Key Takeaways
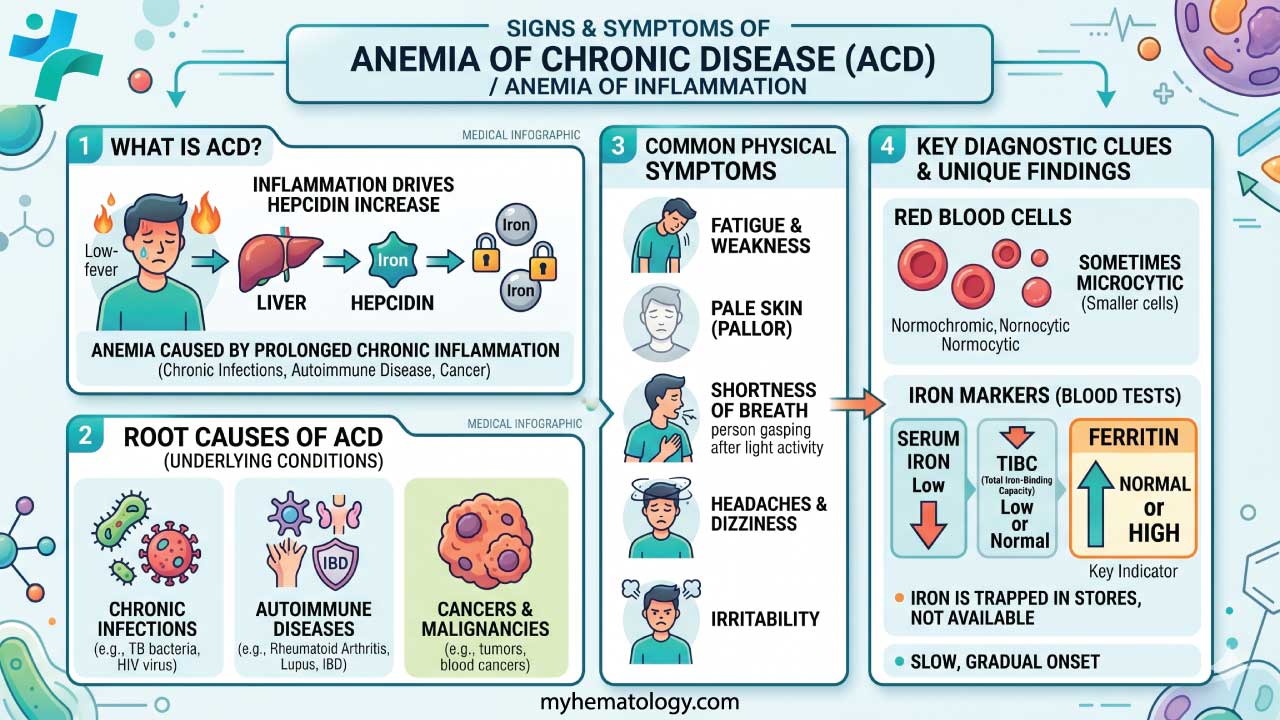
Anemia of chronic disease (ACD), also called anemia of inflammation, is a common anemia caused by long-standing inflammation that disrupts iron use and red blood cell production [1,3].
- Pathophysiology ▾: The central problem is hepcidin, a liver hormone driven up by interleukin-6 (IL-6), which locks iron inside storage cells so the bone marrow cannot use it [3,7].
- Signs and Symptoms ▾: Often has non-specific symptoms like fatigue, weakness, and shortness of breath. Symptoms can be easily overlooked.
- Laboratory Diagnosis ▾: Typical labs show low serum iron, normal or high ferritin, low or normal TIBC, and a low reticulocyte count, separating ACD from iron deficiency anemia [5,6]. Hemoglobin is usually 8.0–9.5 g/dL, and the anemia is most often normocytic but can become microcytic in chronic, severe cases [1].
- Treatment ▾: Treating the underlying inflammation is the cornerstone of management; intravenous iron, ESAs, and newer HIF-PH inhibitors are added in selected cases [4,8,9].
*Click ▾ for more information
Introduction
If you have ever cared for a patient with rheumatoid arthritis, chronic kidney disease, or a long-running infection and noticed their hemoglobin stays stubbornly low, you have already met anemia of chronic disease. It is one of the most common anemias seen in hospitals, second only to iron deficiency anemia [1,3]. The puzzle is that these patients often have plenty of iron in their bodies. The problem is that they cannot use it.
