Key Takeaways
Arterial thrombosis is a blood clot that forms inside an artery, blocking oxygen-rich blood from reaching organs like the heart, brain, or limbs.
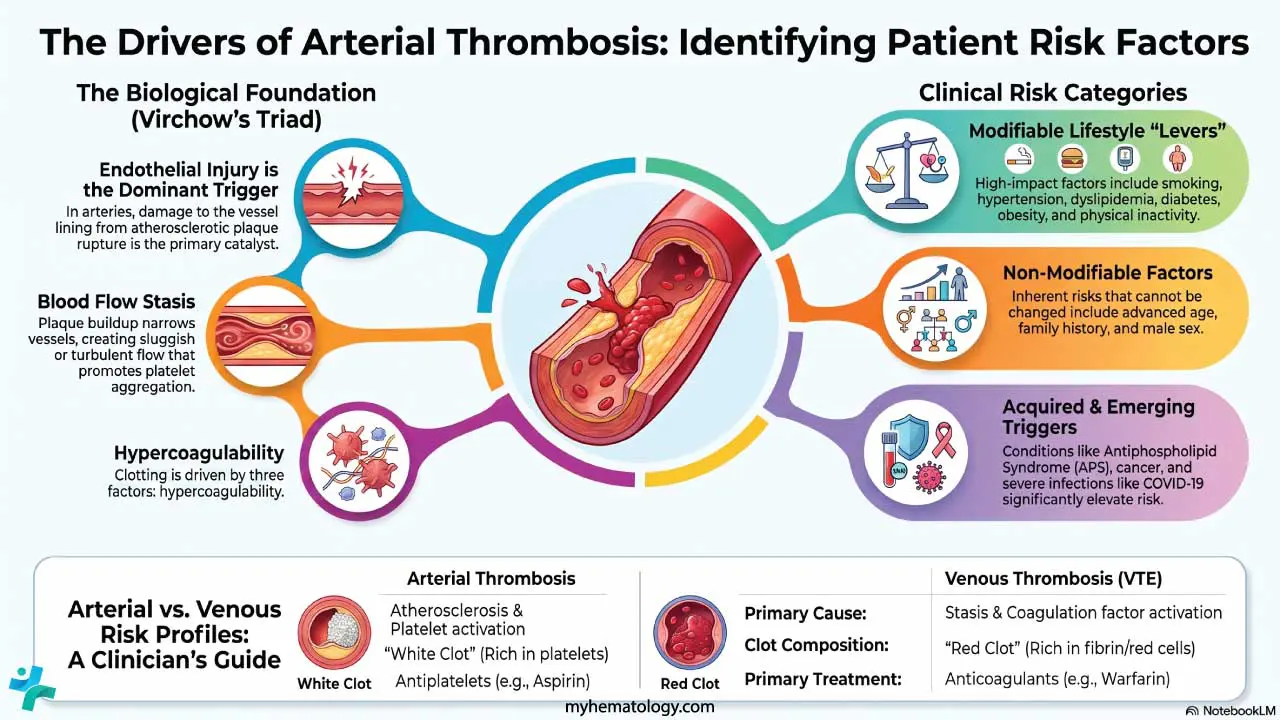
- Risk factors ▾: The three drivers of clot formation are endothelial injury, blood flow disturbance, and hypercoagulability — a framework called Virchow's Triad. In arteries, endothelial injury from atherosclerotic plaque rupture is usually the dominant trigger.
- Symptoms ▾: Common consequences of arterial thrombosis include heart attack, ischemic stroke, peripheral artery disease, and acute limb ischemia. Cardiovascular disease remains the leading global cause of death [8].
- Early diagnosis ▾: Diagnosis combines bedside assessment, imaging (Duplex ultrasound, CT angiography, catheter angiography), and laboratory workup including antiphospholipid antibody testing in unexplained cases [1].
- Treatment ▾: Treatment is time-critical. It centers on reperfusion (thrombolysis or mechanical thrombectomy), antiplatelet therapy, and aggressive secondary prevention with statins, blood pressure control, and lifestyle change [4,5].
*Click ▾ for more information
Introduction
Arterial thrombosis is the formation of a blood clot inside an artery. It blocks the delivery of oxygen-rich blood to tissues downstream, and within hours it can kill heart muscle, brain cells, or limb tissue. Heart attacks, ischemic strokes, and acute limb ischemia are all forms of arterial thrombosis presenting in different vessels.
Cardiovascular disease driven by arterial clotting is the world's leading cause of death [8]. Understanding why arterial clots form, how they differ from venous clots, and how clinicians treat them will shape how you think about patients on cardiology, neurology, and vascular wards.
This article walks through the risk factors, mechanisms, signs, investigations, and treatment of arterial thrombosis, with up-to-date guideline recommendations [4,5].
