Key Takeaways
Serologic cross-matching is the last laboratory check before a red-cell transfusion. It mixes the patient's plasma with red cells from a specific donor unit to confirm they will not react. An incompatible cross-match means the unit cannot be transfused. The lab moves to antibody identification and antigen-matched donor selection.
- Major cross-matching (recipient plasma + donor cells) is the standard test. Minor cross-matching (donor plasma + recipient cells) is now rarely performed.
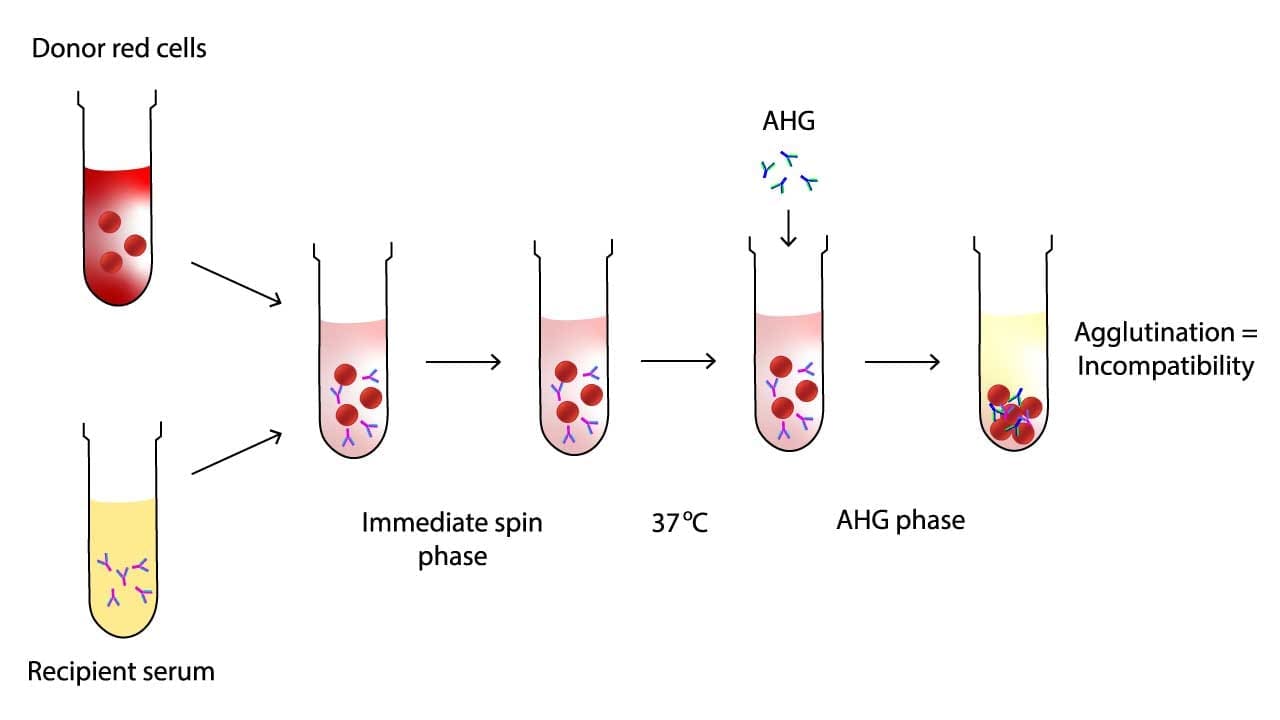
- The tube method runs in two main phases: an Immediate Spin phase to catch ABO mismatches, and an Anti-Human Globulin (AHG) phase, after 37°C incubation and washing, to catch clinically significant IgG antibodies [1,4].
- Coombs Control Cells must agglutinate at the end of any negative AHG test. If they do not, the result is invalid and the test must be repeated.
- Modern blood banks often use gel or solid-phase platforms, and an electronic cross-matching workflow for eligible patients with a negative antibody screen [1].
