Key Takeaways
The ABO blood group is the most clinically important blood group system in transfusion and organ transplantation. A mismatch can trigger acute intravascular hemolysis, kidney failure, and death within minutes.
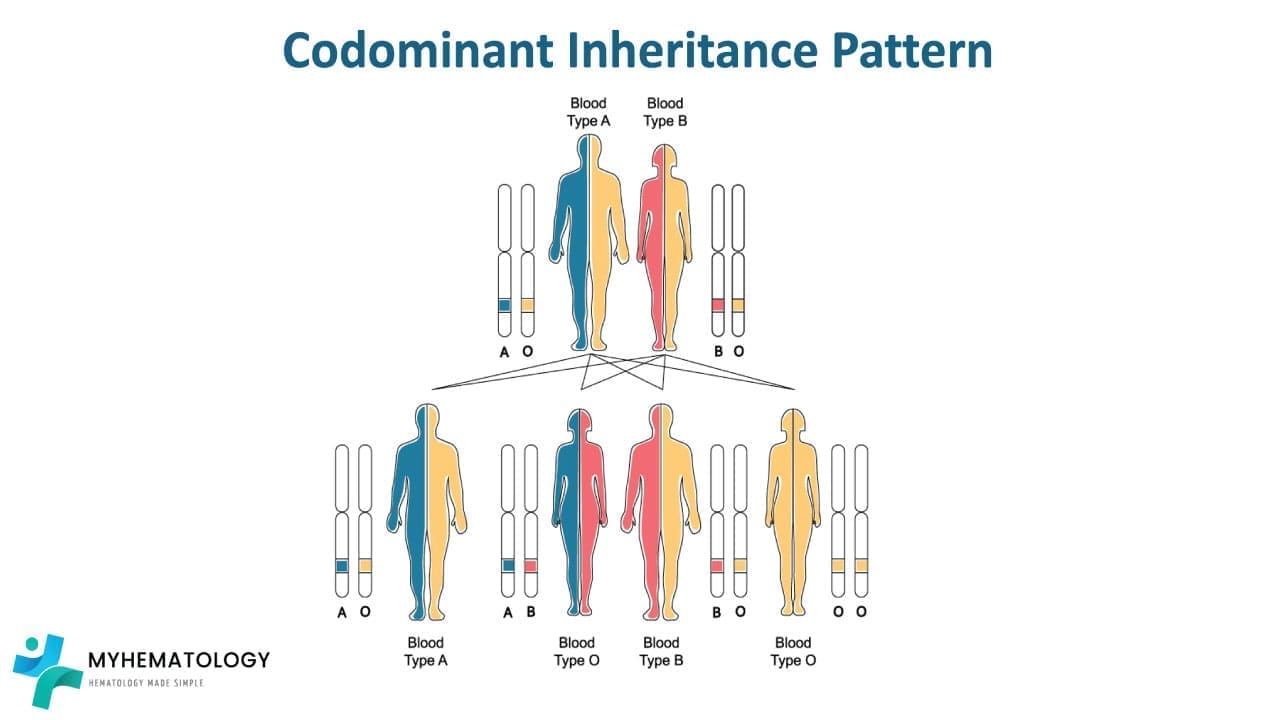
- Three antigens define the system: A, B, and the H antigen (the precursor on which A and B are built). The ABO gene on chromosome 9q34.2 has three alleles: A, B, and O. A and B are codominant; O is recessive.
- People naturally produce antibodies against the ABO antigens they lack. These "naturally occurring" anti-A and anti-B antibodies appear in the first months of life from environmental exposure to similar bacterial sugars [3].
- Blood typing uses forward typing (testing red cells with anti-A and anti-B sera) and reverse typing (testing plasma against known A and B cells). The three common methods are tile, tube, and gel card [2].
- Type O red cells are the universal red cell donor; type AB is the universal red cell recipient. For plasma the rule flips with AB is the universal plasma donor.
What the ABO Blood Group System Is
The ABO blood group is the most clinically important way we classify human blood. It decides who can safely receive whose red cells, who can donate plasma to whom, and who can receive a transplanted organ from whom. A small mismatch in ABO during transfusion can destroy the donor red cells almost immediately, leading to kidney failure, shock, and death [2].
That is why every patient before surgery, every pregnant woman at booking, and every transplant candidate gets an ABO blood group test. The system reaches well beyond red cells, too. ABO antigens sit on white cells, platelets, kidney tubules, heart endothelium, lung tissue, the gut lining, and pancreas. So an ABO mismatch is a problem for organ transplantation as well as transfusion [3].
This article walks through how the system was discovered, how the antigens are built, how they are inherited, how laboratories test for them, and how all of that translates into safer transfusions and transplants.