Anemia of chronic disease (anemia of inflammation) develops when sustained inflammation interferes with the normal supply chain between iron stores and the bone marrow. This guide walks you through why it happens, how to recognize it, how to tell it apart from iron deficiency, and how clinicians treat it in 2026.
Definition of Anemia
Anemia is a reduced ability of the blood to carry oxygen. The World Health Organization defines anemia using hemoglobin (Hb) cutoffs, updated in 2024, with thresholds that differ by age, sex, and pregnancy status [12]. In adults, the broad cutoffs are Hb below 13 g/dL in men and below 12 g/dL in non-pregnant women.
Anemia generally arises from one of three problems:
- Too few red blood cells.
- Too little hemoglobin in each cell.
- Hemoglobin that doesn't function properly.
Anemias are commonly classified by red blood cell size on a complete blood count (CBC):
- Microcytic (small cells, MCV < 80 fL) — most often iron deficiency anemia.
- Normocytic (normal-sized cells) — includes anemia of chronic disease, aplastic anemia, and many hemolytic anemias.
- Macrocytic (large cells, MCV > 100 fL) — typically vitamin B12 or folate deficiency, liver disease, or alcohol-related causes.
ACD usually sits in the normocytic group, but in long-standing inflammation it can drift into microcytic territory and start to look like iron deficiency [1].
Causes of Anemia of Chronic Disease
Any condition that keeps the immune system switched on for weeks to months can trigger ACD. The common culprits group into a few categories.
Chronic infections:
- Tuberculosis, osteomyelitis (bone infection), and endocarditis.
- HIV and chronic hepatitis B or C.
- Persistent parasitic infections such as malaria.
Autoimmune diseases:
- Rheumatoid arthritis.
- Systemic lupus erythematosus (SLE).
- Inflammatory bowel disease, including Crohn's disease and ulcerative colitis.
Other chronic inflammatory conditions:
- Chronic kidney disease (CKD).
- Many cancers, including lymphoma, carcinoma, and sarcoma.
- Chronic heart failure, where low-grade inflammation contributes alongside iron deficiency [10].
- Obesity-related low-grade inflammation, which is increasingly recognized as a driver of mild ACD [6].
Less common triggers:
- Vasculitides (inflammation of blood vessels).
- Sarcoidosis.
- Persistent post-viral inflammation, including Long COVID, which is increasingly recognized as a driver of mild, normocytic ACD that mirrors the pathophysiology seen in classic autoimmune conditions [13].
Pathophysiology of Anemia of Inflammation
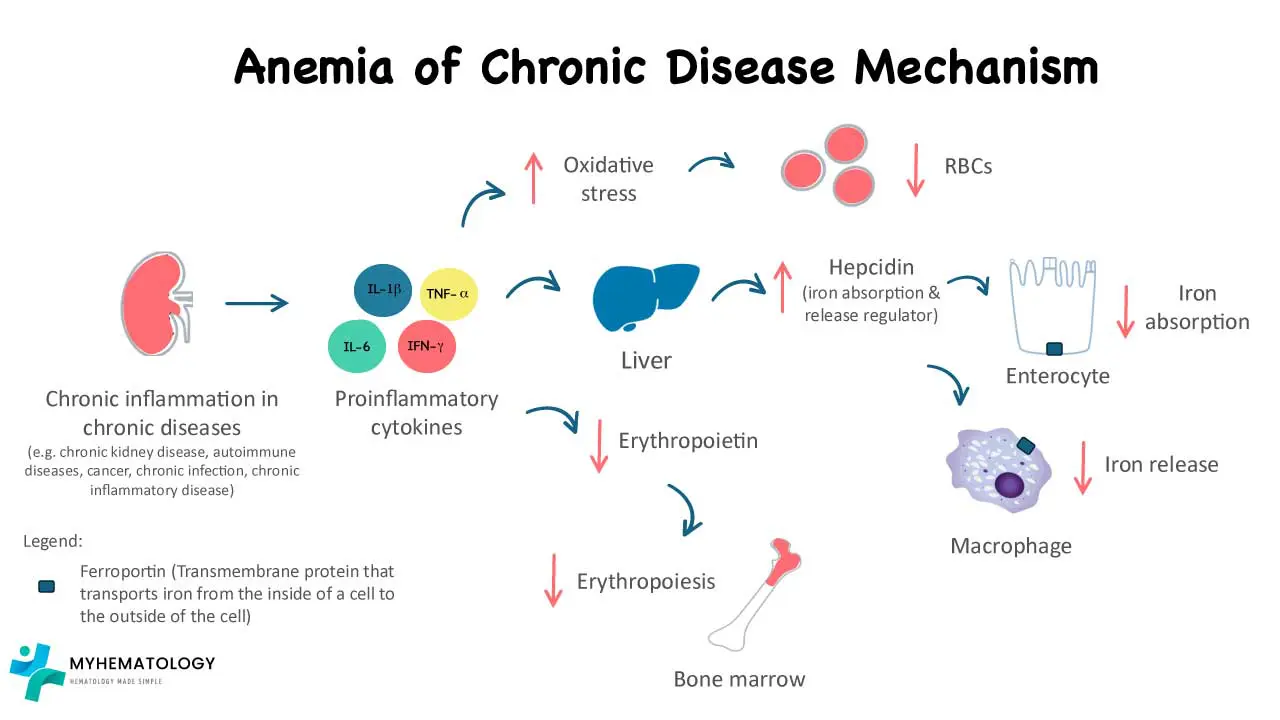
The pathophysiology of anemia of chronic disease is the most important section to understand, because every diagnostic and treatment decision flows from it. Four mechanisms are at work, and they reinforce each other [3,4,7].
