Key Takeaways
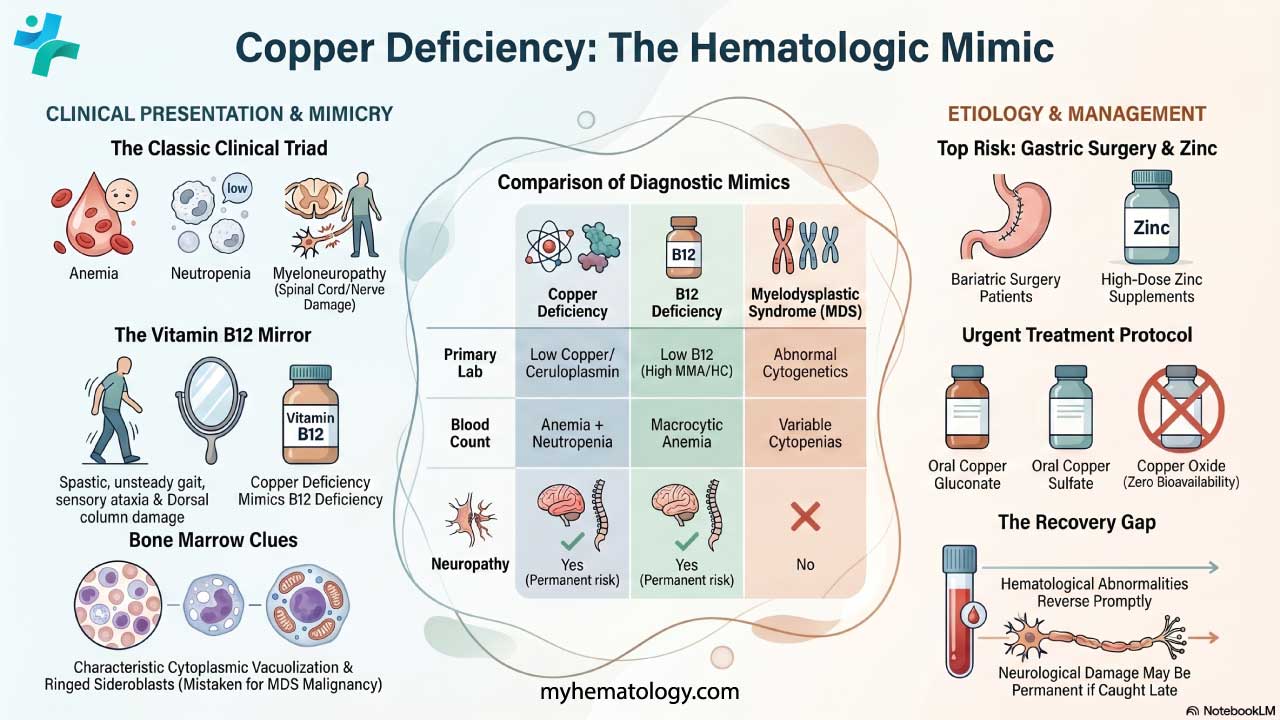
Copper deficiency is an under-recognized cause of cytopenias and neurological disease, with the classic triad of anemia, neutropenia, and myeloneuropathy [1,3].
- Causes ▾: The commonest causes are bariatric and upper gastrointestinal surgery, excess zinc ingestion, malabsorption syndromes, and prolonged parenteral nutrition lacking copper [2,4].
- Clinical manifestations ▾: The neurological picture is a myelopathy with spastic gait and sensory ataxia that closely mimics subacute combined degeneration of the spinal cord caused by B12 deficiency [4,7].
- Laboratory Investigations & Diagnosis ▾: Diagnosis rests on low serum copper and low ceruloplasmin, with serum zinc measured to exclude zinc-induced copper deficiency. Bone marrow may mimic myelodysplastic syndrome with ringed sideroblasts and vacuolated precursors [1,5,6].
- Treatment & management ▾: Hematological abnormalities reverse promptly with copper replacement, but neurological damage may be permanent — making early recognition critical [3,6].
*Click ▾ for more information
Introduction
Copper is a trace element the human body needs in tiny amounts but cannot do without. It sits at the heart of enzymes that handle iron transport, energy production, antioxidant defense, connective tissue cross-linking, and the myelin coating around nerves [2]. Lose it, and several systems falter at once.
This is why copper deficiency matters in hematology even though most students hear far more about iron and B12. The presentation overlaps strikingly with both B12 deficiency and myelodysplastic syndrome, which means it is frequently missed or misdiagnosed [1,5]. Patients have been referred for bone marrow transplantation when a simple oral supplement would have fixed the problem [1].