A Brief History of the ABO Discovery
In 1900, Austrian physician Karl Landsteiner mixed blood samples from his colleagues and noticed something strange. Some pairs clumped when combined; others did not. He worked out that red cells carry different antigens on their surface, and that the plasma of each person carries antibodies against the antigens they themselves lack. He named the antigens A, B, and C. C was later renamed O, from the German "Ohne" meaning "without" [1].
Before Landsteiner's discovery, blood transfusion was often fatal because no one understood why some pairings clumped. His work made matched transfusion possible. He received the Nobel Prize in Physiology or Medicine in 1930.
A short and accurate timeline of the early discoveries:
- 1900: Landsteiner describes the ABO system.
- 1902: Von Decastello and Sturli (his colleagues) describe the fourth blood group, AB.
- 1939–1940: Levine and Stetson, then Landsteiner and Wiener, describe the Rh system.
- 1946: Coombs, Mourant, and Race describe the Kell system, named after Mrs. Kelleher [7].
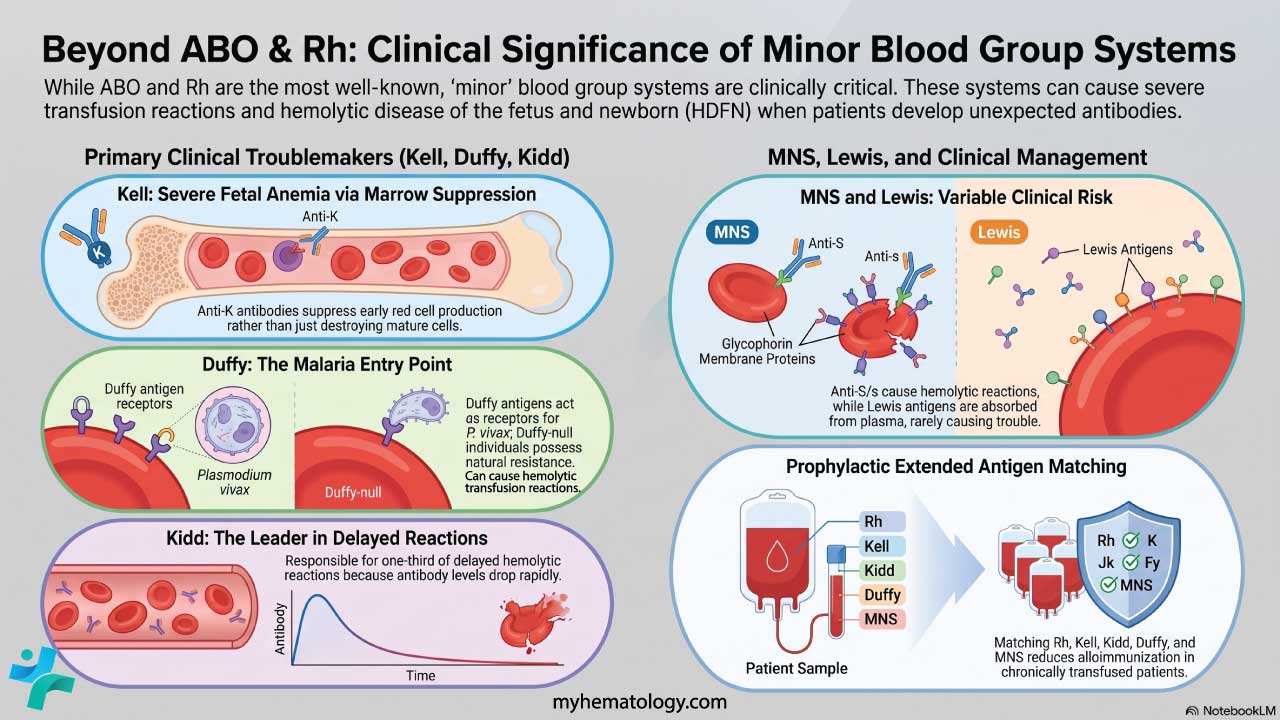
As of late 2023, the International Society of Blood Transfusion (ISBT) officially recognizes 45 distinct blood group systems (comprising over 360 individual red cell antigens). ABO and Rh remain the two most clinically important [6,9].
