Key Takeaways
Waldenström macroglobulinemia (WM) is a rare, slow-growing B-cell lymphoma characterized by the overproduction of IgM monoclonal immunoglobulin by lymphoplasmacytic lymphoma (LPL) cells.
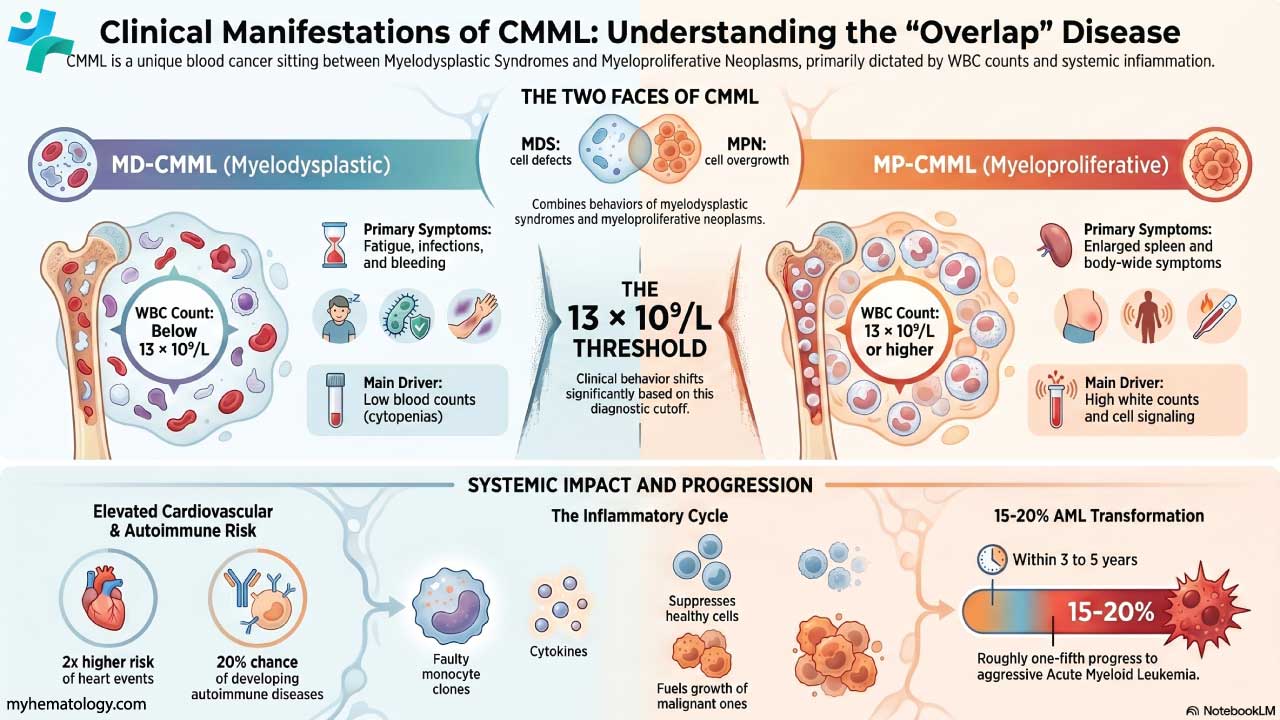
- Pathophysiology ▾: Primarily driven by the MYD88 L265P mutation, leading to uncontrolled LPL cell proliferation.
- Symptoms ▾: Includes fatigue, weakness, hyperviscosity syndrome (visual disturbances, headaches), peripheral neuropathy, and organomegaly.
- Diagnosis ▾: Relies on serum protein electrophoresis (SPEP), immunofixation electrophoresis (IFE), bone marrow biopsy, and genetic testing (MYD88 mutation).
- Treatment ▾: Varies based on symptoms and includes chemoimmunotherapy, BTK inhibitors, proteasome inhibitors, and plasmapheresis for hyperviscosity.
- Prognosis ▾: Variable, assessed by the IPSSWM; complications include hyperviscosity, neuropathy, and organ damage.