The condition is treatable. The challenge is thinking of it. The good news is that once the clinical pattern clicks — cytopenias plus a spinal cord syndrome in someone with prior gastric surgery or zinc exposure — copper deficiency becomes one of the more satisfying diagnoses in clinical hematology.
Causes of Copper Deficiency

Copper deficiency in adults is almost always acquired. Inherited disease (Menkes disease) is rare and presents in infancy. For adult patients, four mechanisms dominate.
Post-surgical malabsorption
Bariatric surgery, particularly Roux-en-Y gastric bypass, is now the most frequent cause of severe acquired copper deficiency [2,4]. Copper is absorbed mainly in the duodenum and proximal jejunum. Surgery that bypasses these segments dramatically reduces uptake. Standard post-bariatric multivitamins contain only 1–3 mg of copper daily, which is enough for prevention in many patients but insufficient to treat established deficiency [2]. Gastrectomy and other upper gastrointestinal surgeries carry similar risk.
In one retrospective series, 25% of patients with copper deficiency and hematological abnormalities had undergone bariatric surgery, and a further 35% had other gastrointestinal procedures [6].
Excess zinc
Zinc and copper compete for absorption in the small intestine. High zinc intake upregulates an intestinal protein called metallothionein, which binds copper tightly and prevents it from entering circulation [4]. Sources of excessive zinc include:
- Over-the-counter zinc supplements, particularly high-dose immune regimens which saw a significant increase in use following the COVID-19 pandemic [1].
- Zinc-containing denture adhesives. While major manufacturers voluntarily removed zinc from their formulas around 2010 due to myeloneuropathy risks, older, imported, or generic brands may still contain it [12].
- Some cold remedies and lozenges.
- Industrial exposure.
Zinc-induced copper deficiency is increasingly reported and is often missed because patients do not think of supplements as medications [4,7].
Malabsorption syndromes
Celiac disease, inflammatory bowel disease, and short bowel syndrome can all reduce copper absorption. So can chronic diarrhea of any cause [2].
Prolonged parenteral nutrition
Total parenteral nutrition (TPN) formulations without adequate trace element supplementation can cause deficiency over weeks to months. Jejunostomy feeding can also bypass the main absorption site [2].
Other risk factors
- Idiopathic. In around 20–30% of adult cases, no clear cause is identified despite thorough investigation [1,6].
- Certain chelation therapies. Copper-chelating drugs used historically (such as clioquinol) caused syndromes that resemble copper deficiency [4].
Food Sources of Copper
Copper is widely distributed in food, which is why dietary deficiency without an absorption problem is unusual in adults. Good sources include:
- Shellfish, especially oysters, which are among the richest dietary sources
- Organ meats, particularly liver
- Nuts and seeds, including cashews, sunflower seeds, and sesame seeds
- Whole grains and wheat bran
- Dark chocolate and cocoa
- Legumes such as lentils, beans, and chickpeas
- Mushrooms
The recommended daily intake for adults is around 0.9 mg, with higher requirements in pregnancy and lactation.
How Copper Deficiency Causes Anemia and Neutropenia
Copper acts as a cofactor for several enzymes critical to blood and nerve function. Understanding two of them explains most of the clinical picture.
Copper, ceruloplasmin, and iron metabolism
Ceruloplasmin is the main copper-carrying protein in blood. It also functions as a ferroxidase, converting iron from its ferrous (Fe²⁺) to ferric (Fe³⁺) form so it can bind transferrin and be transported to the bone marrow [2]. Hephaestin, another copper-dependent enzyme in the intestinal lining, performs a similar role at the point of iron absorption [2].
When copper is deficient, both enzymes underperform. Iron gets trapped inside cells and cannot be loaded onto transferrin efficiently. The result is functional iron deficiency even when total body iron is normal or high. This explains why copper-deficient patients often have anemia that does not respond to iron supplementation [4,7].
Effects on hematopoiesis
Copper-dependent enzymes also support DNA synthesis, mitochondrial energy production (via cytochrome c oxidase), and protein synthesis in dividing cells [2]. Without enough copper, bone marrow precursors mature abnormally. The bone marrow shows characteristic features:
- Cytoplasmic vacuolization of erythroid and myeloid precursors
- Ringed sideroblasts (red cell precursors with iron-laden mitochondria forming a ring around the nucleus)
- Dysplastic changes in myeloid cells
These changes overlap heavily with myelodysplastic syndrome (MDS), which is why patients with copper deficiency have sometimes been mistakenly worked up for hematological malignancy [1,5].