How ABO Antigens Are Built
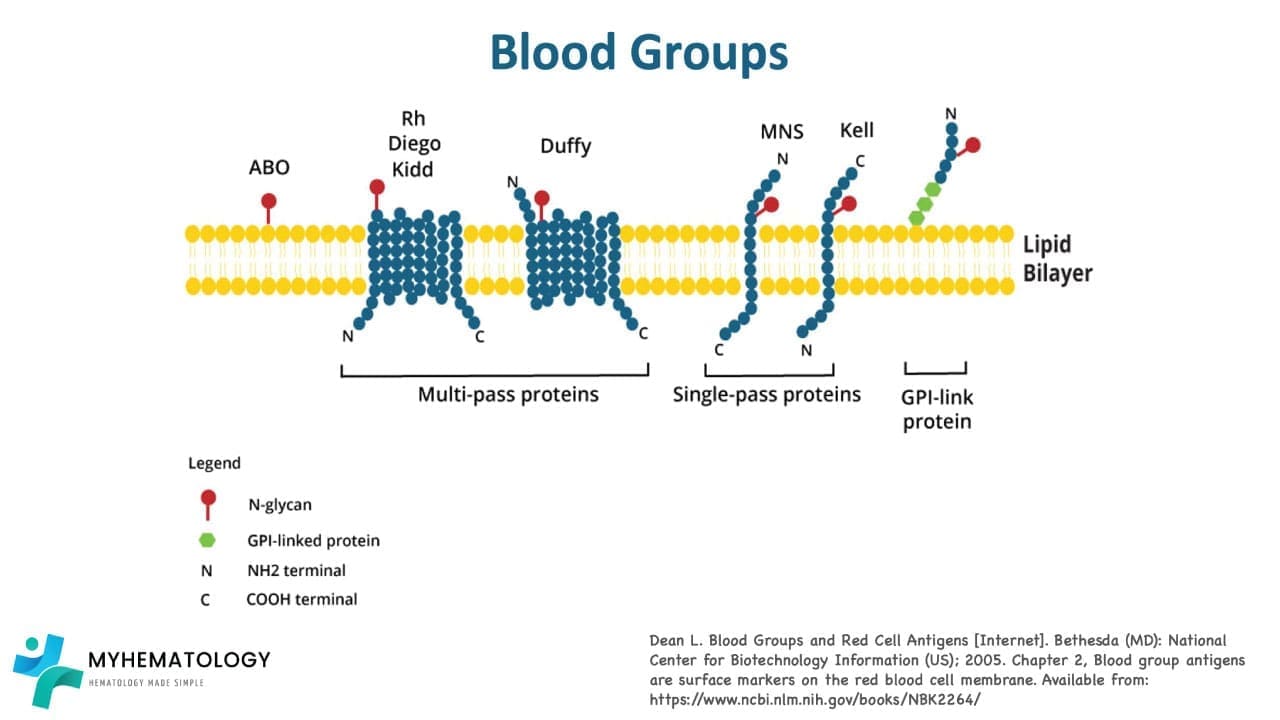
ABO antigens are not whole proteins. They are short chains of sugar molecules — oligosaccharides (short sugar chains) — attached to glycoproteins and glycolipids on the red cell membrane. The exact sugar at the end of the chain determines whether you are A, B, AB, or O.
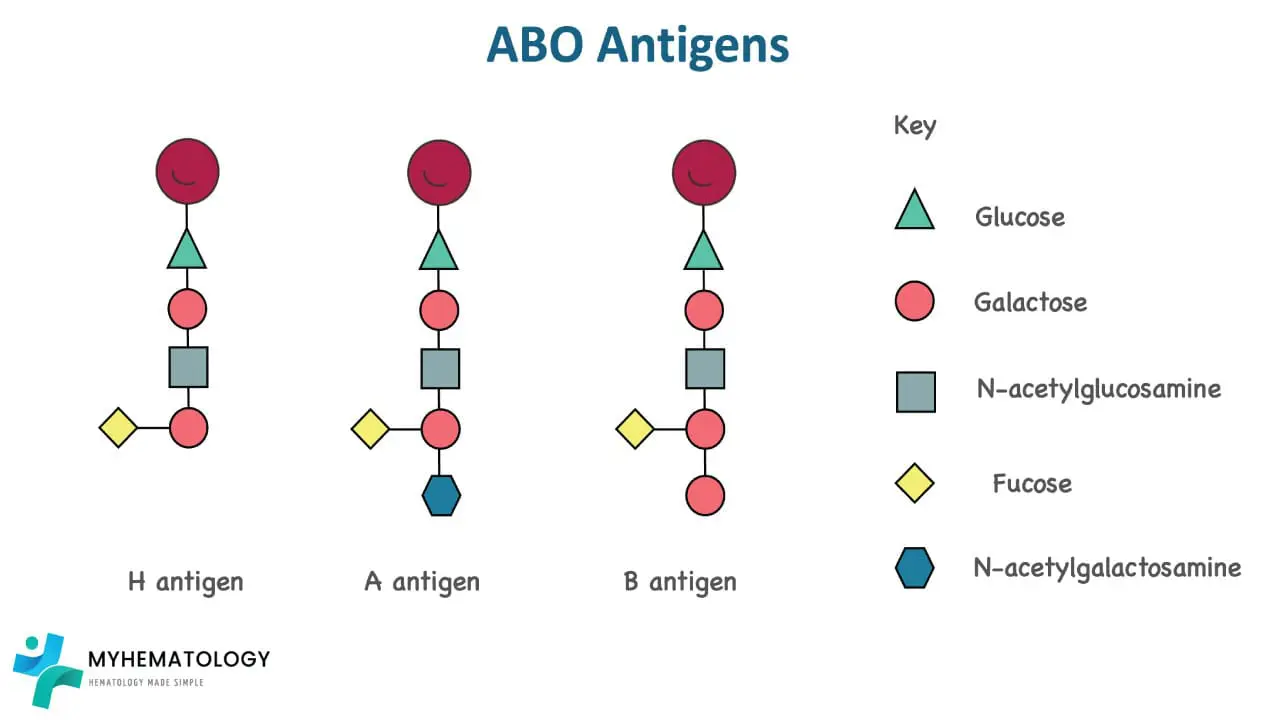
Every ABO antigen is built on the same starting platform: the H antigen. The H antigen is itself a small sugar structure, finished by an enzyme called α-1,2-fucosyltransferase (encoded by the FUT1 gene on red cells). Once the H antigen is in place:
- The A allele codes for an enzyme that adds an N-acetylgalactosamine sugar to H, producing the A antigen.