*Click ▾ for more information
Introduction
Waldenström macroglobulinemia (WM) is a rare, slow-growing type of non-Hodgkin lymphoma characterized by the uncontrolled proliferation of lymphoplasmacytic cells in the bone marrow, lymph nodes, and spleen. These malignant cells produce an excessive amount of immunoglobulin M (IgM) monoclonal protein, which can lead to various clinical manifestations, including hyperviscosity syndrome, anemia, and neurological symptoms. Essentially, it's a cancer of white blood cells where abnormal cells produce too much of a specific protein, causing a range of health issues.
Pathophysiology and Etiology
Waldenström macroglobulinemia (WM) originates from malignant B-lymphocytes that have undergone a specific differentiation pathway, resulting in lymphoplasmacytic lymphoma (LPL) cells. These cells exhibit a hybrid phenotype, possessing characteristics of both lymphocytes and plasma cells.
The process begins with a post-germinal center B-cell that acquires specific genetic mutations, most notably the MYD88 L265P mutation, which is present in the vast majority of Waldenström macroglobulinemia (WM) cases. This mutation leads to constitutive activation of the NF-κB signaling pathway, promoting cell survival and proliferation. This aberrant signaling drives the expansion of the lymphoplasmacytic lymphoma (LPL) clone within the bone marrow, lymph nodes, and spleen, displacing normal hematopoietic cells and leading to cytopenias like anemia, thrombocytopenia, and leukopenia. Additionally, other mutations, such as those in the CXCR4 gene, can contribute to the disease's pathogenesis, influencing cell trafficking and bone marrow infiltration.
The excessive IgM production is a hallmark of Waldenström macroglobulinemia (WM). This monoclonal IgM can lead to hyperviscosity syndrome, where the increased protein concentration in the blood causes sluggish blood flow, resulting in symptoms like visual disturbances, headaches, and neurological dysfunction. Additionally, IgM can have autoimmune properties, leading to complications like cryoglobulinemia (precipitation of IgM at cold temperatures), peripheral neuropathy, and cold agglutinin disease.
The bone marrow microenvironment itself plays a significant role in Waldenström macroglobulinemia (WM) pathogenesis. Stromal cells, cytokines, and growth factors within the bone marrow contribute to the survival and proliferation of LPL cells. The interplay between these factors and the malignant clone sustains the disease process. Essentially, Waldenström macroglobulinemia's (WM) pathophysiology is a complex interplay of genetic mutations, aberrant signaling pathways, and microenvironmental factors that collectively drive the proliferation of LPL cells and the overproduction of IgM, leading to the diverse clinical manifestations of the disease.
Risk Factors of Waldenström Macroglobulinemia (WM)
Waldenström macroglobulinemia (WM) risk factors involve a combination of demographic, genetic, and pre-existing conditions.
- Age: The risk of Waldenström macroglobulinemia (WM) increases significantly with age, with most diagnoses occurring in individuals over 60.
- Sex: Men are more likely to develop Waldenström macroglobulinemia (WM) than women.
- Race: WM is more prevalent among Caucasians.
- IgM Monoclonal Gammopathy of Undetermined Significance (MGUS): Having IgM MGUS, a precursor condition characterized by the presence of abnormal IgM protein without symptoms, increases the risk of developing Waldenström macroglobulinemia (WM);
- Family History: There's evidence suggesting a familial predisposition, with an increased risk for individuals with a family history of Waldenström macroglobulinemia (WM) or other B-cell lymphomas.
- Genetic Factors: While not strictly a "risk factor" in the sense of an environmental exposure, the presence of certain genetic mutations, particularly MYD88 L265P, is fundamentally linked to the disease.
Clinical Presentation and Symptoms
Waldenström macroglobulinemia (WM) presents with a wide array of clinical features and symptoms, largely stemming from the infiltration of lymphoplasmacytic lymphoma (LPL) cells and the overproduction of IgM.
General Constitutional Symptoms
- Fatigue: This is a very common and often debilitating symptom, resulting from anemia and the overall burden of the disease.
- Weakness
- Unexplained Weight Loss
- Night Sweats
- Fever
Hyperviscosity Syndrome
This arises from the increased IgM concentration in the blood, leading to thickened blood.
