Key Takeaways
Hemolytic Disease of the Fetus and Newborn is caused by maternal IgG antibodies crossing the placenta and destroying fetal red blood cells, most often due to RhD incompatibility, with anti-Kell and ABO as the next most important triggers.
- Pathophysiology ▾: The first Rh-incompatible pregnancy typically sensitizes the mother without harming the fetus; subsequent pregnancies with an antigen-positive fetus are at risk because of the anamnestic immune response.
- Clinical features ▾: Anemia and jaundice. Hepatosplenomegaly on examination and edema if hydrops was present prenatally.
- Laboratory investigations ▾: MCA-PSV Doppler ultrasound is the non-invasive gold standard for detecting fetal anemia in HDFN. Cell-free fetal DNA testing for fetal RHD genotype now allows targeted use of RhIg and avoids unnecessary monitoring when the fetus is RhD-negative [1].
- Treatment and management ▾: RhIg prophylaxis at 28 weeks and within 72 hours postpartum has reduced RhD alloimmunization from around 17% to less than 1% in at-risk pregnancies [1].
*Click ▾ for more information
When a pregnant person and their fetus have incompatible blood types, the mother's immune system can mistake fetal red blood cells for invaders. The result is Hemolytic Disease of the Fetus and Newborn, often shortened to HDFN and historically called erythroblastosis fetalis. It can range from mild jaundice in a newborn to life-threatening fetal anemia. The good news: with current prevention and monitoring, most at-risk pregnancies now end well [1,5].
Quick orientation
Hemolytic Disease of the Fetus and Newborn happens when maternal IgG antibodies cross the placenta and attack fetal red blood cells. The most common trigger is RhD incompatibility, but ABO and minor antigens (especially Kell) also cause disease [4,8]. In the United States, around 80 cases per 100,000 live births are reported, though severe HDFN is rarer thanks to RhIg prophylaxis [5].
What you will find below
- How blood group systems set the stage
- Why first pregnancies are usually safe and later ones may not be
- How clinicians detect and grade severity before and after birth
- Current management, from RhIg to intrauterine transfusion
- A look at nipocalimab, a new therapy that could change the field
- Long-term follow-up and what caregivers can expect at home
What is Hemolytic Disease of the Fetus and Newborn?
HDFN is an alloimmune hemolytic anemia (red cell destruction caused by antibodies from another person of the same species) in the fetus or newborn [8]. The mother carries an antigen-negative blood group and the fetus inherits the antigen from the father. If maternal antibodies form and cross the placenta, they coat fetal red cells, which are then destroyed by macrophages in the fetal spleen [4,7].
Two main systems drive the disease:
- Rh (D) incompatibility — historically the most severe form
- ABO incompatibility — common but usually mild
- Minor antigens — anti-Kell, anti-c, and anti-E are the most clinically important [4]
How blood groups create the problem
The ABO system in brief
ABO blood typing is based on A and B sugar antigens on red cells, with matching anti-A and anti-B antibodies in plasma. These antibodies are naturally occurring — they appear without any prior exposure. Most are IgM, which is too large to cross the placenta. That is why ABO Hemolytic Disease of the Fetus and Newborn is usually mild.
ABO incompatibility most often occurs when a Type O mother carries a Type A or B fetus. Type O mothers can produce some IgG anti-A or anti-B that does cross the placenta and causes mild to moderate hemolysis. Hydrops fetalis from ABO incompatibility is rare [8].
The Rh system
The Rh system has more than 50 antigens, but the D antigen is the one that matters most clinically [7]. People who carry D on their red cells are RhD-positive; those who do not are RhD-negative. RhD-negative people do not have natural anti-D. They only make anti-D after exposure to RhD-positive cells, which can happen during pregnancy or transfusion. Because anti-D is IgG, it crosses the placenta freely and can attack the fetal red cells of an RhD-positive baby.
Anti-Kell deserves special mention
Anti-Kell (anti-K) is the third most common cause of severe HDFN. It behaves differently from anti-D: it not only destroys mature red cells but also suppresses fetal red cell production in the marrow [4]. As a result, antibody titer correlates poorly with severity, and clinicians use a lower threshold for triggering close fetal monitoring than for other antibodies.