Risk Factors for Arterial Thrombosis
Most arterial thrombosis sits on top of atherosclerosis. The same factors that promote plaque formation also weaken the vessel wall and make a clot more likely once a plaque ruptures. Identifying these factors early lets clinicians counsel lifestyle change or start medication before an event occurs.
The Northwick Park Heart Study showed that elevated plasma factor VII and fibrinogen are among the strongest independent predictors of coronary events, alongside the more familiar lipid and blood pressure measures [2]. Hyperhomocysteinemia is also recognized as an independent risk factor for premature arterial disease [1].
Modifiable Risk Factors
These are the levers patients and clinicians can pull.
- Smoking: damages the endothelium, increases inflammation, and promotes clotting.
- Hypertension: stretches and injures arterial walls.
- Dyslipidemia: high LDL cholesterol and low HDL cholesterol drive plaque formation.
- Diabetes: chronic high glucose damages small and large arteries.
- Obesity: increases inflammation and metabolic strain.
- Diet: high saturated fat raises risk; fruits, vegetables, and fiber lower it.
- Physical inactivity: reduces protective vascular function.
- Chronic stress: contributes indirectly through blood pressure, inflammation, and behavior.
Non-Modifiable Risk Factors
These cannot be changed but should be recognized.
- Age: arteries lose elasticity over time.
- Family history: genetic clustering of risk factors.
- Ethnicity: risk is heavily stratified by race and ancestry. For instance, Black adults in the United States face a nearly 30% higher cardiovascular mortality rate and roughly twice the risk of a first-ever ischemic stroke compared to non-Hispanic white adults, largely driven by disproportionate rates of severe, early-onset hypertension [11]. Furthermore, people of South Asian descent account for approximately 60% of the global cardiovascular disease burden despite comprising only 25% of the population, often developing coronary artery disease up to a decade earlier than other demographics [12].
- Sex: men generally develop cardiovascular disease 7 to 10 years earlier than women; however, younger women (under 55) who experience an acute myocardial infarction face a significantly higher in-hospital mortality rate than men of the same age [11]. Women's overall risk accelerates sharply after menopause.
Acquired Risk Factors
These are conditions or exposures that emerge during life.
- Antiphospholipid syndrome and other autoimmune diseases.
- Cancer: many malignancies create a hypercoagulable state.
- Combined oral contraceptives and hormone therapy, especially in smokers.
- Trauma and surgery: damaged vessels and reduced mobility raise risk.
- COVID-19 and other severe infections: viral endothelial injury and inflammation can trigger arterial events even in younger patients [1].
Signs and Symptoms
Arterial blockage can present dramatically or quietly, depending on the vessel and the speed of occlusion. Knowing both patterns matters, because a chronic limp and a sudden stroke can stem from the same disease process.
Acute Signs
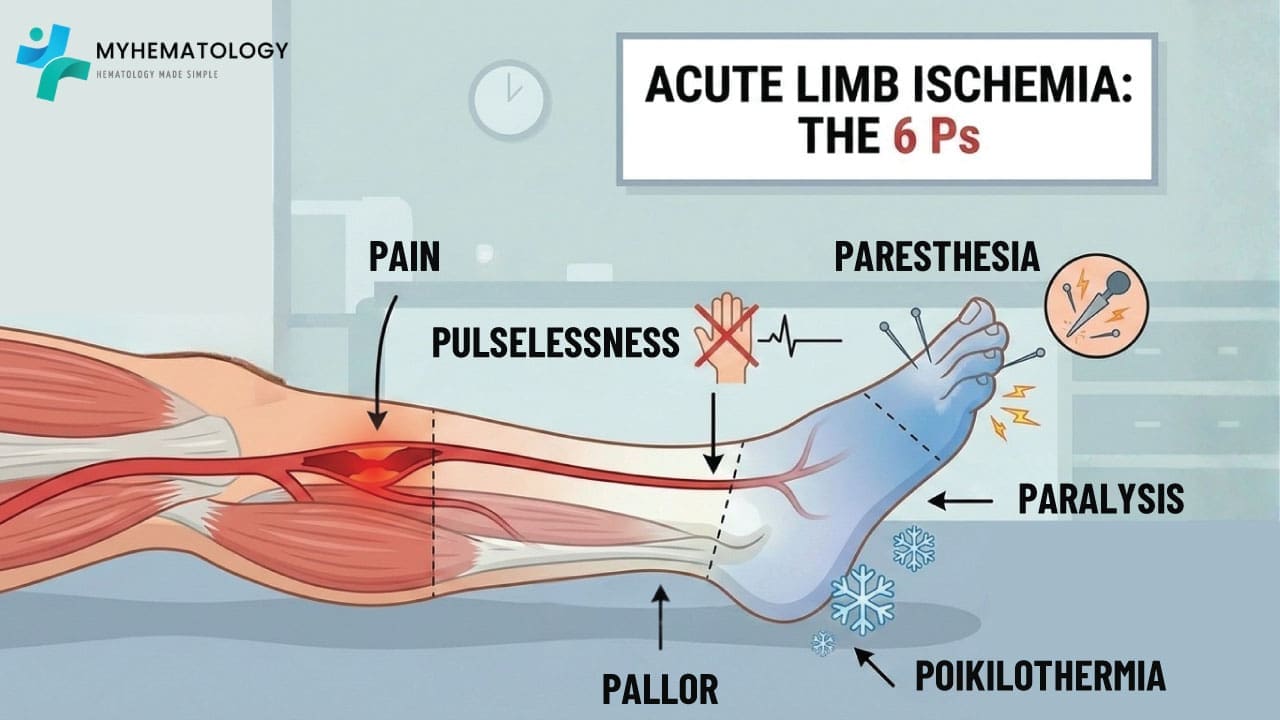
When a clot suddenly closes an artery, tissue downstream loses its oxygen supply within minutes. The classic teaching mnemonic for acute limb ischemia is the six P's:
- Pain — sudden, severe, often distal to the blockage.
