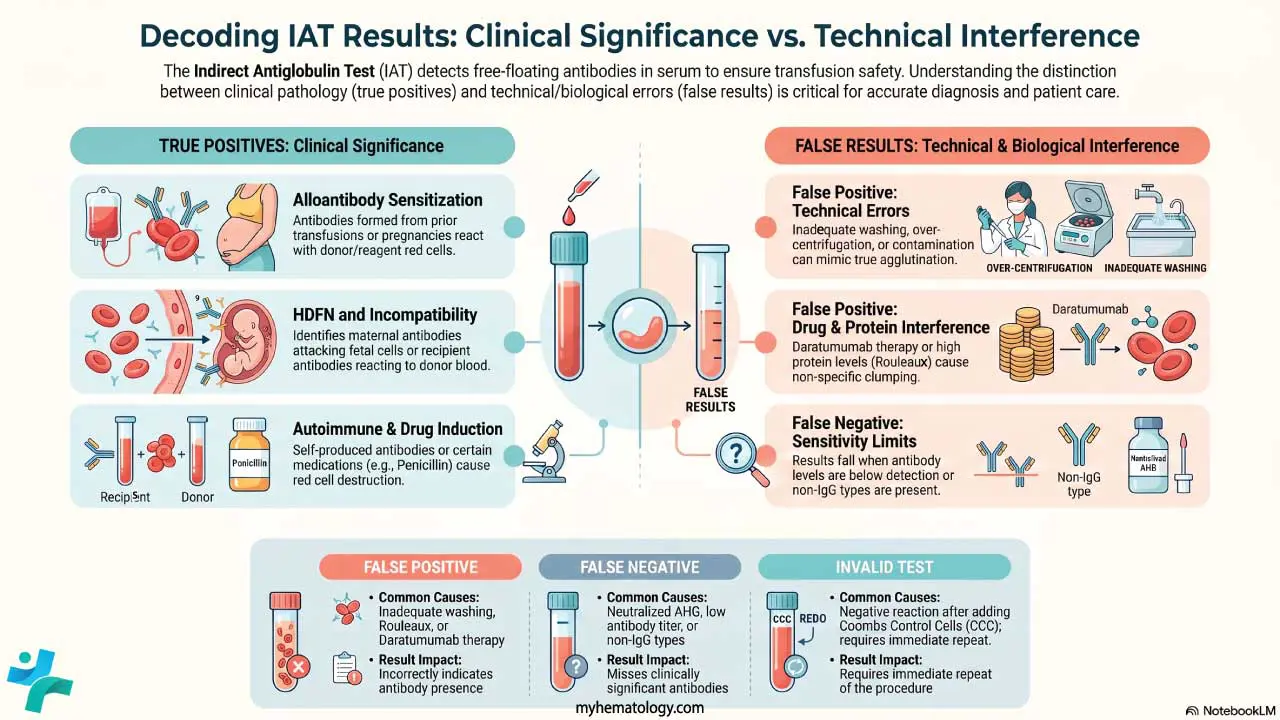
Common Causes of a True Positive IAT
A genuine positive IAT means clinically relevant antibodies are present. The usual sources are:
- Prior transfusion. Patients exposed to foreign red cell antigens may have made alloantibodies that now sit in their plasma [1,3].
- Previous pregnancies. Fetal red cells can sensitize a mother during pregnancy or delivery [2,3].
- HDFN screening. A positive antenatal IAT flags antibodies (anti-D, anti-K, anti-c, anti-Fyᵃ, anti-Jkᵃ and others) that could attack fetal red cells [2].
- Incompatible crossmatch. Patient antibody reacts with antigens on the chosen donor unit; that unit must not be used [1].
- Autoantibodies. Free autoantibody in serum can produce a positive IAT, often together with a positive DAT, in autoimmune hemolytic anemia.
- Passively acquired antibodies from IVIG, plasma, or anti-D immunoglobulin (RhIg) given for Rh prophylaxis. In pregnancy, distinguishing passive RhIg-derived anti-D from immune anti-D is a routine puzzle.
- Drug-induced antibodies caused by penicillin, cephalosporins, methyldopa, or quinidine.
Common Causes of a False-Positive IAT
- Rouleaux. High serum proteins (multiple myeloma, Waldenström macroglobulinemia) make red cells stack like coins. Saline replacement disperses rouleaux but not true agglutination.
- Over-centrifugation. Cells can be packed tightly enough to look agglutinated.
- Contamination of reagents or glassware.
- Cold autoantibodies with wide thermal amplitude. A potent IgM cold antibody can bind at room temperature and carry over into the AHG phase, although strict 37°C incubation usually prevents this.
- Anti-CD38 monoclonal antibodies. Daratumumab and isatuximab bind CD38 on reagent red cells, producing pan-reactivity that masks real alloantibodies [4,5,10]. This is now the most common drug-related interference in modern blood banks.