Introduction
A blood transfusion can save a life within minutes. It can also end one if the wrong unit is given. Cross-matching is the test that closes the gap between "the donor unit looks right on paper" and "this exact unit is safe for this exact patient."
Cross-matching does three things [1,4]:
- It catches ABO mismatches. A clerical or labeling error that survives earlier checks should not survive this one. ABO mismatch is the most common cause of fatal acute hemolytic transfusion reactions.
- It picks up clinically significant antibodies. Some patients carry antibodies against red-cell antigens outside the ABO system (for example, anti-K, anti-Fya, anti-Jka). These can cause delayed hemolysis if missed.
- It serves as a final safeguard. Blood typing and antibody screening narrow the field. Cross-matching tests the actual unit on the actual patient's plasma.
A note on language: you will see "cross-matching," "crossmatch," and "blood compatibility testing" used interchangeably. Strictly speaking, blood compatibility testing is the umbrella that includes ABO/Rh typing, antibody screening, and the cross-match itself. This article focuses on the cross-match step.
Major vs. Minor Cross-matching
Transfusion Medicine
| Feature | Major cross-match | Minor cross-match |
|---|---|---|
| What is mixed | Recipient plasma + donor red cells | Donor plasma + recipient red cells |
| Purpose | Detects ABO mismatch and recipient antibodies against donor cells | Detects donor antibodies against recipient cells |
| Frequency |
Standard Used for almost all red-cell transfusions |
Rare today Superseded by donor plasma screening |
| Clinical weight | Prevents acute and delayed hemolytic reactions | Used only in specific scenarios (e.g., minor incompatible plasma-containing components) |
Modern Cross-Matching Practices
Because most plasma in modern donor units is already screened and tested, minor cross-matching has largely fallen out of routine use. Major cross-matching remains the workhorse [1].
When Is a Serologic Cross-Match Actually Needed?
Not every patient who might need blood gets a full AHG cross-match. Modern labs choose between several pathways based on the antibody screen and clinical situation [1,4]:
- Type & Screen (T&S). ABO/Rh typing plus an antibody screen, performed in advance. Used when transfusion is possible but not likely (for example, low-risk surgery on the Maximum Surgical Blood Order Schedule).
- Electronic (computer) cross-match. When the patient has a negative current and historical antibody screen, two ABO determinations on file, and a validated laboratory information system, the computer confirms ABO compatibility with the chosen donor unit. No physical mixing is needed [1].
- Immediate-Spin serologic cross-match. An abbreviated tube cross-match (IS phase only) is acceptable for patients with a negative antibody screen and no history of clinically significant antibodies [1,6].
- Full AHG serologic cross-match. Required when the patient has a positive antibody screen, a history of clinically significant antibodies, or needs rare blood components.
In an emergency, even these are bypassed. Group O red cells (often O-negative for women of childbearing potential) can be released without a cross-match, with the cross-match completed retrospectively on a pre-transfusion sample [4].
A critical prerequisite for any of these cross-matching pathways is a valid patient sample. According to current AABB and BSH standards, if a patient has been transfused or pregnant within the preceding three months, or if their history is unknown or uncertain, the pre-transfusion sample must be collected no more than 3 days (72 hours) before the transfusion [7]. This strict time limit ensures that any newly developing, rapidly forming antibodies triggered by recent alloexposure are caught before a new unit is transfused. If the patient has no recent history of transfusion or pregnancy, some institutional protocols safely extend sample validity up to 7 or 28 days [1,7].
Pre-Transfusion Testing Algorithm
Determine the correct cross-matching procedure based on patient history.
Principle of Serologic Cross-matching
Two ideas drive the cross-match: antigen-antibody binding and agglutination.
Red blood cells carry antigens on their surface for example A, B, D (Rh), and many others. Plasma can carry antibodies against antigens the patient lacks. When an antibody finds its matching antigen on a donor cell, it binds. If enough antibodies bind, they bridge cells together into visible clumps. That is agglutination, and it is the readout of the test.