- Pallor — pale, waxy skin from loss of oxygenated blood.
- Pulselessness — absent or weak pulses below the occlusion.
- Paresthesia — pins and needles or numbness from nerve ischemia.
- Paralysis — loss of motor function, signaling advanced ischemia.
- Poikilothermia — the limb cools to ambient temperature.
In other arterial beds the equivalent acute presentations are crushing chest pain (myocardial infarction), sudden focal neurological deficit (ischemic stroke), or severe abdominal pain out of proportion to exam (mesenteric ischemia). All are emergencies.
Chronic Symptoms
When a clot or plaque grows slowly, the body adapts, and symptoms creep in.
- Intermittent claudication — leg pain on walking that resolves with rest.
- Recurrent angina — chest pain on exertion in coronary artery disease.
- Coldness and color changes in the affected limb.
- Non-healing ulcers in advanced peripheral artery disease.
Chronic symptoms often look like aging or overuse until they become severe. Asking specifically about exertional pain is a high-yield clinical skill.
Virchow’s Triad
Virchow's Triad describes the three conditions that, together or in combination, allow a thrombus to form. Originally framed for venous thrombosis, the triad still applies in arteries, though the relative weights differ. In arterial disease, endothelial injury and hypercoagulability dominate; stasis plays a smaller role, mostly in atrial fibrillation, aneurysmal sacs, or behind a tight stenosis.
Endothelial Injury
The endothelium is the thin inner lining of blood vessels. A healthy endothelium actively prevents clotting. When it is damaged, it exposes underlying collagen and tissue factor, which recruit platelets and trigger the coagulation cascade.
Common causes of arterial endothelial injury:
- Atherosclerotic plaque rupture or erosion (the dominant trigger)
- Hypertension
- Smoking toxins
- High LDL cholesterol and Lp(a)
- Diabetes and chronic hyperglycemia
- Autoimmune attack (such as in systemic lupus erythematosus)
- Direct trauma or surgical injury
- Infections, including SARS-CoV-2
Blood Flow Stasis
In arteries, true stasis is uncommon but matters in specific settings. Atrial fibrillation creates stagnant blood in the left atrial appendage, which can throw a clot into the brain. Aneurysms and tight stenoses produce turbulent or sluggish flow zones where platelets can aggregate. Heart failure with low cardiac output can also contribute.
Hypercoagulability
Hypercoagulability is a state in which clotting outweighs anticoagulant defenses. Key arterial-relevant causes include:
- Antiphospholipid syndrome (APS) — the single most important hematologic cause of unexplained arterial thrombosis [1,7].
- Myeloproliferative neoplasms — JAK2-mutant polycythemia vera or essential thrombocythemia can present first with an arterial event.
- Hyperhomocysteinemia [1].
- Cancer and active inflammatory disease.
- Pregnancy and the postpartum period.
- Combined oral contraceptives, particularly in smokers.
Antiphospholipid Syndrome: A Closer Look
APS deserves its own callout. It is an autoimmune condition in which antibodies against phospholipid-binding proteins (lupus anticoagulant, anti-cardiolipin, anti-β2-glycoprotein I) drive both arterial and venous clotting [7]. A young patient with an unexplained ischemic stroke, a recurrent miscarriage, or a thrombocytopenia of unclear cause should always be screened for APS [1]. Diagnosis matters because long-term anticoagulation, not just antiplatelet therapy, may be required.