- Anti-CD47 monoclonal antibodies (e.g., magrolimab) cause similar pan-reactivity in ABO and IAT testing [1]. (Note: As of early 2024, the clinical development of magrolimab was discontinued by the manufacturer following FDA clinical holds due to safety and futility concerns [11]. While the serological principle remains valid for training and board exams, it will rarely be encountered in routine clinical practice moving forward.)
Common causes of a false-negative IAT
- Inadequate washing. Residual serum proteins neutralize AHG, so AHG can no longer bind sensitized cells. The result reads negative even though antibody was present. This is the classic teaching trap [1].
- Wrong antibody class. IAT detects IgG; pure IgM or IgA antibodies are missed at the AHG phase.
- Antibody below detection threshold — roughly 150–500 IgG molecules per red cell for the tube method [7].
- High-dose hook (prozone) with very high IgG paraprotein concentrations.
- Reagent or technique errors — expired AHG, too little incubation time, missed AHG addition.
Drug Interference: Daratumumab and the Anti-CD38 Problem
Anti-CD38 monoclonal antibodies are among the most important advances in myeloma therapy and one of the most common causes of pan-reactive IAT in the current era [4,6,10].
CD38 is expressed strongly on plasma cells (the drug's target) but also weakly on red cells. Daratumumab in the patient's plasma binds every reagent red cell, so the IAT reads positive against every panel cell. A real alloantibody hiding underneath cannot be seen [4,10].
The standard workaround, supported by AABB-validated methodology, is to pretreat reagent red cells with 0.2 mol/L DTT before the IAT. DTT breaks disulfide bonds in CD38 and abolishes daratumumab binding, exposing any underlying alloantibody [4,5]. Two trade-offs follow:
- DTT also destroys Kell system antigens, so anti-K cannot be detected on DTT-treated cells. Most institutions issue K-negative units empirically while a patient is on daratumumab to cover this gap [5].
- The patient should have a baseline ABO/Rh type, antibody screen, and extended phenotype or genotype recorded before starting therapy, since daratumumab can persist in plasma for up to six months after the last dose [6].
Newer mitigation methods include the low-dose DTT "Osaka method" (which preserves K antigenicity) [6], trypsin treatment, soluble CD38, and anti-daratumumab idiotype neutralizers. The take-home message: a sudden pan-reactive IAT in a myeloma patient is not a serological mystery as it is almost always the drug, and the lab needs to know about anti-CD38 therapy in advance.
Beyond the Tube: Modern IAT Methods
The spin-tube IAT is excellent for teaching and remains valuable for problem-solving, but most routine pre-transfusion testing now runs on automated platforms [1,2]:
- Column agglutination (gel cards). Patient plasma and reagent cells (which must be prepared as a 0.8% suspension, unlike the 3–5% concentration used in tube testing) are layered onto a microcolumn pre-filled with AHG-impregnated gel [1]. Agglutinates are trapped in the gel; free cells form a button at the bottom. No washing or CCC step is needed.
- Solid-phase red cell adherence (SPRCA). Reagent red cell membranes are bound to microplate wells. Patient plasma is added, washed, and indicator cells are layered on top. A diffuse pattern is positive; a tight button is negative.
- Saline tube IAT. Slow but transparent and used for reference work, problem-solving, and when other methods give discrepant results.
Gel and solid-phase methods are more sensitive to weak IgG antibodies and easier to standardize. The tube method retains an edge in detecting some antibodies that show weakly in gel and is still the format taught in most training programs [1].
Frequently Asked Questions (FAQs)
How is the IAT different from the DAT?
The DAT detects antibodies already attached to a patient's red cells in vivo and is useful for autoimmune hemolytic anemia, transfusion reactions, and HDFN. The IAT detects antibodies free in plasma that have not yet bound red cells and is useful for pre-transfusion screening, crossmatching, and antenatal screening.
Why is AHG essential to the IAT?
IgG antibodies are too small to bridge two red cells against the cells' natural charge repulsion. AHG binds two IgG molecules on different cells at once, cross-linking them and producing visible agglutination [1,3].
What does a positive antenatal IAT mean?
The mother has an antibody that may cross the placenta and damage fetal red cells. The lab will identify the antibody, type the father (and sometimes the fetus by cell-free DNA), titer the antibody, and the obstetric team may follow the pregnancy with middle cerebral artery Doppler scans to detect fetal anemia [2].
Why does daratumumab cause a positive IAT?
Daratumumab targets CD38, which red cells express weakly. The drug coats every reagent red cell and produces pan-reactivity. DTT treatment of reagent cells destroys CD38 and resolves the interference [4,5,10].
What causes a false-negative IAT?
Most often inadequate washing leaving leftover serum proteins to neutralize AHG. Other causes include the antibody being IgM rather than IgG, antibody concentration below the detection threshold, and rare interference from high IgG paraproteins or rheumatoid factor [1].
Why must Coombs control cells be added to negative IAT tubes?
Because a negative result is only valid if the AHG was active when added. CCC are IgG-coated cells that must agglutinate; if they don't, the AHG was missed, was inactive, or was neutralized by leftover protein, and the negative result must be repeated [1].