Some antibodies are strong and cause clumping at room temperature within seconds. These are usually IgM, including anti-A and anti-B. Other antibodies are weaker and need a 37°C incubation plus an AHG reagent (anti-human globulin, also called Coombs reagent) to become visible. These are usually IgG. The two phases of the tube method are designed to catch both types.
Materials
- Recipient serum or plasma
- Donor red cell suspension, 2–5% in saline
- Glass or plastic test tubes, labeled
- Calibrated pipettes and disposable tips
- Normal saline (0.9% NaCl)
- LISS (Low Ionic Strength Solution)
- Anti-Human Globulin (AHG) reagent
- IgG-sensitized Coombs Control Cells (CCC)
- Serologic centrifuge, calibrated
- 37°C incubator or heat block
Donor cells
Red cells from the donor unit are collected from an attached segment, washed, and resuspended at 2–5% in saline. They are not stored in EDTA at the working stage of the test.
Protocol (Tube Method, Major Cross-Match)
Disclaimer. Cross-matching protocols vary by region, accreditation body, reagent supplier, and institutional policy. This is a teaching outline. Always follow your laboratory's validated procedure. Authoritative sources include the AABB Technical Manual [1], the BSH/BCSH pre-transfusion compatibility guidelines [4], and ISBT resources.
Step 1 — Immediate Spin (IS) Phase
- Label a clean test tube with the patient identifier and donor unit number.
- Add 2 drops of recipient serum or plasma.
- Add 1 drop of 2–5% donor red cell suspension.
- Mix gently.
- Centrifuge per validated settings (typically about 900 × g for 15–20 seconds).
- Gently dislodge the cell button and look for agglutination or hemolysis against a good light source.
- Record the result.
Reading the result. Agglutination or hemolysis at this stage suggests ABO mismatch or a strong cold-reactive antibody. The unit is not safe to transfuse without further investigation. No agglutination means you can move on; it does not mean compatible yet.
Step 2 — 37°C Incubation with Enhancement Media
- Add 2 drops of an enhancement medium, such as LISS (Low Ionic Strength Solution) or PEG (Polyethylene Glycol), to the same tube.
- Mix gently.
- Incubate at 37°C for 10–15 minutes (follow specific manufacturer instructions).
Enhancement media speed up antibody binding by lowering the ionic strength around the cells (LISS) or removing water molecules to drive red cells closer together (PEG). Note that when PEG is used, the Immediate Spin phase and post-incubation 37°C readings are often skipped entirely to avoid false positives, proceeding directly to the wash and AHG phases. PEG is highly sensitive for detecting weak, clinically significant antibodies, such as those in the Kidd system (e.g., anti-Jkª) [1].
Step 3 — Wash
- Fill the tube with normal saline.
- Centrifuge and decant the supernatant completely.
- Repeat 3 to 4 times.
- After the final wash, leave only the cell button.
Thorough washing is critical. Any residual recipient globulins will neutralize the AHG reagent in the next step and hide a true incompatibility.
Step 4 — Anti-Human Globulin (AHG) Phase
- Add 2 drops of AHG reagent to the washed cell button.
- Mix gently and centrifuge per validated settings (typically about 1000 × g for 15–20 seconds).
- Gently resuspend the button and look for agglutination.
- Grade and record any reaction.
Step 5 — Coombs Control Cells (Check Cells)
Run only when the AHG result is negative.
- Add 1 drop of IgG-sensitized control cells to the tube.
- Mix and centrifuge per protocol.
- Look for agglutination.
Check cells must agglutinate. If they do not, the AHG reagent was inactive or washing was inadequate, the negative AHG result is invalid, and the test must be repeated.