- Visual Disturbances: Blurred vision, diplopia (double vision), and retinal hemorrhages.
- Headaches: Often severe and persistent.
- Neurological Symptoms: Dizziness, vertigo, ataxia (loss of coordination), and altered mental status.
- Bleeding: Nasal bleeding, gum bleeding, and easy bruising.
Neurological Manifestations
- Peripheral Neuropathy: Numbness, tingling, and pain in the extremities, often due to IgM-mediated nerve damage.
- Bing-Neel Syndrome: A rare but serious complication involving central nervous system infiltration, leading to cognitive impairment, seizures, and other neurological deficits.
Organ Involvement
- Lymphadenopathy: Enlarged lymph nodes, often palpable in the neck, armpits, or groin.
- Hepatomegaly and Splenomegaly
- Anemia: Due to bone marrow infiltration and decreased red blood cell production.
- Cryoglobulinemia: Precipitation of IgM in cold temperatures, leading to Raynaud's phenomenon (numbness and color changes in fingers and toes), purpura (purple spots on the skin), and joint pain.
- Amyloidosis: Deposition of amyloid protein in organs, leading to organ dysfunction.
- Renal Involvement: Kidney dysfunction due to IgM deposition or amyloidosis.
- Pulmonary Involvement: Infiltration of the lungs, leading to shortness of breath and cough.
- Skin Manifestations: Purpura, or other rashes.
Other Symptoms
- Cold Agglutinin Disease: A type of autoimmune hemolytic anemia.
- Increased susceptibility to infections: Due to the impairment of normal immune function.
Laboratory Investigations
Laboratory investigations are crucial for diagnosing Waldenström macroglobulinemia (WM) and monitoring its progression.
- Complete Blood Count (CBC): Expected findings of anemia, leukopenia and thrombocytopenia due to bone marrow infiltration by LPL cells.
- Serum Protein Electrophoresis (SPEP) and Immunofixation Electrophoresis (IFE):
- SPEP: Shows a monoclonal spike (M-spike) in the gamma region, indicating the presence of a monoclonal protein.
- IFE: Confirms the M-spike as IgM, identifying the specific type of monoclonal immunoglobulin. This is a hallmark of WM.
- Bone Marrow Biopsy and Aspirate: Infiltration of the bone marrow by lymphoplasmacytic lymphoma (LPL) cells.
- Immunophenotyping and Flow Cytometry: Characterization of the LPL cells, confirming their B-cell lineage and identifying specific surface markers.
- Genetic Testing: MYD88 L265P mutation analysis: Positive in most cases, confirming the diagnosis. CXCR4 mutation may be positive in some cases which helps in prognostic evaluation.
- Serum Viscosity Measurement: Elevated and is particularly important in patients with hyperviscosity symptoms.
- Beta-2 Microglobulin (β2M): This protein is often elevated in Waldenström macroglobulinemia (WM) and can serve as a prognostic marker.
- Imaging Studies: CT scans, MRI, or PET scans may reveal lymphadenopathy, hepatosplenomegaly, or other organ involvement.
- Other Relevant Tests:
- Cryoglobulins: To detect cryoglobulinemia, which can cause symptoms in cold temperatures.
- Cold agglutinins
- Renal function tests
- Liver function tests
Differential Diagnosis of Waldenström Macroglobulinemia
It's crucial to differentiate Waldenström macroglobulinemia (WM) from other conditions that may present with similar clinical and laboratory features.
- IgM Monoclonal Gammopathy of Undetermined Significance (IgM MGUS): IgM MGUS is characterized by the presence of a monoclonal IgM protein without evidence of bone marrow infiltration or end-organ damage. Distinguishing Waldenström macroglobulinemia (WM) from IgM MGUS is crucial, as MGUS is generally a benign condition.
- Multiple Myeloma (MM): MM is characterized by the proliferation of plasma cells and the production of monoclonal IgG, IgA, or light chains. Although both Waldenström macroglobulinemia (WM) and MM involve monoclonal protein production, the type of immunoglobulin and the cellular morphology differ.