How HDFN develops: the pathophysiology
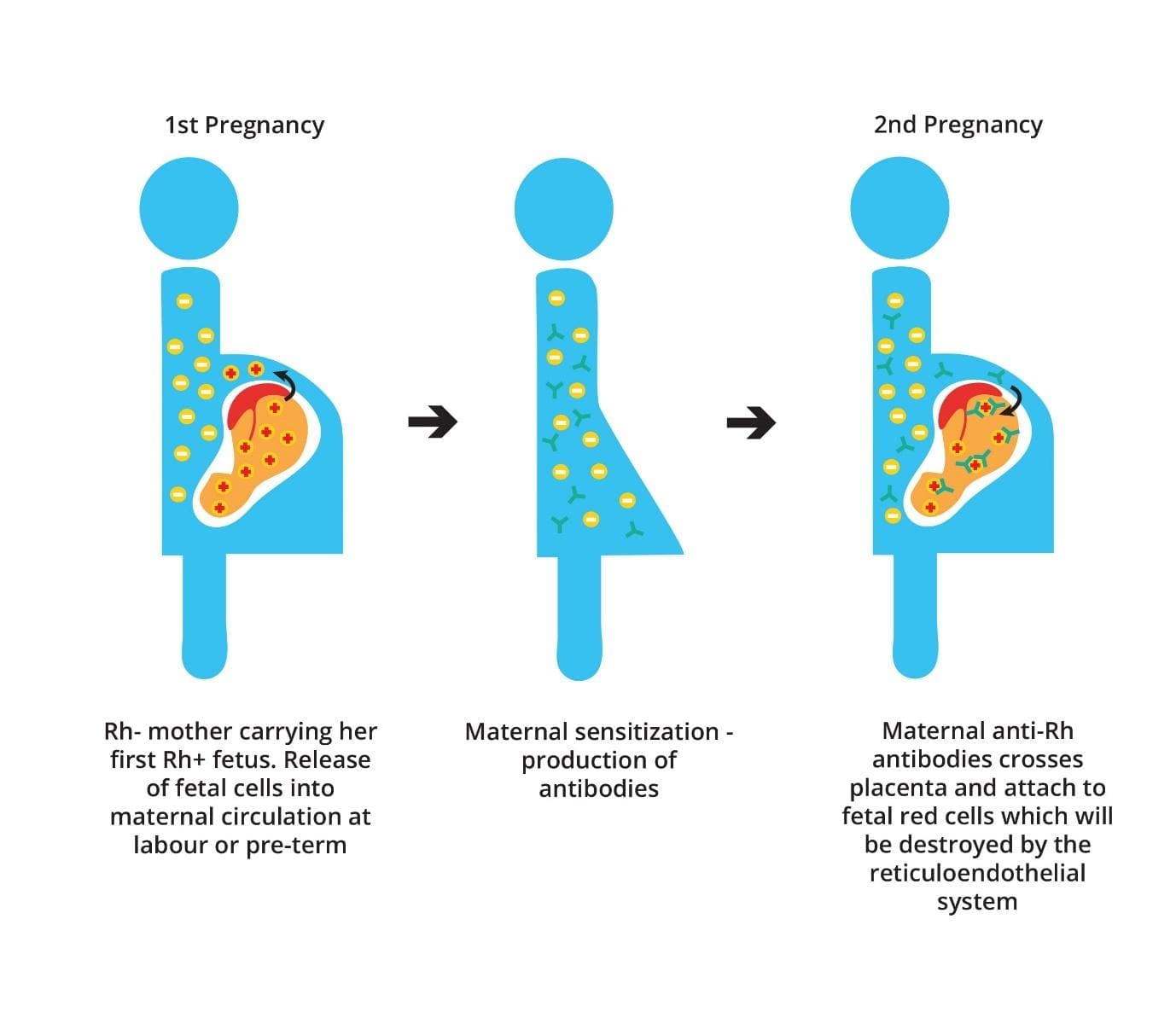
First pregnancy: sensitization
In a typical Rh-incompatible pregnancy, the RhD-negative mother is exposed to fetal RhD-positive red cells during placental microbleeds or, more often, at delivery. Her immune system recognizes the D antigen as foreign and starts producing anti-D antibodies. The first pregnancy itself usually proceeds without hemolytic disease because not enough antibody crosses to the fetus in time [4,7].