Pathophysiology of Arterial Thrombosis
The journey from a healthy artery to an occluding clot is a stepwise cascade.
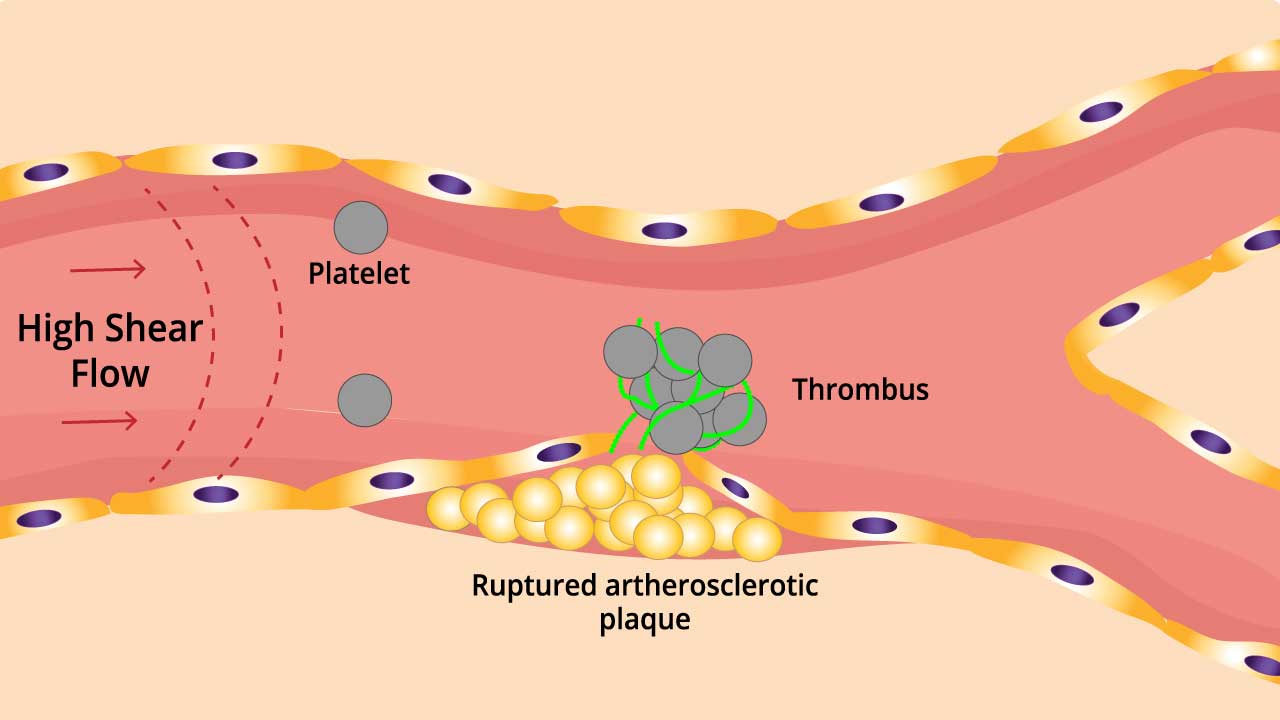
- Plaque rupture or erosion: the inciting event in most arterial thromboses. The plaque cap breaks, exposing the lipid core, collagen, and tissue factor to flowing blood.
- Platelet adhesion and activation: platelets bind to exposed collagen via von Willebrand factor and become activated, releasing ADP and thromboxane A₂. This recruits more platelets.
- Coagulation cascade: tissue factor triggers the extrinsic pathway, generating thrombin.
- Fibrin clot formation: thrombin converts fibrinogen to fibrin, which polymerizes into a mesh trapping platelets and red cells. The artery is now blocked.
Pieces of the thrombus can break off and travel as emboli, lodging in smaller distal vessels and extending the ischemic damage.
Arterial vs. Venous Thrombosis
The two share the same building blocks but assemble them differently.
Comparison
| Feature | Arterial thrombosis | Venous thrombosis (DVT/VTE) |
|---|---|---|
| Primary cause | Plaque rupture and platelet activation | Stasis and coagulation factor activation |
| Clot composition | "White clot" — platelet-rich | "Red clot" — fibrin and red-cell-rich |
| Common symptoms | The six P's (in limb ischemia); chest pain; focal neurological deficit | Swelling, redness, warmth, dull ache |
| Primary treatment | Antiplatelets (aspirin, clopidogrel, ticagrelor, prasugrel) | Anticoagulants (heparin, warfarin, DOACs) |
| Major risks | Heart attack, stroke, limb ischemia | Pulmonary embolism, post-thrombotic syndrome |
Disorders Related to Arterial Thrombosis
Different arteries blocked produce different syndromes.