- The B allele codes for an enzyme that adds a galactose sugar to H, producing the B antigen.
- The O allele codes for a non-functional enzyme. Nothing is added, so the H antigen stays bare. People with two O alleles are blood group O [1,2].
The ABO antigens, designated as A, B, and O, are composed of oligosaccharides, complex carbohydrate structures attached to the surface of red blood cells. Their distinctive molecular configurations arise from subtle variations in the arrangement of these carbohydrate chains.
| ABO Allele | Enzyme Produced | Final Antigen on RBC | Blood Group |
|---|---|---|---|
| A | A glycosyltransferase | A antigen | A |
| B | B glycosyltransferase | B antigen | B |
| O | Non-functional | H antigen only (unmodified) | O |
So group O people are not "antigen-less." They carry the H antigen and in fact, more H antigen than any other group, because nothing has been added on top of it.
Naturally Occurring Antibodies
The ABO system is unusual. In most blood group systems, you only make antibodies after exposure to foreign cells, through transfusion or pregnancy. In the ABO system, antibodies appear within the first few months of life without a known transfusion or pregnancy. They are called naturally occurring antibodies [1].
Why? Because environmental bacteria carry sugars that look very similar to A and B antigens. The infant immune system reacts against the ones it does not see on its own cells. So:
- Group A people make anti-B.
- Group B people make anti-A.
- Group AB people make neither.
- Group O people make both anti-A and anti-B.
This pattern is Landsteiner's law: for whichever ABO antigen you lack, you carry the matching antibody in your plasma. ABO antibodies are usually IgM, but a portion can be IgG, which matters in pregnancy (see HDFN below) [3].
How the ABO Blood Group Is Inherited
The ABO gene sits on chromosome 9 at band 9q34.2 and has seven exons. It has three alleles — A, B, and O. A and B are codominant (both expressed when present together), and O is recessive (only expressed when both copies are O).
Some A and B alleles produce weaker expression of the antigen. These are called subgroups (A1, A2, B1, B2, and rarer ones) and reflect variable expressivity of the gene rather than incomplete penetrance.
ABO Blood Group Genetics
| Parent 1 genotype | Parent 2 genotype | Possible offspring blood groups |
|---|---|---|
| AA or AO | AA or AO |
A
O
|
| AA or AO | BB or BO |
A
B
AB
O
|
| AA or AO | OO |
A
O
|
| BB or BO | BB or BO |
B
O
|
| BB or BO | OO |
B
O
|
| OO | OO |
O
|
| AB | AA or AO |
A
B
AB
|
| AB | BB or BO |
A
B
AB
|
| AB | OO |
A
B
|
| AB | AB |
A
B
AB
|
Genotype notation: uppercase letters = dominant alleles (A, B); O = recessive allele.
This pattern is why a child can occasionally appear to have a blood group "neither parent has" — for example, two parents who are both heterozygous (AO and BO) can have an O child.
Global and Demographic Distribution of ABO Types
Blood group frequencies are not evenly distributed globally. Because ABO distribution varies significantly by geography and evolutionary migration, understanding these demographics is essential for managing regional blood bank supplies. Group O is universally the most common, but Group B is significantly more prevalent in Asian and African populations compared to Caucasian and Hispanic populations. Group AB remains the rarest across all demographics.
The approximate distribution of ABO blood types across different racial and ethnic groups in the United States is as follows [10]:
| Blood Group |
Approximate Frequency by Ethnic Group | |||
|---|---|---|---|---|
| Caucasian | African American | Hispanic | Asian | |
| O |
45%
|
51%
|
57%
|
40%
|
| A |
40%
|
26%
|
31%
|
28%
|
| B |
11%
|
19%
|
10%
|
27%
|
| AB |
4%
|
4%
|
2%
|
5%
|
A and B blood subgroups
Not every A is the same A. Subgroups arise from mutations that change how much antigen the enzyme can make.