Diagnostic Clue of Copper Deficiency
Anemia in copper deficiency can be microcytic, normocytic, or macrocytic depending on the dominant mechanism [3]. Neutropenia is almost always present. Thrombocytopenia, by contrast, is unusual. This pattern of "two out of three cell lines affected" is itself a diagnostic clue.
Clinical Features
Copper deficiency typically presents with a combination of blood and nerve abnormalities. Skin and connective tissue changes occur less commonly.
Hematological features
Most patients present with symptoms of anemia (fatigue, breathlessness, pallor) and findings of neutropenia (recurrent infections, mouth ulcers) [1,3]. The blood count may have been abnormal for months before diagnosis. A bone marrow biopsy is often performed because the picture mimics MDS [5,6].
Neurological features: copper deficiency myeloneuropathy
This is the most serious complication and the one most likely to leave permanent damage. Patients describe a slowly progressive syndrome of [4,7]:
- Sensory ataxia. Difficulty walking, especially in the dark or with eyes closed, due to loss of position sense from dorsal column damage.
- Spastic gait. Stiffness and weakness from corticospinal tract involvement, often with brisk reflexes and upgoing plantars.
- Paresthesia. Numbness or tingling, usually starting in the feet.
- Positive Romberg sign. Loss of balance with eyes closed.
The clinical and MRI findings are nearly identical to subacute combined degeneration of the spinal cord seen in B12 deficiency [4,7]. Spinal MRI typically shows a high T2 signal in the dorsal cervical and thoracic cord. Take note that copper deficiency myeloneuropathy can occur without any hematological abnormalities, which is one reason it is so often missed [4].
Skin and connective tissue features
Less common but worth recognizing:
- Skin depigmentation and pale patches
- Hair changes, including loss of pigment
- Brittle bones and connective tissue weakness from impaired lysyl oxidase activity (which normally cross-links collagen and elastin)
Optic neuropathy
Rarely, copper deficiency can cause visual disturbance from optic nerve involvement, paralleling another B12 deficiency feature [4].

Diagnosis of Copper Deficiency
Suspecting copper deficiency starts with the clinical pattern: unexplained cytopenias, a myelopathy mimicking B12 deficiency, and a history that includes gastric surgery, zinc exposure, or long-term parenteral nutrition.
History and examination
Key questions:
- Have you had any stomach or weight-loss surgery?
- Are you taking zinc supplements, denture adhesives, or cold remedies containing zinc?
- Are you on home parenteral or jejunal feeding?
- Do you have any gastrointestinal disease such as celiac or Crohn's?
On examination, look for pale skin and conjunctivae, signs of infection, neurological signs (vibration, proprioception, Romberg, gait, tone, reflexes, plantars), and any skin or hair depigmentation.
Laboratory diagnosis
First-line tests
- Serum copper. Low in deficiency. Normal range varies by lab but is typically 11.2–20.6 µmol/L (or 80–155 µg/dL). Severe deficiency is generally defined as serum copper below 7.9 µmol/L (or roughly < 0.5 µg/mL) [8].
- Serum ceruloplasmin. Usually low (< 0.2 g/L or < 20 mg/dL) [8,9].
- Serum zinc. Essential when zinc-induced copper deficiency is suspected. Elevated zinc supports the diagnosis [8,9].
- Complete blood count and blood film. Anemia, neutropenia, and dysplastic features.
An important caveat
Both serum copper and ceruloplasmin are acute-phase reactants. Systemic inflammation, severe infections, or malignancies can falsely elevate both markers into the normal range, masking an underlying intracellular deficiency. Always interpret ceruloplasmin and serum copper alongside a C-reactive protein (CRP) level and the clinical context [8,13].
Second-line tests
- 24-hour urinary copper. Typically low in copper deficiency (in contrast to Wilson's disease, where urinary copper is high) [4].
- Bone marrow examination. Often performed because of the MDS-like picture. Findings include vacuolated erythroid and myeloid precursors, ringed sideroblasts, iron-containing plasma cells, and reduced granulocyte precursors [5,6].
- MRI of the spinal cord. Indicated if neurological signs are present. Typically shows high T2 signal in the dorsal columns [4].
Differential diagnosis
Always consider and exclude:
- B12 deficiency. The clinical picture is nearly identical. Both can coexist, and checking one without the other is a classic diagnostic pitfall. If a B12 level is borderline, checking methylmalonic acid (MMA) and homocysteine is critical; strictly normal MMA and homocysteine levels effectively rule out functional B12 deficiency, pointing toward copper as the primary culprit [4].