Interpretation
Modern Platforms: Beyond the Tube and Serology
Most blood banks now use column agglutination technology (gel cards) or solid-phase red-cell adherence as the primary cross-match platform [1,5]. The principle is identical but the format is standardized, easier to read, and easier to store as a record.
A 2008 comparative study found gel and tube methods broadly concordant, with gel offering better sensitivity for some weak antibodies [5]. Gel cards are the default, with tube methods reserved for problem-solving or when reagent reactivity must be confirmed manually.
Furthermore, the cutting edge of compatibility testing now extends beyond serology into molecular red cell genotyping (DNA testing). For patients with sickle cell disease, thalassemia, or multiple complex alloantibodies, serologic cross-matching can become nearly impossible due to constant agglutination or a lack of compatible commercial antisera. Genotyping looks directly at the patient's DNA to determine their exact antigen profile. This allows reference laboratories to find perfectly matched units without relying solely on traditional liquid antigen-antibody reactions, completely bypassing serological interferences [9].
Troubleshooting
False Positives — agglutination without true incompatibility
Common causes
- Fibrin strands in incompletely clotted samples
- Bacterial contamination of reagents or saline
- Cold autoantibodies (e.g., anti-I, anti-i) reacting at room temperature
- Rouleaux formation in patients with abnormal plasma proteins (e.g., multiple myeloma)
- Over-centrifugation packing cells so tightly they look clumped
- Expired or contaminated AHG reagent
- A positive Direct Antiglobulin Test on the recipient's own cells
- Monoclonal antibody therapies, specifically anti-CD38 drugs like Daratumumab. Because donor red blood cells naturally express CD38, these drugs bind to the cells in the test tube, causing a false positive in the AHG phase for every single donor unit tested (panreactivity) [8].
What to do
- Inspect samples for fibrin or turbidity; re-centrifuge if needed.
- Run an autocontrol (recipient serum + recipient cells). A positive autocontrol points to autoantibody or a positive DAT, not necessarily donor incompatibility.
- For suspected rouleaux, perform saline replacement: a drop of saline disperses rouleaux but not true agglutination.
- For suspected cold antibodies, repeat with pre-warmed samples and reagents.
- Re-check reagent expiry and storage.
- Verify centrifuge calibration.
- For patients on anti-CD38 therapies, the laboratory must treat the donor red cells with DTT (dithiothreitol) to denature the CD38 antigen and eliminate the drug interference, or rely entirely on historical blood typing and molecular genotyping [8].
False Negatives — no agglutination despite true incompatibility
These are more dangerous because they wave through a unit that should not be released.
Common causes
- Forgetting to add a reagent (serum, donor cells, or AHG)
- Inadequate washing before AHG (residual globulins neutralize the reagent)
- Weak or expired AHG reagent
- Wrong cell-to-serum ratio (prozone or postzone effect)
- Under-centrifugation
- Antibodies present at very low titer
- Antibodies showing dosage (weaker reaction with heterozygous donor cells)
What to do
- Re-read the protocol step by step. Confirm every reagent was added.
- Wash 3–4 times with full decantation.
- Use enhancement media (LISS or PEG) where validated.
- Run AHG reagent QC daily with IgG-sensitized check cells.
- Verify centrifuge speed, time, and temperature.
- Review the patient's transfusion history and prior antibody work-up.
When to escalate transfusion concerns
If there is any clinical suspicion of incompatibility despite a negative cross-match, escalate. A retrospective hemolytic reaction is a much worse outcome than a delayed transfusion.
Emergency Crossmatch and Massive Transfusion Protocols (MTP)
In high-stakes clinical environments, such as a trauma bay or operating room, the time required for a full AHG crossmatch (45–60 minutes) can be a luxury the patient does not have.
When a patient is experiencing life-threatening hemorrhage, the "standard" crossmatch procedure is bypassed in favor of tiered emergency protocols. The goal is to provide compatible blood as quickly as possible while accepting a calculated level of immunological risk.