1. Hepcidin Locks Iron Away
Inflammation, especially IL-6 from the liver and immune cells, drives production of hepcidin. Hepcidin binds to ferroportin, the protein that moves iron out of cells. When ferroportin is degraded, iron stays trapped inside gut cells (enterocytes) and macrophages. Even with full iron stores, the bone marrow is starved [3,7].
This is the phenomenon of functional iron deficiency: plenty of iron in storage, but none reaching the marrow.
2. EPO Production and Response Are Suppressed
Erythropoietin (EPO) is the kidney hormone that tells the marrow to make more red blood cells. Pro-inflammatory cytokines such as IL-1 and TNF-α reduce EPO production and, just as importantly, blunt the marrow's response to it by disrupting the JAK2/STAT5 signaling pathway in red cell precursors [3,4]. The marrow effectively goes deaf.
3. Erythroferrone Signaling Fails
Normally, when EPO rises, developing red blood cells release erythroferrone (ERFE), which lowers hepcidin and frees up iron. In ACD, the IL-6 signal overwhelms this feedback loop. ERFE goes up but cannot bring hepcidin down [4].
4. Red Blood Cell Lifespan Shortens
Inflamed macrophages in the spleen and liver become more aggressive at clearing red blood cells. The standard 120-day lifespan is shortened, putting more strain on a marrow that is already underperforming [3]. Reactive oxygen species in the marrow microenvironment add to this stress, causing some red cell precursors to die before they ever mature.
The end result is a low hemoglobin from three converging hits: less iron available, less marrow response, and faster red cell loss.
Iron dysregulation and hepcidin
While iron stores might appear normal, the body struggles to utilize it effectively for red blood cell production due to hepcidin's action.
Signs and Symptoms
Symptoms of anemia of chronic disease tend to be quiet and easily blamed on the underlying illness. That's part of why it is so often missed.
Common general symptoms include:
- Fatigue and weakness.
- Shortness of breath, especially on exertion.
- Pale skin and mucous membranes.
- Dizziness or lightheadedness.
- Trouble concentrating.
- Reduced exercise tolerance.
Less common features include chest pain, headaches, cold hands and feet, restlessness, and loss of appetite. In older patients or those with heart disease, even mild anemia can tip them into more obvious symptoms.
Complications of Anemia
ACD is rarely fatal on its own, but it adds load to bodies already coping with serious disease.
- Worsened heart failure: Anemia reduces oxygen-carrying capacity, forcing the heart to work harder. In heart failure with reduced ejection fraction, iron deficiency and ACD-pattern anemia are linked to more hospitalizations and worse symptoms [10].
- Reduced quality of life: Persistent fatigue, breathlessness, and cognitive dulling interfere with work, study, and daily activities.
- More hospitalizations: Patients with ACD-related complications are admitted more often, particularly those with CKD or heart failure.
- Cognitive effects: In chronic, untreated anemia, reduced oxygen delivery to the brain can affect concentration and memory.
Laboratory Investigations
A good workup for anemia of chronic disease has two goals: confirm the iron-block pattern and rule out absolute iron deficiency.
Complete Blood Count and Peripheral Blood Film
Hemoglobin is typically 8.0–9.5 g/dL [1]. The MCV is usually normocytic and normochromic at first, but long-standing or severe inflammation can push it into microcytic territory. The reticulocyte count is low, reflecting an underproducing marrow. The blood film is often unremarkable; if microcytosis is present, it is usually milder than in true iron deficiency [5].