- Folate deficiency
- Myelodysplastic syndrome. The bone marrow can look very similar [1,5].
- HIV and other infections
- Drug-induced cytopenias
A useful rule of thumb
In a patient with cytopenias plus neurological signs, check copper, B12, and folate together.
Treatment of Copper Deficiency
The goals of treatment are to restore copper status, reverse hematological abnormalities, halt neurological progression, and treat the underlying cause.
Removing the cause
This is often the most important step:
- Stop zinc supplements or zinc-containing denture adhesives immediately.
- Adjust parenteral nutrition to include adequate copper.
- Address underlying malabsorption where possible.
Oral copper replacement
For most patients, oral copper is effective and well tolerated. Several regimens are used, all in similar dose ranges [2,9,10]:
- Mayo Clinic regimen: 6 mg elemental copper daily for 1 week, then 4 mg daily for 1 week, then 2 mg daily as maintenance [10].
- Simpler alternative: 2–4 mg elemental copper daily until levels normalize, then maintenance based on response.
Oral copper is given as copper gluconate, copper sulfate, or copper chloride. The specific formulation is critical: clinicians must specifically prescribe copper gluconate, copper sulfate, or copper chloride. Copper oxide is exceptionally poorly absorbed (featuring near-zero bioavailability) and should be strictly avoided when treating deficiency [14].
Intravenous copper
Reserved for severe deficiency, when oral replacement fails, or when malabsorption is profound. Typical regimens use 2–4 mg of elemental copper daily intravenously for around 5–6 days, followed by oral maintenance [8,11]. Modern bariatric guidelines recommend upfront intravenous copper for post-gastric bypass (e.g., Roux-en-Y) patients presenting with severe neurological deficits. The anatomical bypass makes oral absorption so unreliable that waiting to gauge the efficacy of oral therapy risks permanent, irreversible spinal cord damage [15].
Monitoring response
- Hematological recovery is rapid. Anemia and neutropenia typically resolve over 4 to 12 weeks of treatment [8,11].
- Neurological recovery is variable. Improvement, when it occurs, tends to favor sensory symptoms over motor signs. Some patients stabilize without further decline but do not fully recover [4,7].
- Recheck copper and ceruloplasmin at around 3 months. If oral therapy is not working, transition to intravenous administration [9].
- Long-term follow-up is essential, particularly in post-bariatric patients, who should be screened every 6 to 12 months indefinitely [2].
Dietary support
In addition to supplements, encourage copper-rich foods (shellfish, nuts, legumes, whole grains, organ meats) and avoid unnecessary zinc supplementation.
Why Early Diagnosis Matters
Copper deficiency illustrates a recurring lesson in hematology: a treatable nutritional disorder can cause permanent neurological harm if missed. The blood findings reverse predictably with replacement. The spinal cord does not always recover [3,6].
The practical takeaways are to think about copper in any patient with unexplained cytopenias, MDS-like marrow findings without classic cytogenetic abnormalities, or a B12-deficiency-like myelopathy with a normal B12 level. Always ask about bariatric surgery and zinc exposure.
Persistent fatigue, repeated infections, numbness, or balance problems in someone with prior weight-loss surgery, long-term zinc supplementation, or feeding tube nutrition deserves a copper level. Catching copper deficiency early usually means full hematological recovery and a much better chance of preventing lasting nerve damage.
Frequently Asked Questions (FAQs)
What is copper deficiency and why does it matter?
Copper deficiency means the body does not have enough copper to support the enzymes that make blood cells, transport iron, produce energy, and protect nerves. It typically causes a combination of anemia, low white cell counts (neutropenia), and a slowly progressive spinal cord problem called myeloneuropathy. The blood abnormalities reverse quickly with treatment, but nerve damage can become permanent if diagnosis is delayed, which is why early recognition matters.
Who is most at risk of copper deficiency?
The highest-risk groups are people who have had bariatric surgery (especially Roux-en-Y gastric bypass), other upper gastrointestinal surgery, or gastrectomy. Other key risk groups include people taking high-dose zinc supplements, those using zinc-containing denture adhesives heavily, patients on long-term total parenteral nutrition without adequate copper, and people with malabsorption from celiac disease, Crohn's disease, or short bowel syndrome. Dietary deficiency alone is rare in healthy adults.
Can zinc supplements really cause copper deficiency?