Later pregnancies: the anamnestic response
If a sensitized mother carries another RhD-positive fetus, her immune memory kicks in. This is the anamnestic response: faster, stronger antibody production. The IgG she now makes crosses the placenta easily, binds to fetal red cells carrying the D antigen, and tags them for destruction by fetal splenic macrophages [7,8]. The result is fetal anemia and a rising bilirubin load, which the placenta partly clears before birth.
After birth, the newborn must clear bilirubin alone, but the immature liver cannot keep up. Hyperbilirubinemia (high blood bilirubin) follows, and severe cases risk kernicterus — bilirubin-induced brain injury [6].
Signs and symptoms
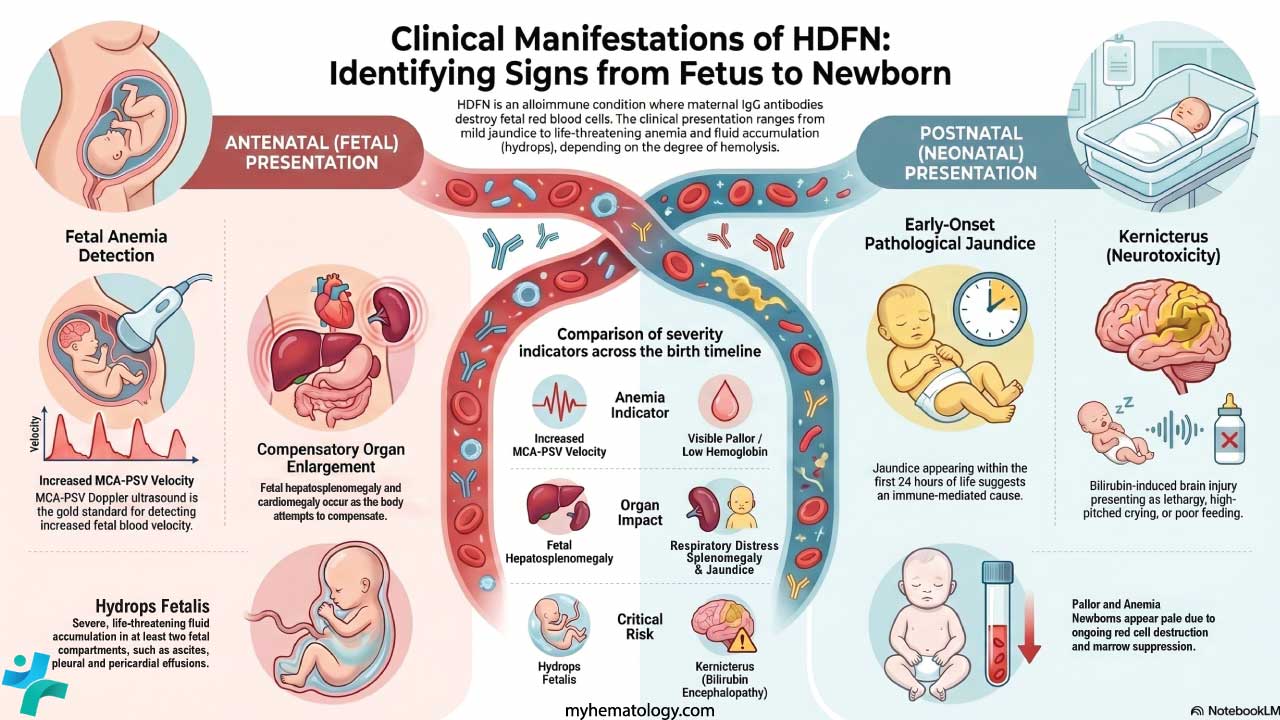
Before birth: antenatal presentation
In sensitized pregnancies, fetal anemia is usually picked up during routine surveillance rather than from symptoms. Clinicians watch for:
- Increased MCA-PSV on Doppler ultrasound (the hallmark sign of fetal anemia)
- Cardiomegaly and signs of heart strain as the fetal heart compensates
- Hepatosplenomegaly from extramedullary hematopoiesis (the liver and spleen making red cells outside the marrow)
The most severe presentation is hydrops fetalis: widespread fluid build-up in at least two fetal compartments, including ascites (fluid in the abdomen), pleural and pericardial effusions, generalized skin edema, polyhydramnios (excess amniotic fluid), and a thickened placenta [7].