Uncrossmatched Emergency Release
This is the fastest possible option, used when the patient’s blood type is unknown and they are in immediate danger of exsanguination.
- O-Negative RBCs: Generally reserved for females of childbearing age to prevent RhD sensitization and potential future Hemolytic Disease of the Fetus and Newborn (HDFN).
- O-Positive RBCs: Often utilized for males or post-menopausal females to conserve the limited supply of O-negative units.
- The Protocol: The blood is released with an "Emergency Release" tag. The laboratory continues the crossmatch process after the blood has left the lab. If an incompatibility is found, the clinical team is notified immediately to stop the transfusion.
Abbreviated (Immediate Spin) Crossmatch
If the laboratory has a valid sample and has determined the patient's ABO/Rh type, an abbreviated cross-matching can be performed in roughly 5–10 minutes.
- The Process: Only the Immediate Spin (IS) phase is performed.
- The Goal: To confirm ABO compatibility and rule out catastrophic "wrong-type" errors.
- The Risk: It does not detect clinically significant IgG antibodies that only react at the 37°C or AHG phases.
Massive Transfusion Protocol (MTP)
An MTP is triggered when a patient requires massive amounts of blood products (typically defined as >10 units of RBCs within 24 hours or >4 units in 1 hour).
- Ratio-Driven Therapy: Instead of waiting for individual crossmatches, the lab provides "packs" of products in a pre-defined ratio, typically 1:1:1 (1 unit of Packed Red Blood Cells, 1 unit of Fresh Frozen Plasma, and 1 unit of Platelets).
- Switching Protocols: Once a patient has received a volume of uncrossmatched blood equivalent to their total blood volume, the laboratory may cease performing crossmatches entirely for subsequent units, as the patient’s original plasma (and any antibodies) has been largely replaced by donor products.
Legal and Clinical Requirements
For any emergency release, the following steps are mandatory:
- Signed Waiver: The requesting physician must sign a document acknowledging the risks of transfusing uncrossmatched blood.
- Sample Collection: A "pre-transfusion" sample must be drawn before the uncrossmatched units are given, if possible, to allow the lab to eventually complete the full compatibility testing.
Frequently Asked Questions (FAQs)
What is cross-matching, and why is it the last test before a blood transfusion?
Cross-matching is a compatibility test that mixes a small amount of the patient's plasma with red cells from a specific donor unit. It is the final check before transfusion because it tests the exact unit the patient will receive, catching any mismatch that earlier tests like ABO typing or antibody screening could miss.
What is the difference between major and minor cross-matching?
Major cross-matching tests the recipient's plasma against donor red cells. It is mandatory for almost every red-cell transfusion. Minor cross-matching tests the donor's plasma against recipient red cells. It is rarely performed today because most plasma-containing components are screened separately, but it can be relevant in specific scenarios.
What is an electronic crossmatch, and is it as safe as a serologic one?
An electronic crossmatch is a computer-based check that confirms ABO compatibility between the patient and a donor unit using verified records. It is considered safe for patients with a negative current and historical antibody screen, two independent ABO determinations on file, and a validated laboratory information system. It is faster than a serologic crossmatch and is widely used.
What does it mean if my crossmatch result is "incompatible"?
An incompatible crossmatch means the patient's plasma reacted with the donor's red cells in the laboratory. The unit cannot be transfused. The lab will then identify the antibody causing the reaction and find donor units that lack the matching antigen.
Why are Coombs control cells (check cells) added at the end of a negative AHG test?
They confirm that the AHG reagent worked. If the AHG reagent was inactive or the cells were not washed properly, a true incompatibility could be missed. Check cells are coated with IgG, so they must agglutinate when AHG is added. If they do not, the test is invalid and must be repeated.
How is blood given in a true emergency if there is no time to crossmatch?
In life-threatening bleeding, group O red cells (often O-negative for women of childbearing potential) can be released without a crossmatch. A crossmatch is then performed retrospectively on a sample drawn before transfusion. This balances immediate survival against the small residual risk of an unexpected antibody.