- Coronary Artery Disease (CAD) and myocardial infarction: a clot in a coronary artery starves heart muscle. The result is a heart attack.
- Ischemic Stroke: a clot blocking arteries supplying the brain causes sudden focal neurological deficits — weakness, slurred speech, vision loss — depending on the territory affected.
- Peripheral Artery Disease (PAD): gradual narrowing of leg arteries causes claudication, ulcers, and in severe cases gangrene.
- Aortic Dissection: a tear in the aortic wall lets blood split between the layers; clot can form within the false lumen and worsen the obstruction [6].
- Acute Limb Ischemia: sudden blockage of an arm or leg artery, presenting with the six P's. A surgical emergency.
- Less common but important sites: renal artery stenosis (renovascular hypertension), mesenteric ischemia (acute abdominal pain), and retinal artery occlusion (sudden vision loss).
Arterial Thrombosis Investigations
Diagnosis splits into three questions: Is there a clot? What damage has it done? And why did it form?
Clinical & Bedside Assessment
Before laboratory results return, clinical signs guide the urgency:
- The six P's for acute limb ischemia.
- Ankle-Brachial Index (ABI) to quantify peripheral artery disease.
- Electrocardiogram (ECG) to detect atrial fibrillation, the leading source of cardioembolic strokes.
Diagnostic Imaging (The Gold Standard)
Imaging is required to confirm the location, extent, and nature of the thrombus.
- Duplex ultrasonography: fast, non-invasive first-line imaging combining structural and flow information.
- CT angiography (CTA): high-resolution 3D map of the arterial tree; the workhorse in emergency settings.
- MR angiography (MRA): useful when CT contrast is contraindicated or for detailed neurovascular imaging.
- Catheter-based digital subtraction angiography (DSA): still the gold standard, and it allows immediate intervention such as thrombectomy or stenting.
Core Laboratory Tests
These assess the patient’s general state and the immediate biochemical impact of the clot.
- Complete Blood Count with differential: looks for thrombocytosis, polycythemia, or leukocytosis. The neutrophil-to-lymphocyte ratio is an emerging inflammatory marker linked to adverse outcomes.
- Coagulation profile (PT, aPTT, fibrinogen, D-dimer): often normal in arterial events, but useful as a baseline.
- Markers of organ damage: troponin (heart), creatine kinase and myoglobin (skeletal muscle), LDH and AST (organ infarction).
- Metabolic panel: HbA1c, lipid profile, and lipoprotein(a) (Lp(a)) — a genetically determined cholesterol particle now recognized as an independent atherosclerotic and thrombotic risk factor.
Hematological & Etiological Workup
When an arterial event is unexplained (not clearly atherosclerotic and not cardioembolic) a deeper workup is warranted [1].
- Antiphospholipid syndrome screen: lupus anticoagulant, anti-cardiolipin (IgG/IgM), anti-β2-glycoprotein I (IgG/IgM) [7]. This is the highest-yield hematology test in unexplained arterial events.
- JAK2 V617F mutation, with CALR and MPL if JAK2 is negative, to rule out myeloproliferative neoplasms.
- Homocysteine level: elevated levels are an independent risk factor [1].
- Hereditary thrombophilia panel (Factor V Leiden, prothrombin G20210A): low-yield for arterial events but considered in young patients with no other cause.
Embolic Source Workup
If the clot looks embolic, find the source.
- Transthoracic or transesophageal echocardiogram to look for left atrial thrombi, vegetations, or a patent foramen ovale.
- Holter monitoring to catch paroxysmal atrial fibrillation.
Investigation Summary
| Category | Key investigations |
|---|---|
| Immediate diagnosis | CTA, duplex ultrasound, ABI, ECG |
| Basic hematology | CBC with NLR, PT/aPTT, fibrinogen, D-dimer |
| Atherosclerotic risk | Lipids, HbA1c, hs-CRP, Lp(a) |
| Hematology workup | APS screen, JAK2 mutation, homocysteine |
| Embolic source | TTE/TEE, Holter monitor |
| Advanced tools | TEG/ROTEM, thrombin generation, platelet aggregometry |
Treatment and Management
The management of arterial thrombosis is a race against time. Once an artery is blocked, the tissue downstream begins to die. The goal is to restore blood flow as fast as possible, then prevent the next event.
Acute Reperfusion
- Thrombolysis ("clot-busting"): drugs dissolve the fibrin mesh. The latest AHA/ASA guidelines formally recognize tenecteplase (0.25 mg/kg) as the preferred first-line thrombolytic over alteplase for eligible acute ischemic stroke patients within the 4.5-hour window, owing to its superior fibrin specificity and practical single-bolus administration [13]. Furthermore, treatment windows for mechanical thrombectomy are increasingly dictated by advanced perfusion imaging (CT perfusion or MRI) to identify salvageable penumbral tissue, extending interventions up to 24 hours (and sometimes beyond) rather than relying strictly on symptom-onset time clocks [13].