After birth: neonatal presentation
Once the placenta is gone, bilirubin rises quickly. Clinicians look for:
- Jaundice within the first 24 hours of life, with a distinctive orange-yellow hue from unconjugated bilirubin. Early jaundice is always pathological [6].
- Pallor from ongoing hemolysis and anemia
- Hepatosplenomegaly on examination
- Edema if hydrops was present prenatally
- Respiratory distress if pleural effusions or severe anemia compromise breathing
The dreaded complication is kernicterus. Early signs are subtle: lethargy, poor feeding, high-pitched cry, hypotonia (low muscle tone). Late signs include hypertonia with arched neck (opisthotonus), seizures, fever, abnormal upward gaze, and apnea. Long-term sequelae can include athetoid cerebral palsy, hearing loss, intellectual disability, and dental enamel defects [6,8].

How HDFN is tested
Antenatal investigations
The goals: identify pregnancies at risk and grade severity if antibodies are present.
Maternal screening. Every pregnant person should have ABO and RhD typing, plus an indirect antiglobulin test (IAT) early in pregnancy to screen for clinically significant antibodies [4]. If an antibody is found, titers are tracked. For most antibodies, a critical titer of around 16 triggers fetal surveillance. For anti-Kell, because it uniquely suppresses fetal erythropoiesis and correlates poorly with disease severity, the critical titer threshold is much lower (often 1:4 or even any detectable titer) to trigger close MCA-PSV monitoring [4].
Cell-free fetal DNA (cfDNA) for fetal RHD genotyping. This is the most significant recent advance in Hemolytic Disease of the Fetus and Newborn diagnostics. A maternal blood sample is analyzed for fetal DNA fragments to determine whether the fetus carries RhD or another red cell antigen [1]. The practical impact:
- In sensitized RhD-negative pregnancies where the fetus is RhD-negative, no monitoring or intervention is needed.
- In non-sensitized RhD-negative pregnancies, RhIg can be given only to those carrying an RhD-positive fetus, conserving a globally limited blood product.
Routine fetal RHD screening has been standard in much of Europe for several years, and US practice is shifting in this direction [1].
Fetal surveillance with MCA-PSV. Middle cerebral artery peak systolic velocity Doppler is the non-invasive gold standard. As anemia develops, blood becomes less viscous and flows faster through the fetal cerebral arteries. A reading above 1.5 multiples of the median (MoM) for gestational age predicts moderate to severe anemia and usually triggers intrauterine transfusion [4]. MCA-PSV becomes less reliable after 35 weeks, when delivery becomes the safer option.
Invasive tests (rare today). Cordocentesis (percutaneous umbilical blood sampling) directly measures fetal hemoglobin, hematocrit, and bilirubin. It is now reserved for the moment of intrauterine transfusion. Amniocentesis with ΔOD450 was once the standard but has been replaced by MCA-PSV.
Postnatal investigations
After birth, the goals are confirming immune-mediated hemolysis and tracking severity.
- ABO and RhD typing of the newborn
- Direct Antiglobulin Test (DAT, Coombs). A positive DAT confirms maternal IgG is coating the newborn's red cells. This is the diagnostic hallmark [6].
- Complete blood count with reticulocyte count. Measures anemia and how hard the marrow is compensating.