Common subgroups of A: A1 (the strongest, most common form) and A2 (weaker antigen, present in roughly 20% of group A individuals). Rare forms include A3, Ax, Am, Ay, Ael, and Aend.
Common subgroups of B: B1, B2, and rare forms B3, Bx, Bm, By, Bel, and Bend.
Why subgroups matter clinically:
- Weak reactions in typing. A2 or B2 cells may give faint reactions with anti-A or anti-B, leading to mistyping if the technician is not careful.
- Mixed-field appearance. Some subgroups give a salt-and-pepper pattern — some cells reacting, others not.
- Forward–reverse mismatch. A person's red cells may type as one group while their plasma antibodies suggest another. Resolving these discrepancies often requires molecular typing or absorption-elution testing.
There is also an interesting clinical scenario called the acquired B phenotype, where bacterial enzymes in conditions like colorectal cancer or bowel obstruction transiently modify the A antigen so that a true group A patient appears to be AB. It resolves once the underlying disease is treated.
Understanding Secretor Status: The FUT2 Gene
About 80% of people also carry ABO antigens floating freely in their saliva, tears, sweat, and digestive fluids. These people are called secretors. The other 20% are non-secretors.
The difference comes from a related gene called FUT2 (the Se gene). FUT2 makes the same kind of fucosyltransferase enzyme as FUT1, but it works in glandular tissues rather than red cells. If you have at least one working copy (genotype SeSe or Sese), you secrete H, A, and/or B substances in your fluids. If both copies are non-functional (sese), you secrete none even though your red cells still express your normal ABO type [3].
Why does secretor status matter?
- Forensic identification. Before DNA profiling, secretor status let investigators determine ABO type from saliva on a cigarette, an envelope, or a sweat stain.
- Norovirus susceptibility. Norovirus uses ABO-related sugars on the gut lining as a docking site. Non-secretors are partially or fully resistant to many norovirus strains.
- Helicobacter pylori and ulcer risk. Secretor status influences how easily H. pylori sticks to the stomach lining and may change peptic ulcer risk.
- Resolving difficult ABO typing. If a typing result is ambiguous, saliva testing can sometimes confirm the group but only in secretors.
The Bombay Phenotype (Oh)
In 1952, in what was then Bombay (now Mumbai), Dr. Y.M. Bhende described patients whose blood typed as O but who suffered severe hemolytic reactions when given any type O blood. He had discovered the Bombay phenotype, present in roughly 1 in 10,000 people in India and around 1 in a million in Europe.
Bombay individuals inherit two non-functional FUT1 alleles (genotype hh). They cannot make the H antigen — the foundation A and B are built on. So even if they carry an A or B allele, they have nowhere to attach the A or B sugars.
Two consequences follow:
- In forward typing they look like O. No A, no B, no H. So anti-A and anti-B reagents do not react.
- Their plasma contains anti-A, anti-B, and a powerful anti-H. Because they have never seen the H antigen, they make potent IgM anti-H that reacts at body temperature. This anti-H attacks every ordinary ABO type (A, B, AB, and regular O) because all of those carry H.
The clinical consequence is severe: a Bombay person can only receive blood from another Bombay person. Misidentifying them as type O is a life-threatening error.
| Type O | Bombay (Oh) | |
|---|---|---|
| Genotype | OO with HH or Hh | Any ABO genotype with hh |
| H Antigen on RBCs | Present Highest amount of any ABO group | Absent |
| Forward Type Result | O | Looks like O (phenotypic mimicry) |
| Plasma Antibodies | Anti-A, Anti-B | Anti-A, Anti-B + Anti-H |
| Compatible Donors | Any Type O | Only other Bombay |
| Secretor Status | Variable | Always non-secretor |
A milder variant called Para-Bombay has a partial FUT1 defect plus a working FUT2. Tiny amounts of H substance circulate in plasma and adsorb onto red cells, giving very weak A, B, or H expression. Para-Bombay individuals usually have a weaker anti-H and may tolerate carefully matched ABO blood, but they still need specialized testing.
How Laboratories Determine the ABO Blood Group
Two complementary tests run together:
Forward typing detects antigens on the patient's red cells. A drop of patient blood is mixed with anti-A serum and, separately, with anti-B serum. Clumping means the matching antigen is present.
Reverse typing detects antibodies in the patient's plasma. A drop of patient plasma is mixed with known A red cells and, separately, with known B red cells. Clumping means the matching antibody is present.
A correct result requires the two halves to agree. A patient whose cells type as group A should have anti-B, and only anti-B, in their plasma.