- Mechanical thrombectomy: a catheter physically removes the clot. It is now the standard for many large-vessel strokes, with the eligibility window extended up to 24 hours in selected patients with salvageable tissue [5].
- Angioplasty and stenting: a balloon crushes the underlying plaque and a mesh stent props the artery open.
- Surgical bypass: for long or complex blockages, surgeons reroute blood around the obstruction using a vein or synthetic graft.
For ST-elevation myocardial infarction, the priority is primary percutaneous coronary intervention within 90 minutes of first medical contact whenever feasible.
Pharmacological Management
Because arterial clots are platelet-rich, antiplatelet agents are the cornerstone of treatment, with anticoagulants playing a supporting role.
- Antiplatelet therapy:
- Aspirin irreversibly inhibits COX-1 and reduces thromboxane A₂.
- P2Y12 inhibitors (clopidogrel, ticagrelor, prasugrel) block ADP-mediated platelet activation.
- Dual antiplatelet therapy (DAPT) combining aspirin with a P2Y12 inhibitor is standard after acute coronary syndrome and stenting, typically for 12 months [4].
- Anticoagulation:
- Heparin (UFH or LMWH) in the acute phase to prevent clot propagation.
- Warfarin or DOACs when the source is cardioembolic (such as atrial fibrillation) or when APS is diagnosed [1,7].
- Emerging Anticoagulation (Factor XIa inhibitors): Drugs like asundexian and milvexian are actively reshaping the landscape of thrombosis prevention. By targeting Factor XIa, these agents aim to decouple thrombosis (pathological clotting) from hemostasis (normal bleeding control), potentially offering a way to prevent arterial clots with a significantly lower bleeding risk than traditional DOACs or heparin [15].
Secondary Prevention
Once the clot is gone, the work shifts to preventing the next one.
| Category | Goal / Therapy |
|---|---|
| Lipid management | High-intensity statin (e.g., atorvastatin 40–80 mg) to stabilize plaque and lower LDL, with LDL targets typically below 55 mg/dL after an event [4] |
| Blood pressure | Target generally <130/80 mmHg, often using ACE inhibitors or beta-blockers |
| Diabetes control | Tight glucose control to limit endothelial damage |
| Anti-inflammatory therapy | Low-dose colchicine 0.5 mg daily FDA-approved 2023 — reduces MI, stroke, coronary revascularization, and cardiovascular death in atherosclerotic disease [9] |
| Lipoprotein(a) management | For patients with highly elevated Lp(a) and recurrent events, emerging RNA-interference therapies (such as olpasiran or pelacarsen) target the liver to drastically reduce Lp(a) production, addressing a risk factor that standard statins cannot effectively lower [14] |
| Lifestyle | Smoking cessation, regular exercise, Mediterranean-style diet |
Frequently Asked Questions (FAQs)
How can you tell the difference between DVT and arterial thrombosis?
DVT happens in veins, usually the deep veins of the legs. It causes swelling, warmth, redness, and a dull aching pain. Arterial thrombosis happens in arteries and causes sudden severe pain, paleness, coldness, and loss of pulse in the affected area, or a stroke or heart attack depending on the vessel. Both need urgent care, but the treatments differ with anticoagulants for DVT, antiplatelets and reperfusion for arterial events.
What are the common sites of arterial thrombosis?
The most common are the coronary arteries (causing heart attack), the carotid and intracranial arteries (causing ischemic stroke), and the leg arteries (causing peripheral artery disease or acute limb ischemia). Less common but important sites include the renal arteries, the mesenteric arteries supplying the intestines, and the retinal arteries.
What are the six P's of arterial thrombosis?
The six P's describe acute limb ischemia: Pain, Pallor, Pulselessness, Paresthesia, Paralysis, and Poikilothermia (coldness). Together they signal a critical loss of arterial flow to a limb and demand emergency assessment.
Why is aspirin used in arterial thrombosis?
Aspirin irreversibly blocks COX-1 in platelets, preventing them from releasing thromboxane A₂ and clumping. Because arterial clots are platelet-rich, aspirin is highly effective at reducing recurrence. It increases bleeding risk, so it should be taken only under medical advice [4].
How long do you take anticoagulants for arterial thrombosis?
Duration depends on the cause. After cardioembolic stroke from atrial fibrillation, anticoagulation is usually long-term. After unexplained arterial thrombosis with confirmed antiphospholipid syndrome, it may be lifelong [7]. After standard atherosclerotic events, antiplatelet therapy is preferred over anticoagulation, with DAPT typically continued for 12 months after coronary intervention [4].