- Total and fractionated serum bilirubin, plotted against current risk-adjusted clinical thresholds (such as the 2022 American Academy of Pediatrics guidelines). These guidelines factor in gestational age, postnatal age in hours, and neurotoxicity risk factors (including HDFN) to guide phototherapy and exchange transfusion decisions [9].
| Condition | Key Mechanism | Newborn Presentation | Diagnostic Clue |
|---|---|---|---|
|
Rh, ABO, or Minor Antigen Incompatibility
DAT Positive
|
Maternal IgG destroys fetal RBCs | Early jaundice, anaemia, hepatosplenomegaly; hydrops in severe cases | Positive Direct Antiglobulin Test (DAT) — newborn's RBCs are coated with maternal IgG |
|
G6PD or Pyruvate Kinase Deficiency
DAT Negative
|
RBCs vulnerable to oxidative stress | Jaundice (often delayed or triggered), anaemia | Negative DAT; enzyme assay confirmatory; bite cells on smear (G6PD) |
|
Hereditary Spherocytosis
DAT Negative
|
Rigid spherocytes destroyed in spleen | Anaemia, jaundice, splenomegaly | Negative DAT; EMA binding test confirmatory |
|
Sepsis
DAT Negative
|
Toxin- or DIC-related haemolysis | Jaundice, anaemia, fever, lethargy | Negative DAT; positive blood culture |
|
Concealed Haemorrhage
DAT Negative
|
RBCs sequestered, then broken down | Anaemia, delayed jaundice | Negative DAT; visible bruising on examination |
|
Physiologic Jaundice
DAT Negative
|
Slow bilirubin conjugation | Jaundice after 24 hours; peaks day 3–5 | Negative DAT; normal CBC |
|
Non-immune Hydrops
DAT Negative
|
Heart failure or low protein causes fluid leakage | Hydrops with severe anaemia | Negative DAT; viral or genetic testing — Parvovirus B19, alpha-thalassaemia |
How HDFN is treated
The three goals are: prevent sensitization, correct fetal anemia, prevent neonatal neurotoxicity.
Prevention: RhIg prophylaxis
RhD Immune Globulin (RhIg, RhoGAM). RhIg is a concentrated dose of anti-D antibodies. When given to an RhD-negative mother, it binds any fetal RhD-positive cells in her circulation before her own immune system can react. Standard dosing is around 28 weeks of gestation and within 72 hours postpartum if the newborn is RhD-positive. Additional doses are given after potential feto-maternal hemorrhage events, including trauma, miscarriage, or amniocentesis [4,7].
Why RhIg works. It acts as antibody-mediated immune suppression: the fetal red cells are cleared before the mother's B cells can mount a primary response. Widespread RhIg use has reduced RhD alloimmunization from around 17% per at-risk pregnancy to less than 1% [1]. It is important for caregivers to note that RhIg is exclusively effective against the RhD antigen; there is no prophylactic immune globulin available to prevent sensitization to Kell, ABO, or other minor blood group antigens [7].
Targeted prophylaxis. Cell-free fetal DNA testing now allows clinicians to skip RhIg in the roughly 40% of RhD-negative pregnancies where the fetus is also RhD-negative.
Antenatal management of an affected fetus
Once a mother is sensitized, the focus shifts to the fetus.
- Serial MCA-PSV Doppler. Routine surveillance starting around 18–20 weeks if titers are critical.
- Intrauterine transfusion (IUT). The definitive treatment for severe fetal anemia. Compatible donor blood (typically O-negative, irradiated, CMV-safe, leukoreduced) is transfused into the fetal umbilical vein under ultrasound guidance. IUT can be repeated through pregnancy. At experienced centers, survival exceeds 90% in non-hydropic fetuses and around 75% in hydropic fetuses, with generally favorable neurodevelopmental outcomes [4,7].
- Therapeutic plasma exchange (plasmapheresis) combined with maternal IVIG is utilized for very-high-risk cases (such as a history of fetal loss before 24 weeks) where severe disease develops before the fetus is old enough for a safe IUT. Plasmapheresis physically removes circulating maternal antibodies, and IVIG suppresses their rebound. This combination acts as a vital "bridge" therapy to delay severe anemia until an intrauterine transfusion becomes technically feasible around 20 to 22 weeks of gestation [10].
- Early delivery at 35–37 weeks if monitoring shows worsening anemia near term.