Three main techniques are used.
| Method | How It Works | Strengths | Weaknesses |
|---|---|---|---|
| Tile (Slide) Field Use | Mix blood with anti-A and anti-B on a glass slide; observe for clumping. | Cheap Fast Field-suitable | Subjective Drying artifacts Less sensitive |
| Tube Clinical Standard | Mix in tubes, incubate at 37 °C, centrifuge, then observe for agglutination. | More accurate Clinical standard | Slower More labor |
| Gel Card Modern | Patient cells/plasma layered in antibody-pre-loaded gel; centrifugation traps agglutinated cells at the top. | Rapid Sensitive Easy to read Standardized | Higher reagent cost |
When forward and reverse typing disagree, additional tests resolve the discrepancy:
- Molecular typing (PCR-based ABO genotyping) for genetic variants and weak alleles.
- Absorption-elution to detect very weakly expressed antigens.
- Saliva neutralization to identify secretor-status–related variants.
In the modern blood bank, ABO typing is just the first step of pre-transfusion testing. Patients also undergo a type and screen (ABO/Rh plus an antibody screen for clinically significant non-ABO antibodies). If transfusion is needed, a crossmatch confirms compatibility with specific donor units, performed either as a serological tube or gel test, or for patients with a clean antibody screen, as an electronic crossmatch where a computer matches ABO/Rh records.
Transfusion Compatibility
The transfusion principle is simple: the recipient's antibodies must not have a target on the donor's cells. When that rule is broken, the result is acute hemolytic transfusion reaction (AHTR), in which donor red cells are destroyed inside blood vessels. AHTR can cause disseminated intravascular coagulation, kidney failure, and death [2].
Because red cell transfusions and plasma transfusions move opposite "ingredients" (cells vs. plasma), the compatibility rules flip between them.
Rule 1: Red Cell Transfusion
Worry about the recipient's antibodies attacking donor red cell antigens.
Transfusion Medicine
| Recipient | Compatible Donor RBCs | Preferred Order |
|---|---|---|
|
A
A
|
A
O
|
A
then
O
|
|
B
B
|
B
O
|
B
then
O
|
|
AB
AB
|
A
B
AB
O
|
AB
then
A or B
then
O
|
|
O
O
|
O
|
O only
|
- Universal red cell donor: O negative. O cells have no A or B antigens, so the recipient's anti-A and anti-B have nothing to attack.
- Universal red cell recipient: AB. AB people have neither anti-A nor anti-B, so they tolerate any ABO type.
In trauma, low-titer group O whole blood (LTOWB) is increasingly used as a single product for massive hemorrhage, given before formal type-and-screen results are available.
Rule 2: Plasma Transfusion (Fresh Frozen Plasma)
Now worry about the donor's antibodies attacking the recipient's red cell antigens.
- Universal plasma donor: AB. AB plasma contains neither anti-A nor anti-B, so it cannot attack any recipient's red cells.
- Universal plasma recipient: O. O recipients have no A or B antigens for any donor antibody to bind.
The ABO Blood Group Beyond Transfusion
The ABO blood group is more than a transfusion compatibility code. It influences several health outcomes [3,4]:
- Venous thromboembolism. Non-O blood groups are associated with about 25–30% higher levels of von Willebrand factor and Factor VIII, and a roughly two-fold higher risk of deep vein thrombosis and pulmonary embolism compared with group O.
- Cardiovascular disease. Non-O blood groups carry a small increased risk of coronary artery disease and ischemic stroke, partly via the same coagulation factor effect.
- Cancer. Group A has been linked to modestly higher risks of pancreatic and gastric cancer.
- Infectious disease. During the COVID-19 pandemic, several large studies and meta-analyses reported group A had higher risk of severe disease and group O had lower risk, although the absolute effect was small. It must be emphasized that the absolute risk difference is negligible at the individual level; confounding factors such as age, socioeconomic status, and underlying comorbidities heavily dwarf the impact of a patient's ABO group on infectious disease outcomes [11].
These associations do not change individual clinical management. Your blood group is not a reason to change your lifestyle.
Hemolytic Disease of the Fetus and Newborn (HDFN)
ABO-HDFN typically occurs when a group O mother carries a group A or B fetus. Group O mothers, unlike A or B mothers, can produce IgG anti-A and anti-B in addition to IgM. IgG crosses the placenta and can attach to fetal red cells, causing hemolysis, anemia, and jaundice in the newborn [3].
The good news: ABO-HDFN is usually mild, much milder than Rh-HDFN, because fetal A and B antigens are not yet fully developed and are also expressed widely on other tissues, "soaking up" maternal antibodies. Most cases are managed with phototherapy.
ABO-Incompatible Solid Organ Transplantation
For decades, an ABO mismatch between donor and recipient was considered an absolute contraindication to organ transplantation. That has changed. Modern desensitization protocols of combining rituximab (a B-cell depleting antibody), plasma exchange or immunoadsorption, and intravenous immunoglobulin can lower the recipient's anti-donor isoagglutinin titers enough to allow safe transplantation [8].