Standard Iron Studies
This is where ACD is most easily separated from iron deficiency anemia.
| Parameter | Result in ACD | Why |
|---|---|---|
| Serum iron | Low | Hepcidin blocks release from macrophages |
| Ferritin | Normal or high | Stores are intact and ferritin rises in inflammation |
| TIBC | Low or normal | Transferrin production falls in inflammation |
| Transferrin saturation | Low (often 15–20%) | Less iron is available to bind transferrin |
In patients with systemic inflammation (most notably chronic kidney disease (CKD) and heart failure) the standard diagnostic thresholds for iron deficiency change. Clinicians typically diagnose absolute or functional iron deficiency requiring therapy when the transferrin saturation (TSAT) is < 20% and ferritin is < 100 ng/mL (absolute deficiency) or 100–300 ng/mL (functional deficiency, indicating iron is trapped by hepcidin) [9,10].
Reticulocyte Hemoglobin (RET-He or CHr) is now standard on most modern automated hematology analyzers, this is a highly reliable front-line marker. It reflects the actual iron available to the bone marrow over the previous 48–72 hours. It will be low in iron-restricted erythropoiesis (like ACD), providing a real-time snapshot that bypasses the acute-phase reactivity of ferritin [5].
Advanced Diagnostic Markers
When ACD and iron deficiency coexist (common in CKD, IBD, and cancer) standard iron studies become unreliable. Several extra tests help [5,6]:
- Soluble transferrin receptor (sTfR): Normal in ACD, raised in iron deficiency. Not affected by inflammation.
- sTfR/log ferritin index: A ratio under 1 suggests pure ACD. A ratio over 2 suggests iron deficiency or mixed ACD plus iron deficiency.
- Serum hepcidin: Confirms the mechanism. Still mostly a research test, although ELISA assays are increasingly used in specialist settings.
Inflammatory Markers
CRP and ESR are usually elevated. A normal CRP in suspected ACD should prompt a search for another cause.
Bone Marrow Examination (Rarely Required)
Rarely needed for ACD alone, but in difficult cases a Perl's Prussian blue stain is informative:
- In ACD: Iron is present, often increased, inside macrophages, but reduced or absent in developing red cell precursors (sideroblasts).
- In iron deficiency: Iron is absent from both macrophages and precursors.
ACD vs. Iron Deficiency Anemia
| Marker | Pure ACD | Pure Iron Deficiency Anemia | Mixed ACD + Iron Deficiency |
|---|---|---|---|
| Serum iron | Low | Low | Low |
| Ferritin | Normal or High >100 ng/mL | Low <30 ng/mL | Low-Normal 30–99 ng/mL |
| TIBC | Low or Normal | High | Normal to High |
| Transferrin Saturation (TSAT) | Normal to Low | Low <20% | Low <20% |
| sTfR | Normal | High | High |
| Marrow iron | Present in macrophages | Absent | Absent in precursors, variable in macrophages |