Is arterial thrombosis curable?
The clot itself can be removed, dissolved, or bypassed. The underlying disease such as atherosclerosis, APS, atrial fibrillation, hypercoagulability is usually a chronic condition that needs ongoing control. With modern reperfusion, antiplatelets, statins, and lifestyle change, recurrence rates have fallen substantially [4,8].
What is the difference between a thrombus and an embolus?
A thrombus is a clot that forms and stays where it formed. An embolus is a clot (or other particle) that breaks off and travels through the bloodstream until it gets stuck in a smaller vessel. A clot in the left atrium is a thrombus; the same clot once it travels to the brain and lodges in a cerebral artery is an embolus.
Can COVID-19 cause arterial thrombosis?
Yes. SARS-CoV-2 infects vascular endothelium and triggers severe inflammation, increasing both venous and arterial clot risk. Strokes and heart attacks have been reported in younger patients during and after acute COVID-19, even without traditional risk factors [1].
Is arterial thrombosis hereditary?
The clot itself is not inherited, but several risk-amplifying conditions are. Familial hypercholesterolemia, elevated Lp(a), inherited hypertension, and certain thrombophilias all run in families [1]. A strong family history of early heart attack or stroke warrants closer screening.
What is the "golden hour" in treating arterial thrombosis?
This is the principle that the sooner blood flow is restored, the less tissue dies. For ischemic stroke, every minute of delay corresponds to roughly two million neurons lost, which is why the 2026 AHA/ASA guidelines emphasize giving thrombolysis as fast as possible within the eligible window [5]. For STEMI, the target is primary PCI within 90 minutes of first medical contact [4].
Glossary of Related Medical Terms
- Anticoagulant: a drug that slows clotting by interfering with clotting factors (heparin, warfarin, DOACs).
- Antiphospholipid syndrome (APS): an autoimmune disease in which antibodies against phospholipid-binding proteins drive arterial and venous clotting.
- Antiplatelet: a drug that prevents platelets from sticking together (aspirin, clopidogrel).
- Atherosclerosis: a buildup of fatty plaque inside artery walls that narrows the vessel and can rupture.
- Claudication: cramping leg pain that comes on with walking and resolves with rest.
- Embolus: a clot or particle that breaks off and travels through the bloodstream to block another vessel.
- Endothelium: the thin inner lining of blood vessels.
- Hypercoagulability: a state in which blood clots more readily than normal.
- Infarction: tissue death caused by loss of blood supply.
- Ischemia: reduced blood supply to a tissue.
- Lipoprotein(a) (Lp(a)): a cholesterol-carrying particle that increases atherosclerosis and arterial thrombosis risk.
- Mechanical thrombectomy: catheter-based physical removal of a clot.
- Plaque rupture: a break in an atherosclerotic plaque cap that exposes thrombogenic material.
- Reperfusion: restoring blood flow to a tissue after an obstruction is removed.
- Stenosis: narrowing of a blood vessel.
- Thrombolysis: drug-based dissolving of clots ("clot-busting").
- Thrombus: a clot that forms and stays in one place inside a vessel.
- Tissue factor: a protein released by injured or activated cells that triggers the extrinsic coagulation pathway.
- Virchow's Triad: the three pillars of clot formation — endothelial injury, blood flow stasis, hypercoagulability.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- May, J. E., & Moll, S. (2020). How I treat unexplained arterial thrombosis. Blood, 136(13), 1487–1498. https://doi.org/10.1182/blood.2019000820
- Ten Cate, H., & Meade, T. (2014). The Northwick Park Heart Study: evidence from the laboratory. Journal of thrombosis and haemostasis : JTH, 12(5), 587–592. https://doi.org/10.1111/jth.12545
- Bhatt, D. L., Lopes, R. D., & Harrington, R. A. (2022). Diagnosis and Treatment of Acute Coronary Syndromes: A Review. JAMA, 327(7), 662–675. https://doi.org/10.1001/jama.2022.0358
- Byrne, R. A., Rossello, X., Coughlan, J. J., Barbato, E., Berry, C., Chieffo, A., Claeys, M. J., Dan, G. A., Dweck, M. R., Galbraith, M., Gilard, M., Hinterbuchner, L., Jankowska, E. A., Jüni, P., Kimura, T., Kunadian, V., Leosdottir, M., Lorusso, R., Pedretti, R. F. E., Rigopoulos, A. G., … ESC Scientific Document Group (2023). 2023 ESC Guidelines for the management of acute coronary syndromes. European heart journal, 44(38), 3720–3826. https://doi.org/10.1093/eurheartj/ehad191