Long-term outcome data from large kidney transplant centers now report patient survival around 99% at 1 year and graft survival above 90% over multi-year follow-up, approaching the results of ABO-compatible transplants [8]. ABO-incompatible programs have made transplantation accessible to patients who would otherwise wait years for a matched donor.
Toward Universal Blood: Enzymatic Conversion
A 2024 study published in Nature Microbiology by Jensen and colleagues at Lund University and the Technical University of Denmark identified enzymes from the gut bacterium Akkermansia muciniphila that can strip A, B, and several extended antigens from red cells [5]. Unlike earlier attempts that left residual antigens behind, the new enzyme cocktail produced units that closely resemble true type O.
However, significant hurdles remain before this technology can be widely adopted in clinical practice. First, producing and purifying these bacterial enzymes at an industrial scale for millions of donor units remains cost-prohibitive. Second, there are unresolved safety concerns regarding alloimmunization. If trace amounts of the bacterial enzyme remain in the converted blood unit despite rigorous washing, the recipient's immune system could develop antibodies against the enzyme itself, potentially triggering severe allergic or immune reactions during subsequent transfusions [12].
Safety and regulatory work continues. But if it succeeds, enzymatic conversion could ease chronic blood shortages, simplify logistics, and protect patients from accidental ABO-mismatched transfusions [5].
Frequently Asked Questions (FAQs)
Can your blood type change over time?
Not in everyday life. Two clinical exceptions exist. After an allogeneic bone marrow or stem cell transplant, the recipient's blood-forming cells are replaced by the donor's, and over months the recipient's circulating ABO type converts to the donor's type. Some leukemias and myelodysplastic syndromes can transiently weaken antigen expression, making typing ambiguous. The rare acquired B phenotype in patients with bowel disease can also temporarily make a group A person test as AB.
Why is type O the "Universal Donor" for red cells?
Type O red cells lack both A and B antigens. There is nothing on the surface for a recipient's anti-A or anti-B to attack. The fully universal product is O negative (also lacking the RhD antigen), reserved for emergencies and women of childbearing age.
What happens if I am given the wrong blood type?
You can develop an acute hemolytic transfusion reaction. The recipient's anti-A or anti-B antibodies bind donor red cells within minutes, activating complement and bursting the cells inside blood vessels. Symptoms like fever, chills, back pain, dark urine, and hypotension can appear after just a few millilitres. Without immediate intervention, AHTR can cause kidney failure, disseminated intravascular coagulation, and death [2].
Why don't we naturally have anti-RhD antibodies the way we have anti-A and anti-B?
ABO antigens resemble bacterial sugars in our environment, so the infant immune system encounters look-alikes early in life and makes anti-A or anti-B without a transfusion or pregnancy. The RhD antigen is unique to human red cells. To produce anti-D, a person has to be exposed via blood-to-blood contact like a transfusion or, more commonly, fetal red cells crossing into a mother's circulation during pregnancy or delivery.
Is the H-antigen the same as type O?
Not quite. The H antigen is the precursor sugar structure on which A and B are built. People with type O carry the H antigen — in fact, more H than any other group, since nothing has been added on top. Only people with the Bombay phenotype lack the H antigen entirely, and they are clinically distinct from regular type O.
Can a person be a secretor for some ABO antigens but not others?
No. Secretor status is an "all-or-nothing" property of the FUT2 gene. If you secrete, you secrete whatever ABO antigens your genotype dictates (A, B, or H). If you do not, you secrete none of them.
Can a Bombay person genetically be type A or B?
Yes. A Bombay individual's ABO genotype can be A, B, AB, or O. They simply lack the H antigen needed to display A or B on the cell surface. If they pass an A or B allele to a child who inherits a normal FUT1 gene from the other parent, that child will express A or B normally — sometimes producing what looks like a "miraculous" blood group inheritance in the family.
Does my ABO blood group affect my risk of disease?
Modestly. Non-O blood groups are linked to higher risk of venous thromboembolism, group A to slightly higher risk of pancreatic and gastric cancers, and group A was associated with more severe COVID-19 in several pandemic-era studies [3,4]. The effects are small at the individual level and do not currently change clinical management for most people.
Glossary of Related Medical Terms
- Agglutination: Visible clumping of red cells when antibodies bind matching antigens.
- Allele: One of several versions of the same gene, found at the same chromosomal location.
- Alloantibody: An antibody made against an antigen from another person of the same species.
- Antibody-mediated rejection (AMR): Rejection of a transplanted organ caused by recipient antibodies attacking donor antigens.
- Codominant: Both alleles fully expressed when present together (A and B in group AB).
- Genotype: Genetic makeup at a specific gene (e.g., AO, BB, hh).