- Other B-cell Lymphomas: Other B-cell lymphomas, such as marginal zone lymphoma and mantle cell lymphoma, can present with lymphadenopathy and bone marrow infiltration. Immunophenotyping and genetic testing are essential for distinguishing these lymphomas from Waldenström macroglobulinemia (WM).
- Chronic Lymphocytic Leukemia (CLL): CLL is characterized by the proliferation of mature lymphocytes. Although both CLL and Waldenström macroglobulinemia (WM) can involve bone marrow infiltration and lymphadenopathy, the cellular morphology and immunophenotype differ. CLL typically expresses CD5, where Waldenström macroglobulinemia (WM) does not.
- Hyperviscosity Syndrome (due to other causes): Hyperviscosity can occur in conditions other than Waldenström macroglobulinemia (WM), such as polycythemia vera and other paraproteinemias. Identifying the underlying cause of hyperviscosity is essential for appropriate management.
- Cryoglobulinemia (due to other causes): Cryoglobulinemia can be associated with various underlying conditions, including infections (e.g., hepatitis C) and autoimmune diseases. Identifying the underlying cause is important for proper treatment.
- Amyloidosis (due to other causes): Amyloidosis can occur in multiple myeloma, and other conditions. Tissue biopsy is needed to confirm amyloidosis.
- Bing-Neel syndrome (due to other causes): Other diseases can affect the central nervous system.
Treatment and Management
The treatment and management of Waldenström macroglobulinemia (WM) depend on the patient's symptoms, disease burden, and overall health. Not all patients require immediate treatment, and a "watch and wait" approach may be appropriate for asymptomatic individuals.
Indications for Treatment
- Symptomatic disease (e.g., fatigue, weight loss, night sweats).
- Hyperviscosity syndrome.
- Symptomatic anemia or thrombocytopenia.
- Symptomatic lymphadenopathy or organomegaly.
- Peripheral neuropathy.
- Cryoglobulinemia with symptoms.
- Bing-Neel syndrome.
Treatment Modalities
- Chemoimmunotherapy: Rituximab-based regimens (e.g., rituximab with bendamustine, rituximab with cyclophosphamide, dexamethasone, and rituximab (R-CHOP)) are commonly used. These regimens combine the targeted antibody rituximab with chemotherapy drugs to kill LPL cells.
- BTK Inhibitors: Ibrutinib, zanubrutinib, and other Bruton tyrosine kinase (BTK) inhibitors are highly effective in WM. These drugs target the B-cell receptor signaling pathway, inhibiting the growth and survival of LPL cells. BTK inhibitors are often used as first line treatment.
- Proteasome Inhibitors: Bortezomib is a proteasome inhibitor that can be used in WM, particularly in patients with neuropathy. Often used in combination with rituximab.
- Plasma Exchange (Plasmapheresis): This procedure is used to rapidly reduce IgM levels in patients with hyperviscosity syndrome. It involves removing plasma from the blood and replacing it with albumin or other fluids. This is a temporary measure, and other treatments are needed to address the underlying disease.
- Monoclonal Antibodies: Rituximab, and other monoclonal antibodies are used to target CD20, on the surface of B cells.
- Other therapies: Other chemotherapy drugs, such as cladribine, may be used in certain cases.
Supportive Care
- Management of Anemia: Erythropoiesis-stimulating agents (ESAs) or blood transfusions may be used to treat anemia.
- Management of Infections: Prophylactic antibiotics or antiviral medications may be necessary in patients with increased susceptibility to infections.
- Management of Neuropathy: Medications such as gabapentin or pregabalin may be used to manage neuropathic pain.
- Pain Management: Pain medications may be needed to manage pain associated with organomegaly or other complications.
Monitoring and Follow-Up
- Regular monitoring of IgM levels, CBC, and clinical symptoms is essential.
- Monitoring for treatment response and relapse is crucial.
- Patients should be monitored for potential treatment-related toxicities.
Treatment Considerations
Treatment decisions should be individualized based on the patient's age, comorbidities, and preferences. Clinical trials may offer access to novel therapies for Waldenström macroglobulinemia (WM).