Differential Diagnosis
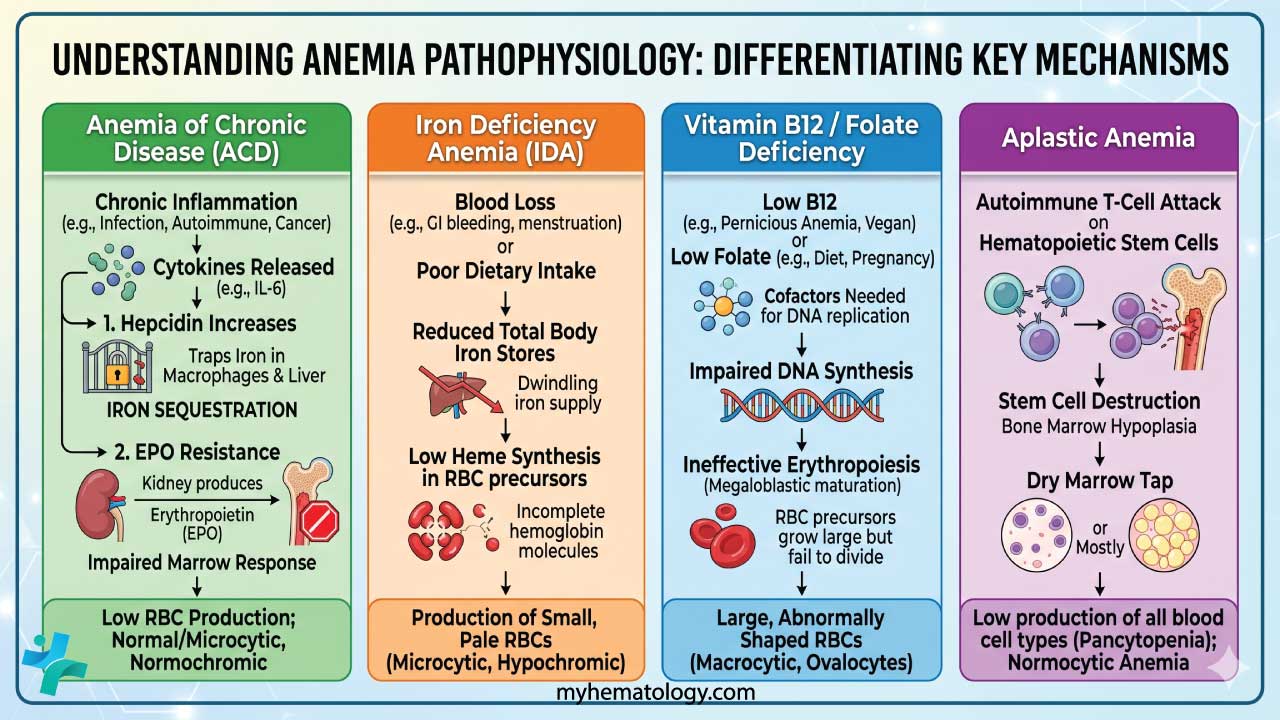
ACD's main lookalikes are iron deficiency anemia, megaloblastic anemia, and aplastic anemia.
ACD vs. Common Anemias
| Feature | ACD | Iron Deficiency Anemia | Megaloblastic (B12 / Folate) | Aplastic Anemia |
|---|---|---|---|---|
| MCV | Normocytic (can become microcytic) | Microcytic | Macrocytic (> 100 fL) | Normocytic |
| Reticulocytes | Low | Low | Low | Very low |
| Serum iron | Low | Low | Normal to high | Normal to high |
| Ferritin | Normal to high | Low | Normal to high | Normal to high |
| TIBC | Low or normal | High | Normal | Normal |
| Blood film | Usually normocytic | Hypochromic, pencil cells | Hypersegmented neutrophils, ovalocytes | Normocytic, normochromic |
| WBC & platelets | Usually normal | Usually normal | May be low in severe cases | Low (pancytopenia) |
| Bone marrow | Iron in macrophages, low sideroblasts | Absent iron stores | Megaloblastic changes | Hypocellular |
Key Differentiators
- ACD vs. iron deficiency: Ferritin and TIBC tell the story. In ACD the iron is locked in a full safe; in iron deficiency the safe is empty.
- ACD vs. B12 or folate deficiency: Megaloblastic anemias are macrocytic with hypersegmented neutrophils.
- ACD vs. aplastic anemia: Aplastic anemia comes with pancytopenia. If you see low Hb together with low white cells and low platelets and no clear inflammatory cause, a bone marrow biopsy is essential.
A patient can have more than one anemia at the same time. A patient with inflammatory bowel disease often has both ACD and iron deficiency from blood loss, which is why careful interpretation of all the iron markers matters.
Treatment and Management
Managing anemia of chronic disease is rarely about the anemia alone. The anemia is a symptom of systemic inflammation, and lasting improvement depends on calming that inflammation [3,4].
Step 1: Treat the Underlying Condition
The most effective long-term answer is to control whatever is driving the inflammation:
- Infections: Appropriate antibiotic, antiviral, or antifungal therapy.
- Autoimmune disease: Corticosteroids, disease-modifying drugs, or biologics such as TNF-α inhibitors.
- Cancer: Surgery, chemotherapy, or radiotherapy aimed at reducing tumor-driven inflammation.
As CRP and IL-6 fall, hepcidin falls with them. Iron is released, the marrow recovers, and hemoglobin tends to rise on its own.
Step 2: Iron Therapy When Indicated
Iron therapy in ACD is more nuanced than in iron deficiency anemia.
- Oral iron is usually ineffective in active ACD. High hepcidin levels block ferroportin in the gut, so the iron is absorbed into the gut lining but cannot reach the blood. Side effects such as nausea and constipation are common with little benefit [3,4].