A new option on the horizon: nipocalimab
Nipocalimab is a monoclonal antibody that blocks FcRn, the neonatal Fc receptor that transports IgG across the placenta. By blocking FcRn, nipocalimab reduces the amount of harmful maternal IgG that reaches the fetus and lengthens the time before the fetus develops severe anemia [2,3].
In the Phase 2 UNITY trial, around 54% of high-risk alloimmunized pregnancies achieved live birth at or after 32 weeks of gestation without needing an intrauterine transfusion [2]. The Phase 3 AZALEA trial is ongoing [3]. Nipocalimab has FDA Fast Track and Orphan Drug designations for HDFN. It is not yet FDA-approved for this indication, but if the Phase 3 results hold, it could change first-line management for severe HDFN.
Postnatal management of the newborn
Phototherapy is the first-line treatment for hyperbilirubinemia. Specific blue-green wavelengths (around 420–490 nm) convert bilirubin in the skin into water-soluble photoisomers that the body can excrete without liver conjugation. Bilirubin is plotted on hour-specific nomograms; intensive phototherapy is used for higher levels [6].

Exchange transfusion is reserved for severe cases. Indications include bilirubin levels approaching kernicterus thresholds despite intensive phototherapy, signs of acute bilirubin encephalopathy, or severe anemia at birth (often hemoglobin below 10–12 g/dL, depending on the clinical picture). A double-volume exchange removes most of the sensitized red cells, circulating maternal antibodies, and excess bilirubin. It is effective but carries real risks: electrolyte disturbances, infection, vascular complications, and rarely death [6,8].
Intravenous immunoglobulin (IVIG) is sometimes used alongside phototherapy to reduce ongoing hemolysis. However, recent clinical guidelines strongly recommend limiting its use to cases where the bilirubin level is rapidly rising or is within 2 mg/dL of the exchange transfusion threshold despite intensive phototherapy. This narrowed, cautious indication is due to mixed efficacy in recent trials and a recognized association between postnatal IVIG administration and necrotizing enterocolitis (NEC) [9].
Supportive care includes top-up transfusions if anemia recurs in the weeks after birth, careful hydration during phototherapy, and respiratory support for hydropic infants.
Long-term follow-up
Hemolytic Disease of the Fetus and Newborn does not always end at discharge. Maternal antibodies can persist in the infant's circulation for up to 12 weeks, and ongoing hemolysis may suppress erythropoiesis. Standard follow-up includes:
- Repeat CBCs over the first 8–12 weeks
- Auditory brainstem response (ABR) testing for any infant with severe hyperbilirubinemia, because bilirubin is toxic to the auditory pathway
- Neurodevelopmental follow-up to detect kernicterus sequelae
- Monitoring for hyporegenerative anemia, particularly in infants who received intrauterine transfusions (IUTs). IUTs suppress the fetal bone marrow's own red blood cell production. As the transfused adult red cells naturally reach the end of their lifespan, these infants are at the highest risk for delayed profound anemia and frequently require "top-up" blood transfusions in the first few months of life [6].
A note for caregivers
If your baby is being treated for HDFN, knowing what to expect makes the hospital stay easier. Phototherapy looks dramatic — bright lights, eye protection, frequent feedings — but it is painless. After discharge, watch for returning yellowness of the skin or eyes, unusual sleepiness, poor feeding, or pallor, and bring your baby to scheduled follow-up blood checks. Hearing screens and developmental check-ins are routine, not a sign that something has gone wrong. Most babies treated for HDFN today grow up healthy.
Frequently Asked Questions (FAQs)
What is hemolytic disease of the fetus and newborn (HDFN)?
HDFN is a condition where a pregnant person's IgG antibodies cross the placenta and destroy the fetus's red blood cells. It happens when the mother and fetus have incompatible red cell antigens, most commonly RhD. Severe cases cause fetal anemia, jaundice after birth, and sometimes hydrops fetalis. Modern prevention with RhIg and treatment with intrauterine transfusion mean most affected pregnancies now end with healthy babies [1,4].
Why is the first pregnancy usually safe but later ones at risk?
A first Rh-incompatible pregnancy exposes the mother to fetal red cells mostly at delivery. By then her immune system can recognize the D antigen, but the existing pregnancy is already over. By the next pregnancy, immune memory produces large amounts of IgG anti-D quickly. These antibodies cross the placenta and attack fetal red cells. This faster, stronger second response is called the anamnestic response [7].