Prognosis and Complications
Waldenström macroglobulinemia (WM) is generally considered an indolent (slow-growing) lymphoma, and many patients can live for years with the disease. However, the course of Waldenström macroglobulinemia (WM) can vary significantly among individuals. Factors influencing prognosis include:
- Age
- Disease stage
- Presence of specific genetic mutations (e.g., CXCR4 mutations)
- Response to treatment
International Prognostic Scoring System for Waldenström Macroglobulinemia (IPSSWM)
The IPSSWM is a tool used to predict the prognosis of patients with Waldenström macroglobulinemia (WM). This scoring system helps clinicians to stratify patients and guide treatment decisions.
| Risk Factor | Cutoff Value | Points |
| Age | > 65 years | 1 |
| Hemoglobin | ≤ 10.5 g/dL | 1 |
| Platelet Count | ≤ 100 x 109/L | 1 |
| β2-microglobulin | > 3 mg/L | 1 |
| Serum Monoclonal IgM Protein | > 70 g/L | 1 |
Scoring
- Low 0 - 1 points
- Intermediate 2 points
- High ≥ 3 points
Interpretation
- Low-risk: Patients in this group generally have a better prognosis.
- Intermediate-risk: Patients in this group have an intermediate prognosis.
- High-risk: Patients in this group have a less favorable prognosis.
Complications of Waldenström macroglobulinemia (WM)
- Hyperviscosity Syndrome: Can lead to visual disturbances, neurological symptoms, and bleeding.
- Peripheral Neuropathy: Can cause numbness, tingling, and pain in the extremities.
- Bing-Neel Syndrome: Rare but a serious complication involving central nervous system infiltration.
- Cryoglobulinemia: Can cause Raynaud's phenomenon, purpura, and joint pain.
- Amyloidosis: Can lead to organ dysfunction.
- Anemia: Can cause fatigue and weakness.
- Infections: Increased susceptibility to infections due to impaired immune function.
- Transformation to Aggressive Lymphoma: In rare cases, Waldenström macroglobulinemia (WM) can transform into a more aggressive type of lymphoma.
- Treatment-Related Toxicities: Chemotherapy and other treatments can cause side effects.
- Long term side effects of the disease: Organ damage due to long term IgM deposition.
- Bleeding: Due to hyperviscosity, or thrombocytopenia.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Gertz MA. Waldenström macroglobulinemia: 2023 update on diagnosis, risk stratification, and management. Am J Hematol. 2023 Feb;98(2):348-358. doi: 10.1002/ajh.26796. Epub 2023 Jan 1. PMID: 36588395; PMCID: PMC10249724.
- Dimopoulos MA, Kastritis E. How I treat Waldenström macroglobulinemia. Blood. 2019 Dec 5;134(23):2022-2035. doi: 10.1182/blood.2019000725. PMID: 31527073.
- Grunenberg A, Buske C. How to manage waldenström's macroglobulinemia in 2024. Cancer Treat Rev. 2024 Apr;125:102715. doi: 10.1016/j.ctrv.2024.102715. Epub 2024 Mar 5. PMID: 38471356.
- Treon SP, Xu L, Guerrera ML, Jimenez C, Hunter ZR, Liu X, Demos M, Gustine J, Chan G, Munshi M, Tsakmaklis N, Chen JG, Kofides A, Sklavenitis-Pistofidis R, Bustoros M, Keezer A, Meid K, Patterson CJ, Sacco A, Roccaro A, Branagan AR, Yang G, Ghobrial IM, Castillo JJ. Genomic Landscape of Waldenström Macroglobulinemia and Its Impact on Treatment Strategies. J Clin Oncol. 2020 Apr 10;38(11):1198-1208. doi: 10.1200/JCO.19.02314. Epub 2020 Feb 21. PMID: 32083995; PMCID: PMC7351339.
- Castillo JJ, Treon SP. How we manage Bing-Neel syndrome. Br J Haematol. 2019 Nov;187(3):277-285. doi: 10.1111/bjh.16167. Epub 2019 Aug 20. PMID: 31430829.