- Intravenous (IV) iron bypasses the gut and delivers iron straight to the marrow. It is the preferred option when iron is needed and is especially useful in mixed ACD plus iron deficiency, or in functional iron deficiency where ferritin is normal but transferrin saturation is below 20% [6]. In heart failure with reduced ejection fraction and iron deficiency, the 2023 ESC guidelines recommend IV ferric carboxymaltose or ferric derisomaltose to improve symptoms and reduce hospitalizations [10]. The clinical threshold for administering IV iron has lowered significantly because newer, high-molecular-weight formulations (such as ferric carboxymaltose and ferric derisomaltose) allow for large total-dose infusions in a single 15-minute visit with an exceptionally low risk of allergic reactions compared to older dextran-based formulations [14].
Step 3: Erythropoiesis-Stimulating Agents (ESAs)
ESAs such as epoetin alfa and darbepoetin alfa help overcome both the low EPO levels and the marrow's resistance to EPO. They are most commonly used in:
- Anemia of chronic kidney disease.
- Chemotherapy-induced anemia, with shared decision-making about the risks (ASCO/ASH guidance) [11].
ESAs work best when paired with enough available iron, often IV. Without iron, the marrow tries to make red cells but cannot.
High-dose ESAs carry real risks, including thromboembolism and possible tumor progression in some cancers. The 2024 KDIGO guidelines emphasize an individualized approach rather than a one-size-fits-all target. In CKD, nephrologists generally initiate ESAs when Hb falls below 10.0 g/dL, aiming for a maintenance target of 10.0–11.5 g/dL. The primary goal is avoiding blood transfusions and alleviating severe symptoms, using the lowest possible dose to minimize Major Adverse Cardiovascular Events (MACE) [9].
Step 4: Newer Therapies — HIF-PH Inhibitors
Hypoxia-inducible factor prolyl hydroxylase (HIF-PH) inhibitors are oral drugs that stabilize HIF, raising natural EPO and lowering hepcidin at the same time [8]. They are especially promising in CKD, where they may eventually replace some uses of ESAs.
Approval is regional and worth knowing for exams and practice:
- Roxadustat: Approved in China, Japan, the EU, and the UK for CKD-related anemia. The US FDA declined approval in 2021 over cardiovascular safety concerns.
- Daprodustat: Approved by the US FDA in 2023, but only for dialysis-dependent CKD anemia.
- Vadadustat: Approved by the US FDA in 2024 for dialysis-dependent CKD anemia.
The US FDA restricted daprodustat and vadadustat strictly to dialysis-dependent patients because large clinical trials in non-dialysis patients failed to definitively show non-inferiority to ESAs regarding the risk of Major Adverse Cardiovascular Events (MACE) and thromboembolism. However, European and Asian regulatory bodies have accepted broader use with careful patient selection [15].
Step 5: Other Targeted Therapies
- Anti-IL-6 therapy (e.g., tocilizumab) blocks the upstream signal that drives hepcidin.
- Hepcidin antagonists and ferroportin stabilizers are in clinical trials and may become important options in coming years [4].
Step 6: Red Blood Cell Transfusion
Transfusion is reserved for severe symptomatic anemia, usually Hb below 7–8 g/dL, or for patients with cardiovascular compromise. It works fast but does not treat the underlying problem, and it adds risks: iron overload (especially troublesome in patients whose iron stores are already high), transfusion reactions, and alloimmunization.
Management Summary Table
| Intervention | Goal | Best For |
|---|---|---|
| Treat underlying cause | Remove the inflammatory trigger | First-line for everyone |
| IV iron | Bypass the hepcidin block | Mixed ACD plus iron deficiency, or functional iron deficiency |
| ESAs | Overcome marrow resistance and low EPO | CKD anemia, chemotherapy-induced anemia |
| HIF-PH inhibitors | Boost EPO and lower hepcidin | CKD anemia, particularly oral therapy |
| RBC transfusion | Rapid symptomatic relief | Severe symptomatic anemia or hemodynamic compromise |
Always check the sTfR/log Ferritin Index before starting iron.
If the index is low (< 1), the patient has pure ACD, and giving iron (especially oral) is unlikely to help and may cause harm through oxidative stress. Focus on the inflammation first!
Frequently Asked Questions (FAQs)
What is anemia of chronic disease in simple terms?