- Prabhakaran, S., Gonzalez, N. R., Zachrison, K. S., Adeoye, O., Alexandrov, A. W., Ansari, S. A., Chapman, S., Czap, A. L., Dumitrascu, O. M., Ishida, K., Jadhav, A. P., Johnson, B., Johnston, K. C., Khatri, P., Kimberly, W. T., Lee, V. H., Leslie-Mazwi, T. M., Mac Grory, B., Madsen, T. E., Menon, B., … Peer Review Committee (2026). 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association. Stroke, 10.1161/STR.0000000000000513. Advance online publication. https://doi.org/10.1161/STR.0000000000000513
- Tadros, R. O., Tang, G. H. L., Barnes, H. J., Mousavi, I., Kovacic, J. C., Faries, P., Olin, J. W., Marin, M. L., & Adams, D. H. (2019). Optimal Treatment of Uncomplicated Type B Aortic Dissection: JACC Review Topic of the Week. Journal of the American College of Cardiology, 74(11), 1494–1504. https://doi.org/10.1016/j.jacc.2019.07.063
- Garcia, D., & Erkan, D. (2018). Diagnosis and Management of the Antiphospholipid Syndrome. The New England journal of medicine, 378(21), 2010–2021. https://doi.org/10.1056/NEJMra1705454
- Tsao, C. W., Aday, A. W., Almarzooq, Z. I., Anderson, C. A. M., Arora, P., Avery, C. L., Baker-Smith, C. M., Beaton, A. Z., Boehme, A. K., Buxton, A. E., Commodore-Mensah, Y., Elkind, M. S. V., Evenson, K. R., Eze-Nliam, C., Fugar, S., Generoso, G., Heard, D. G., Hiremath, S., Ho, J. E., Kalani, R., … American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee (2023). Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation, 147(8), e93–e621. https://doi.org/10.1161/CIR.0000000000001123
- Nelson, K., Fuster, V., & Ridker, P. M. (2023). Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease: JACC Review Topic of the Week. Journal of the American College of Cardiology, 82(7), 648–660. https://doi.org/10.1016/j.jacc.2023.05.055
- Tsivgoulis, G., Katsanos, A. H., Sandset, E. C., Turc, G., Nguyen, T. N., Bivard, A., Fischer, U., & Khatri, P. (2023). Thrombolysis for acute ischaemic stroke: current status and future perspectives. The Lancet. Neurology, 22(5), 418–429. https://doi.org/10.1016/S1474-4422(22)00519-1
- Martin, S. S., Aday, A. W., Almarzooq, Z. I., Anderson, C. A. M., Arora, P., Avery, C. L., Baker-Smith, C. M., Barone Gibbs, B., Beaton, A. Z., Boehme, A. K., Commodore-Mensah, Y., Currie, M. E., Elkind, M. S. V., Evenson, K. R., Generoso, G., Heard, D. G., Hiremath, S., Johansen, M. C., Kalani, R., Kazi, D. S., … American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee (2024). 2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation, 149(8), e347–e913. https://doi.org/10.1161/CIR.0000000000001209
- Volgman, A. S., Palaniappan, L. S., Aggarwal, N. T., Gupta, M., Khandelwal, A., Krishnan, A. V., Lichtman, J. H., Mehta, L. S., Patel, H. N., Shah, K. S., Shah, S. H., Watson, K. E., & American Heart Association Council on Epidemiology and Prevention; Cardiovascular Disease and Stroke in Women and Special Populations Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Stroke Council (2018). Atherosclerotic Cardiovascular Disease in South Asians in the United States: Epidemiology, Risk Factors, and Treatments: A Scientific Statement From the American Heart Association. Circulation, 138(1), e1–e34. https://doi.org/10.1161/CIR.0000000000000580
- Potla, N., & Ganti, L. (2022). Tenecteplase vs. alteplase for acute ischemic stroke: a systematic review. International journal of emergency medicine, 15(1), 1. https://doi.org/10.1186/s12245-021-00399-w
- O'Donoghue, M. L., Rosenson, R. S., Gencer, B., López, J. A. G., Lepor, N. E., Baum, S. J., Stout, E., Gaudet, D., Knusel, B., Kuder, J. F., Ran, X., Murphy, S. A., Wang, H., Wu, Y., Kassahun, H., Sabatine, M. S., & OCEAN(a)-DOSE Trial Investigators (2022). Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease. The New England journal of medicine, 387(20), 1855–1864. https://doi.org/10.1056/NEJMoa2211023
- Hsu, C., Hutt, E., Bloomfield, D. M., Gailani, D., & Weitz, J. I. (2021). Factor XI Inhibition to Uncouple Thrombosis From Hemostasis: JACC Review Topic of the Week. Journal of the American College of Cardiology, 78(6), 625–631. https://doi.org/10.1016/j.jacc.2021.06.010