Glossary of Related Medical Terms
- Agglutination — visible clumping of red blood cells when antibodies bind to matching antigens on the cell surface.
- Hemolysis — destruction of red blood cells, releasing hemoglobin into surrounding fluid. In the lab, it can look like a pink or red tint to the supernatant.
- Antigen — a molecule on the surface of a red blood cell that the immune system can recognize. Examples include A, B, D (Rh), Kell, and Duffy.
- Antibody — a protein made by the immune system that binds to a specific antigen. Some antibodies cause transfusion reactions.
- ABO compatibility — the rule that a recipient must not receive red cells carrying an A or B antigen they have antibodies against.
- Anti-Human Globulin (AHG) reagent — a reagent that binds to human IgG antibodies or complement already attached to red cells, making the reaction visible. Also called Coombs reagent.
- Coombs Control Cells (Check Cells) — IgG-coated red cells added at the end of a negative AHG test to confirm the AHG reagent was active. They must agglutinate; if not, the test is invalid.
- Immediate Spin (IS) Phase — the first stage of a tube crossmatch, run at room temperature, mainly to catch ABO mismatches.
- LISS (Low Ionic Strength Solution) — an enhancement medium that speeds up antibody binding during 37°C incubation.
- Rouleaux — red cells stacked like coins, often seen with abnormal plasma proteins. Looks like agglutination but disperses with saline.
- Autocontrol — recipient serum tested against the recipient's own red cells, used to detect autoantibodies that could mimic incompatibility.
- Electronic crossmatch — a computer-based compatibility check used when the antibody screen is negative and validated criteria are met. No physical mixing of cells and serum is required.
- Type & Screen — ABO/Rh typing plus an antibody screen, performed in advance of possible transfusion.
- Type & Crossmatch — Type & Screen plus a serologic or electronic crossmatch against a specific donor unit, performed when transfusion is likely.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cohn, C. S., Delaney, M., Johnson, S. T., & Katz, L. M. (Eds.). (2023). AABB technical manual (21st ed.). AABB Press.
- Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2261/
- Bain, B. J., Bates, I., & Laffan, M. A. (2017). Dacie and Lewis practical haematology (12th ed.). Elsevier.
- British Committee for Standards in Haematology, Milkins, C., Berryman, J., Cantwell, C., Elliott, C., Haggas, R., Jones, J., Rowley, M., Williams, M., & Win, N. (2013). Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories. British Committee for Standards in Haematology. Transfusion medicine (Oxford, England), 23(1), 3–35. https://doi.org/10.1111/j.1365-3148.2012.01199.x
- Swarup, D., Dhot, P. S., Kotwal, J., & Verma, A. K. (2008). Comparative Study of Blood Cross Matching Using Conventional Tube and Gel Method. Medical journal, Armed Forces India, 64(2), 129–130. https://doi.org/10.1016/S0377-1237(08)80054-8
- Shulman, I. A., Nelson, J. M., Saxena, S., Thompson, J. C., Okamoto, M., Kent, D. R., & Nakayama, R. K. (1984). Experience with the routine use of an abbreviated crossmatch. American journal of clinical pathology, 82(2), 178–181. https://doi.org/10.1093/ajcp/82.2.178
- AABB. (2022). Standards for Blood Banks and Transfusion Services (33rd ed.). AABB.
- Chapuy, C. I., Nicholson, R. T., Aguad, M. D., Chapuy, B., Laubach, J. P., Richardson, P. G., Doshi, P., & Kaufman, R. M. (2015). Resolving the daratumumab interference with blood compatibility testing. Transfusion, 55(6 Pt 2), 1545–1554. https://doi.org/10.1111/trf.13069
- Westhoff C. M. (2019). Blood group genotyping. Blood, 133(17), 1814–1820. https://doi.org/10.1182/blood-2018-11-833954