Anemia of chronic disease (ACD), also called anemia of inflammation, is a mild-to-moderate anemia caused by long-standing inflammation. Inflammation pushes the liver to make hepcidin, which locks iron inside storage cells. The bone marrow then cannot get enough iron to make red blood cells, even when the body has plenty in storage. It is most often seen in chronic infections, autoimmune diseases, chronic kidney disease, heart failure, and some cancers.
How do doctors tell anemia of chronic disease apart from iron deficiency anemia?
Both show low serum iron. The difference is in iron storage and transport. ACD shows normal or high ferritin and a low or normal TIBC, because iron is locked away rather than missing. Iron deficiency anemia shows low ferritin and a high TIBC, because the body genuinely lacks iron. Soluble transferrin receptor (sTfR) is normal in ACD and raised in iron deficiency. The sTfR-to-log-ferritin index is the single most reliable calculation for separating them.
Why don't iron tablets fix anemia of chronic disease?
Oral iron is usually ineffective because hepcidin is high. Hepcidin shuts down ferroportin, the protein that lets iron pass from the gut into the bloodstream. The iron is absorbed into gut cells but cannot get into circulation. Most patients with active ACD need treatment of the underlying inflammation instead, with IV iron used when iron is genuinely required.
What is the main treatment for anemia of chronic disease?
The cornerstone is treating the underlying cause: antibiotics for infection, immune-modifying drugs for autoimmune disease, or cancer treatment. As inflammation falls, hepcidin falls, iron becomes available, and hemoglobin recovers. IV iron, erythropoiesis-stimulating agents (ESAs), or newer HIF-PH inhibitors may be added in specific situations, especially in chronic kidney disease and cancer-related anemia. Transfusion is reserved for severe or symptomatic anemia.
Is anemia of chronic disease dangerous?
ACD is rarely life-threatening on its own. It tends to be mild to moderate. The risk comes from the company it keeps. In heart failure, untreated ACD worsens symptoms and hospitalization rates. In chronic kidney disease, it is linked to worse cardiovascular outcomes. The seriousness usually reflects the underlying condition more than the anemia itself.
Can children develop anemia of chronic disease?
Yes. Children with chronic infections, juvenile idiopathic arthritis, inflammatory bowel disease, or chronic kidney disease can develop ACD through the same mechanism as adults. Pediatric workups are careful to rule out iron deficiency and nutritional anemias first, because they are far more common in children and need different treatment.
Glossary of Related Medical Terms
- Anemia: A condition where the blood carries less oxygen than normal, usually from low hemoglobin or fewer red blood cells.
- Cytokines: Signaling proteins released by immune cells. IL-6 and IL-1 are the main drivers in ACD.
- Erythropoiesis: The process of making red blood cells in the bone marrow.
- Erythropoietin (EPO): A kidney hormone that tells the marrow to produce more red blood cells.
- Erythroferrone (ERFE): A hormone released by developing red blood cells that lowers hepcidin so iron is freed for use.
- Ferritin: The body's iron storage protein. High ferritin usually means plenty of stored iron.
- Ferroportin: The "door" that moves iron out of cells. Hepcidin closes this door.
- Functional iron deficiency: Plenty of iron in storage, but not available for red cell production.
- Hepcidin: A liver hormone that controls iron in the body. Inflammation raises hepcidin and blocks iron release.
- HIF-PH inhibitors: Oral drugs (roxadustat, daprodustat, vadadustat) that raise natural EPO and lower hepcidin.
- Macrophage: An immune cell that stores iron and recycles old red blood cells.
- Reticulocyte: A young red blood cell. A low count signals the marrow isn't keeping up.
- Soluble transferrin receptor (sTfR): A blood marker raised when cells lack iron. Helps separate ACD from iron deficiency.
- TIBC (total iron-binding capacity): A measure of how much iron the blood can carry on transferrin. Low in ACD, high in iron deficiency.
- Transferrin: The blood protein that carries iron to where it is needed.
- Transferrin saturation: The percentage of transferrin actually carrying iron.