How is HDFN prevented?
The cornerstone is RhD immune globulin (RhIg, RhoGAM and similar) given to RhD-negative pregnant people at around 28 weeks and again within 72 hours after delivery if the newborn is RhD-positive. RhIg neutralizes fetal RhD-positive cells before the mother's immune system reacts. Cell-free fetal DNA testing now allows clinicians to give RhIg only when the fetus is actually RhD-positive [1].
What is the most accurate test for fetal anemia in HDFN?
Middle cerebral artery peak systolic velocity (MCA-PSV) Doppler ultrasound is the standard non-invasive test. As anemia thins the blood, it flows faster through the fetal cerebral arteries. A reading above 1.5 multiples of the median for gestational age predicts moderate to severe anemia and usually triggers an intrauterine transfusion [4].
What is nipocalimab and is it approved for HDFN? Nipocalimab is a monoclonal antibody that blocks the FcRn receptor responsible for moving IgG from mother to fetus across the placenta. By blocking FcRn, less harmful antibody reaches the fetus. The Phase 2 UNITY trial showed about 54% of high-risk pregnancies achieved live birth at or after 32 weeks without intrauterine transfusion [2]. The Phase 3 AZALEA trial is ongoing [3]. Nipocalimab is not yet FDA-approved for HDFN.
How long does HDFN affect the baby after birth?
Most newborns recover within days to weeks once jaundice and anemia are treated. However, maternal antibodies can persist in the baby's circulation for up to 12 weeks, so mild ongoing hemolysis may continue. Babies need follow-up blood counts during this period, and some need additional small transfusions if anemia returns. Hearing tests and developmental checks are routine [6].
Glossary of Related Medical Terms
- Alloimmunization — When a person makes antibodies against red blood cell antigens from another person of the same species (e.g., mother making antibodies against fetal red cell antigens she lacks).
- Anamnestic response — The faster, stronger immune response that occurs on second or later exposure to an antigen, because memory cells are already primed.
- Antigen — A molecule (often on a cell surface) that the immune system can recognize and respond to.
- Antibody — A protein made by B cells that binds to a specific antigen. IgG is small enough to cross the placenta; IgM is not.
- Cell-free fetal DNA (cfDNA) — Small fragments of fetal DNA that circulate in the mother's bloodstream during pregnancy and can be tested non-invasively.
- DAT (Direct Antiglobulin Test) / Coombs test — A blood test that detects antibodies already stuck to red blood cells. A positive DAT in a newborn confirms immune-mediated hemolysis.
- Erythropoiesis — The production of red blood cells, mainly in the bone marrow.
- Exchange transfusion — A procedure that gradually replaces a newborn's blood with donor blood to remove bilirubin, antibodies, and damaged red cells.
- FcRn (neonatal Fc receptor) — A receptor that transports IgG antibodies across the placenta and recycles them in the body. Blocking it prevents harmful maternal IgG from reaching the fetus.
- Hemolysis — Destruction of red blood cells, releasing hemoglobin and producing bilirubin.
- Hydrops fetalis — Severe fluid build-up in two or more fetal body compartments (e.g., chest, abdomen, skin); a life-threatening complication of severe fetal anemia.
- Hyperbilirubinemia — Abnormally high blood bilirubin, the yellow pigment from broken-down red cells.
- IgG / IgM — Two classes of antibody. IgG crosses the placenta; IgM does not.
- Intrauterine transfusion (IUT) — Transfusion of donor red cells directly into the fetus (usually via the umbilical vein) under ultrasound guidance.
- Kernicterus — Brain damage caused by bilirubin crossing the blood-brain barrier in newborns; preventable with timely treatment.
- MCA-PSV (middle cerebral artery peak systolic velocity) — An ultrasound measurement of how fast blood flows in a fetal brain artery; a non-invasive way to detect fetal anemia.
- RhIg (Rh immune globulin, e.g., RhoGAM) — An injection of anti-D antibodies given to RhD-negative mothers to prevent them from making their own anti-D antibodies.