- Glycosyltransferase: An enzyme that attaches a sugar molecule to a protein, lipid, or other sugar.
- Hemolysis: The bursting of red blood cells.
- Immunogenicity: How strongly an antigen provokes an antibody response.
- Isoagglutinin: A naturally occurring antibody (anti-A or anti-B) directed against ABO antigens absent from one's own cells.
- Locus: The chromosomal location of a gene.
- Low-titer group O whole blood (LTOWB): Group O whole blood with low anti-A and anti-B titers, used in trauma resuscitation.
- Oligosaccharide: A short chain of sugar units; ABO antigens are oligosaccharides.
- Phenotype: The observable expression of a genotype (e.g., blood group A).
- Secretor: A person whose body secretes ABO antigens into saliva and other fluids because of a working FUT2 gene.
- Sensitization: Initial immune exposure that triggers antibody production.
- Variable expressivity: The same genotype producing different strengths of the same trait in different people.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005. Chapter 5, The ABO blood group. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2267/
- Romanos-Sirakis EC, Desai D. ABO Blood Group System. [Updated 2025 Apr 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK580518/
- Groot, H. E., Villegas Sierra, L. E., Said, M. A., Lipsic, E., Karper, J. C., & van der Harst, P. (2020). Genetically Determined ABO Blood Group and its Associations With Health and Disease. Arteriosclerosis, thrombosis, and vascular biology, 40(3), 830–838. https://doi.org/10.1161/ATVBAHA.119.313658
- Abegaz S. B. (2021). Human ABO Blood Groups and Their Associations with Different Diseases. BioMed research international, 2021, 6629060. https://doi.org/10.1155/2021/6629060
- Jensen, M., Stenfelt, L., Ricci Hagman, J., Pichler, M. J., Weikum, J., Nielsen, T. S., Hult, A., Morth, J. P., Olsson, M. L., & Abou Hachem, M. (2024). Akkermansia muciniphila exoglycosidases target extended blood group antigens to generate ABO-universal blood. Nature microbiology, 9(5), 1176–1188. https://doi.org/10.1038/s41564-024-01663-4
- Storry, J. R., Clausen, F. B., Castilho, L., Chen, Q., Daniels, G., Denomme, G., Flegel, W. A., Gassner, C., de Haas, M., Hyland, C., Yanli, J., Keller, M., Lomas-Francis, C., Nogues, N., Olsson, M. L., Peyrard, T., van der Schoot, E., Tani, Y., Thornton, N., Wagner, F., … Yahalom, V. (2019). International Society of Blood Transfusion Working Party on Red Cell Immunogenetics and Blood Group Terminology: Report of the Dubai, Copenhagen and Toronto meetings. Vox sanguinis, 114(1), 95–102. https://doi.org/10.1111/vox.12717
- COOMBS, R. R., MOURANT, A. E., & RACE, R. R. (1946). In-vivo isosensitisation of red cells in babies with haemolytic disease. Lancet (London, England), 1(6391), 264–266. https://doi.org/10.1016/s0140-6736(46)91925-3
- Naciri Bennani, H., Bobo Barry, K. M., Noble, J., Malvezzi, P., Jouve, T., & Rostaing, L. (2024). Outcomes of ABO-incompatible kidney transplants with very high isoagglutinin titers: a single-center experience and literature review. Frontiers in immunology, 15, 1504495. https://doi.org/10.3389/fimmu.2024.1504495
- International Society of Blood Transfusion (ISBT). (2023). Red Cell Immunogenetics and Blood Group Terminology. Retrieved from https://www.isbtweb.org/isbt-working-parties/rcibgt.html
- Garratty, G., Glynn, S. A., McEntire, R., & Retrovirus Epidemiology Donor Study (2004). ABO and Rh(D) phenotype frequencies of different racial/ethnic groups in the United States. Transfusion, 44(5), 703–706. https://doi.org/10.1111/j.1537-2995.2004.03338.x
- Goel, R., Bloch, E. M., Pirenne, F., Al-Riyami, A. Z., Crowe, E., Dau, L., Land, K., Townsend, M., Jecko, T., Rahimi-Levene, N., Patidar, G., Josephson, C. D., Arora, S., Vermeulen, M., Vrielink, H., Montemayor, C., Oreh, A., Hindawi, S., van den Berg, K., Serrano, K., … ISBT COVID-19 Working Group (2021). ABO blood group and COVID-19: a review on behalf of the ISBT COVID-19 Working Group. Vox sanguinis, 116(8), 849–861. https://doi.org/10.1111/vox.13076
- Rahfeld, P., & Withers, S. G. (2020). Toward universal donor blood: Enzymatic conversion of A and B to O type. The Journal of biological chemistry, 295(2), 325–334. https://doi.org/10.1074/jbc.REV119.008164