Glossary of Related Medical Terms
- Agglutination — visible clumping of red blood cells when antibodies bridge multiple cells together. The "positive" signal in the IAT.
- Alloantibody — an antibody made against red cell antigens that the person does not have, usually after transfusion or pregnancy.
- Antihuman globulin (AHG) / Coombs reagent — an antibody against human IgG (and sometimes C3d) that bridges IgG-coated red cells so clumping becomes visible.
- Autoantibody — an antibody produced against the person's own red cell antigens.
- Coombs control cells (CCC) — IgG-coated reagent red cells added to all negative IAT tubes to confirm that AHG was active and the wash was adequate.
- Crossmatch — test that mixes patient serum with donor red cells before transfusion to check compatibility.
- Daratumumab/Isatuximab — anti-CD38 monoclonal antibodies used to treat multiple myeloma; cause pan-reactive IAT until reagent cells are pretreated (commonly with DTT).
- DTT (dithiothreitol) — chemical that breaks disulfide bonds; used to denature CD38 on reagent cells so anti-CD38 drugs no longer interfere with the IAT.
- HDFN — hemolytic disease of the fetus and newborn; maternal IgG crosses the placenta and destroys fetal red cells.
- LISS (low ionic strength solution) — enhancement medium that speeds up antibody binding, allowing IAT incubation as short as 10–15 minutes.
- Polyspecific vs. monospecific AHG — polyspecific contains anti-IgG and anti-C3d; monospecific contains only anti-IgG. Most modern screening uses anti-IgG to avoid clinically insignificant complement reactions.
- Rouleaux — red cells stacked like coins because of high serum protein; can mimic agglutination but disperses with saline replacement.
- Sensitization — antibody binding to red cell antigen without visible clumping; the IAT visualizes sensitization by adding AHG.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cohn, C. S., Delaney, M., Johnson, S. T., & Katz, L. M. (Eds.). (2023). Technical manual (21st ed.). AABB.
- British Committee for Standards in Haematology, Milkins, C., Berryman, J., Cantwell, C., Elliott, C., Haggas, R., Jones, J., Rowley, M., Williams, M., & Win, N. (2013). Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories. British Committee for Standards in Haematology. Transfusion medicine (Oxford, England), 23(1), 3–35. https://doi.org/10.1111/j.1365-3148.2012.01199.x
- Theis SR, Hashmi MF. Coombs Test. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547707/
- Chapuy, C. I., Nicholson, R. T., Aguad, M. D., Chapuy, B., Laubach, J. P., Richardson, P. G., Doshi, P., & Kaufman, R. M. (2015). Resolving the daratumumab interference with blood compatibility testing. Transfusion, 55(6 Pt 2), 1545–1554. https://doi.org/10.1111/trf.13069
- Chapuy, C. I., Aguad, M. D., Nicholson, R. T., AuBuchon, J. P., Cohn, C. S., Delaney, M., Fung, M. K., Unger, M., Doshi, P., Murphy, M. F., Dumont, L. J., Kaufman, R. M., & DARA-DTT Study Group* for the BEST Collaborative (2016). International validation of a dithiothreitol (DTT)-based method to resolve the daratumumab interference with blood compatibility testing. Transfusion, 56(12), 2964–2972. https://doi.org/10.1111/trf.13789
- Hosokawa, M., Kashiwagi, H., Nakayama, K., Sakuragi, M., Nakao, M., Morikawa, T., Kiyokawa, T., Aochi, H., Nagamine, K., Shibayama, H., & Tomiyama, Y. (2018). Distinct effects of daratumumab on indirect and direct antiglobulin tests: a new method employing 0.01 mol/L dithiothreitol for negating the daratumumab interference with preserving K antigenicity (Osaka method). Transfusion, 58(12), 3003–3013. https://doi.org/10.1111/trf.14900
- Petz, L. D., & Garratty, G. (2004). Immune hemolytic anemias (2nd ed.). Churchill Livingstone.
- Bain, B. J., Bates, I., & Laffan, M. A. (Eds.). (2017). Dacie and Lewis practical haematology (12th ed.). Elsevier.
- Daniels, G. & Bromilow I. (2013). Essential Guide to Blood Groups (3rd ed.). Wiley-Blackwell.
- Sullivan, H. C., Gerner-Smidt, C., Nooka, A. K., Arthur, C. M., Thompson, L., Mener, A., Patel, S. R., Yee, M., Fasano, R. M., Josephson, C. D., Kaufman, R. M., Roback, J. D., Lonial, S., & Stowell, S. R. (2017). Daratumumab (anti-CD38) induces loss of CD38 on red blood cells. Blood, 129(22), 3033–3037. https://doi.org/10.1182/blood-2016-11-749432
- Gilead Sciences. (2024, February 7). Gilead statement on discontinuation of Phase 3 ENHANCE-3 study in AML. https://www.gilead.com/company/company-statements/2024/gilead-statement-on-discontinuation-of-phase-3-enhance-3-study-in-aml