References
- Madu, A. J., & Ughasoro, M. D. (2017). Anaemia of Chronic Disease: An In-Depth Review. Medical principles and practice : international journal of the Kuwait University, Health Science Centre, 26(1), 1–9. https://doi.org/10.1159/000452104
- GBD 2021 Anaemia Collaborators (2023). Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990-2021: findings from the Global Burden of Disease Study 2021. The Lancet. Haematology, 10(9), e713–e734. https://doi.org/10.1016/S2352-3026(23)00160-6
- Marques, O., Weiss, G., & Muckenthaler, M. U. (2022). The role of iron in chronic inflammatory diseases: from mechanisms to treatment options in anemia of inflammation. Blood, 140(19), 2011–2023. https://doi.org/10.1182/blood.2021013472
- Weiss, G., Ganz, T., & Goodnough, L. T. (2019). Anemia of inflammation. Blood, 133(1), 40–50. https://doi.org/10.1182/blood-2018-06-856500
- Svenson, N., Bailey, J., Durairaj, S., & Dempsey-Hibbert, N. (2021). A simplified diagnostic pathway for the differential diagnosis of iron deficiency anaemia and anaemia of chronic disease. International journal of laboratory hematology, 43(6), 1644–1652. https://doi.org/10.1111/ijlh.13666
- Wiciński, M., Liczner, G., Cadelski, K., Kołnierzak, T., Nowaczewska, M., & Malinowski, B. (2020). Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?. Nutrients, 12(6), 1784. https://doi.org/10.3390/nu12061784
- Sun, C. C., Vaja, V., Babitt, J. L., & Lin, H. Y. (2012). Targeting the hepcidin-ferroportin axis to develop new treatment strategies for anemia of chronic disease and anemia of inflammation. American journal of hematology, 87(4), 392–400. https://doi.org/10.1002/ajh.23110
- Li, Z., Shen, L., Tu, Y., Lu, S., & Liu, B. (2025). Hypoxia-inducible factor-prolyl hydroxylase inhibitors in treatment of anemia with chronic disease. Chinese medical journal, 138(12), 1424–1432. https://doi.org/10.1097/CM9.0000000000003470
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group (2024). KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney international, 105(4S), S117–S314. https://doi.org/10.1016/j.kint.2023.10.018
- McDonagh, T. A., Metra, M., Adamo, M., Gardner, R. S., Baumbach, A., Böhm, M., Burri, H., Butler, J., Čelutkienė, J., Chioncel, O., Cleland, J. G. F., Crespo-Leiro, M. G., Farmakis, D., Gilard, M., Heymans, S., Hoes, A. W., Jaarsma, T., Jankowska, E. A., Lainscak, M., Lam, C. S. P., … ESC Scientific Document Group (2023). 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European heart journal, 44(37), 3627–3639. https://doi.org/10.1093/eurheartj/ehad195
- Bohlius, J., Bohlke, K., Castelli, R., Djulbegovic, B., Lustberg, M. B., Martino, M., Mountzios, G., Peswani, N., Porter, L., Tanaka, T. N., Trifirò, G., Yang, H., & Lazo-Langner, A. (2019). Management of Cancer-Associated Anemia With Erythropoiesis-Stimulating Agents: ASCO/ASH Clinical Practice Guideline Update. Journal of clinical oncology : official journal of the American Society of Clinical Oncology, 37(15), 1336–1351. https://doi.org/10.1200/JCO.18.02142
- World Health Organization. (2024). WHO guideline on haemoglobin cutoffs to define anaemia in individuals and populations. WHO.
- Sonnweber, T., Boehm, A., Sahanic, S., Pizzini, A., Aichner, M., Sonnweber, B., Kurz, K., Koppelstätter, S., Haschka, D., Petzer, V., Hilbe, R., Theurl, M., Lehner, D., Nairz, M., Puchner, B., Luger, A., Schwabl, C., Bellmann-Weiler, R., Wöll, E., Widmann, G., … Weiss, G. (2020). Persisting alterations of iron homeostasis in COVID-19 are associated with non-resolving lung pathologies and poor patients' performance: a prospective observational cohort study. Respiratory research, 21(1), 276. https://doi.org/10.1186/s12931-020-01546-2
- Auerbach, M., & Macdougall, I. (2017). The available intravenous iron formulations: History, efficacy, and toxicology. Hemodialysis international. International Symposium on Home Hemodialysis, 21 Suppl 1, S83–S92. https://doi.org/10.1111/hdi.12560
- Singh, A. K., Carroll, K., McMurray, J. J. V., Solomon, S., Jha, V., Johansen, K. L., Lopes, R. D., Macdougall, I. C., Obrador, G. T., Waikar, S. S., Wanner, C., Wheeler, D. C., Więcek, A., Blackorby, A., Cizman, B., Cobitz, A. R., Davies, R., DiMino, T. L., Kler, L., Meadowcroft, A. M., … ASCEND-ND Study Group (2021). Daprodustat for the Treatment of Anemia in Patients Not Undergoing Dialysis. The New England journal of medicine, 385(25), 2313–2324. https://doi.org/10.1056/NEJMoa2113380