- Sensitization — The first immune exposure that causes the body to start producing antibodies against an antigen.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Moise K. J., Jr (2025). The use of free DNA for fetal RHD genotyping in the Rh negative pregnant patient-the time has come. American journal of obstetrics and gynecology, 232(2), 188–193. https://doi.org/10.1016/j.ajog.2024.08.017
- Moise, K. J., Jr, Ling, L. E., Oepkes, D., Tiblad, E., Verweij, E. J. T. J., Lopriore, E., Smoleniec, J., Sachs, U. J., Bein, G., Kilby, M. D., Miller, R. S., Devlieger, R., Audibert, F., Emery, S. P., Markham, K., Norton, M. E., Ocón-Hernández, O., Pandya, P., Pereira, L., Silver, R. M., … UNITY Study Group (2024). Nipocalimab in Early-Onset Severe Hemolytic Disease of the Fetus and Newborn. The New England journal of medicine, 391(6), 526–537. https://doi.org/10.1056/NEJMoa2314466
- Komatsu, Y., Verweij, E. J. T. J., Tiblad, E., Lopriore, E., Oepkes, D., Agarwal, P., Lam, E., Leu, J. H., Ling, L. E., Nelson, R. M., Olusajo, V., Saeed-Khawaja, S., Tjoa, M. L., Zhou, J., Amin, U., Sirah, W., & Moise, K. J. (2025). Design of a Phase 3, Global, Multicenter, Randomized, Placebo-Controlled, Double-Blind Study of Nipocalimab in Pregnancies at Risk for Severe Hemolytic Disease of the Fetus and Newborn. American journal of perinatology, 42(7), 842–853. https://doi.org/10.1055/a-2404-8089
- Society for Maternal-Fetal Medicine (SMFM). Electronic address: [email protected], Mari, G., Norton, M. E., Stone, J., Berghella, V., Sciscione, A. C., Tate, D., & Schenone, M. H. (2015). Society for Maternal-Fetal Medicine (SMFM) Clinical Guideline #8: the fetus at risk for anemia--diagnosis and management. American journal of obstetrics and gynecology, 212(6), 697–710. https://doi.org/10.1016/j.ajog.2015.01.059
- Yu, D., Ling, L. E., Krumme, A. A., Tjoa, M. L., & Moise, K. J., Jr (2023). Live birth prevalence of hemolytic disease of the fetus and newborn in the United States from 1996 to 2010. AJOG global reports, 3(2), 100203. https://doi.org/10.1016/j.xagr.2023.100203
- De Winter, D. P., Hulzebos, C., Van 't Oever, R. M., De Haas, M., Verweij, E. J., & Lopriore, E. (2023). History and current standard of postnatal management in hemolytic disease of the fetus and newborn. European journal of pediatrics, 182(2), 489–500. https://doi.org/10.1007/s00431-022-04724-0
- Delaney, M., & Matthews, D. C. (2015). Hemolytic disease of the fetus and newborn: managing the mother, fetus, and newborn. Hematology. American Society of Hematology. Education Program, 2015, 146–151. https://doi.org/10.1182/asheducation-2015.1.146
- Hall V, Vadakekut ES, Maines J, et al. Hemolytic Disease of the Fetus and Newborn. [Updated 2025 Jan 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557423/
- Kemper, A. R., Newman, T. B., Slaughter, J. L., Maisels, M. J., Watchko, J. F., Downs, S. M., Grout, R. W., Bundy, D. G., Stark, A. R., Bogen, D. L., Holmes, A. V., Feldman-Winter, L. B., Bhutani, V. K., Brown, S. R., Maradiaga Panayotti, G. M., Okechukwu, K., Rappo, P. D., & Russell, T. L. (2022). Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 150(3), e2022058859. https://doi.org/10.1542/peds.2022-058859
- Zwiers, C., van Kamp, I., Oepkes, D., & Lopriore, E. (2017). Intrauterine transfusion and non-invasive treatment options for hemolytic disease of the fetus and newborn - review on current management and outcome. Expert review of hematology, 10(4), 337–344. https://doi.org/10.1080/17474086.2017.1305265