Yes. Zinc and copper compete for absorption in the small intestine. High zinc intake increases an intestinal protein called metallothionein, which traps copper inside the gut lining and prevents it from reaching the bloodstream. Cases have been linked to long-term zinc supplement use, cold remedies containing zinc, and even excessive use of zinc-containing denture creams. Anyone with unexplained anemia, neutropenia, or nerve symptoms who takes zinc-containing products should have copper checked.
How is copper deficiency diagnosed?
The first step is measuring serum copper and serum ceruloplasmin, both of which are low in deficiency. Serum zinc is also checked to rule out zinc-induced copper deficiency. A complete blood count usually shows anemia and neutropenia, and the blood film and bone marrow may show changes that look very similar to myelodysplastic syndrome. If neurological symptoms are present, MRI of the spinal cord often shows changes in the dorsal columns. One important pitfall is that ceruloplasmin is an acute-phase reactant — inflammation, pregnancy, or oral contraceptive use can falsely raise it and mask the diagnosis.
Why does copper deficiency look like B12 deficiency?
Both conditions damage the same parts of the spinal cord — the dorsal columns and lateral corticospinal tracts — producing nearly identical clinical pictures of spastic gait, sensory ataxia, and a positive Romberg sign. Both can also cause macrocytic anemia. The two can even coexist, so most clinicians check copper, B12, and folate together when a patient presents with cytopenias and neurological signs. A B12-deficiency-like syndrome with a normal B12 level should prompt a copper test.
How is copper deficiency treated?
Treatment has two parts: replacing copper and removing the cause. Most patients are treated with oral elemental copper, typically 6 mg daily for one week, then 4 mg daily for one week, then 2 mg daily as maintenance. Intravenous copper at 2–4 mg daily for around five to six days is used for severe deficiency or when oral therapy fails. Equally important is stopping any zinc supplements, adjusting parenteral nutrition, or addressing the underlying malabsorption. Hematological recovery usually takes 4 to 12 weeks. Neurological recovery is slower and may be incomplete.
Is the nerve damage from copper deficiency reversible?
Partly. Anemia and neutropenia almost always resolve completely with treatment. Neurological symptoms are different. Some patients improve, particularly sensory symptoms, but many stabilize without full recovery, and a few continue to progress despite replacement. The earlier copper is replaced, the better the neurological outcome. This is the main reason copper deficiency should never be treated as a minor or low-priority diagnosis once identified.
Do I need lifelong follow-up after copper deficiency is treated?
It depends on the cause. Patients who had a one-off cause (such as a course of high-dose zinc that has now been stopped) may not need indefinite monitoring once levels normalize. Patients with permanent risk factors — bariatric surgery, ongoing malabsorption, long-term parenteral nutrition — need regular copper and ceruloplasmin checks, typically every 6 to 12 months, for life. Standard post-bariatric multivitamins contain only 1–3 mg of copper daily, which may not be enough to prevent recurrence in everyone.
Glossary of Related Medical Terms
- Copper — An essential trace element that the body needs in small amounts. It acts as a cofactor for enzymes involved in iron transport, energy production, antioxidant defense, connective tissue formation, and nerve function.
- Ceruloplasmin — The main copper-carrying protein in blood. It also functions as a ferroxidase enzyme, converting iron to a form that can be transported to tissues. Low ceruloplasmin is a key marker of copper deficiency.
- Ferroxidase — An enzyme that oxidizes iron from its ferrous (Fe²⁺) to ferric (Fe³⁺) form so it can bind transferrin and be transported in the blood.
- Hephaestin — A copper-dependent enzyme in the intestinal lining that helps move absorbed iron from gut cells into the bloodstream. It links copper status to iron metabolism.
- Metallothionein — A small protein in intestinal cells that binds metals, including copper and zinc. High zinc intake increases metallothionein and traps copper, preventing its absorption.
- Cytochrome c oxidase — A copper-containing enzyme in the mitochondrial electron transport chain, essential for cellular energy production.
- Lysyl oxidase — A copper-dependent enzyme that cross-links collagen and elastin, giving strength to bones, blood vessels, and other connective tissues.
- Superoxide dismutase (Cu/Zn-SOD) — A copper- and zinc-containing enzyme that protects cells from oxidative damage by neutralizing reactive oxygen species.
- Neutropenia — A low neutrophil count, increasing the risk of bacterial and fungal infections. A near-universal finding in copper deficiency.
- Cytopenia — A reduction in the number of one or more types of blood cells. Copper deficiency typically causes anemia and neutropenia together.
- Macrocytic anemia — Anemia in which red blood cells are larger than normal. Can occur in copper deficiency as well as in B12 and folate deficiency.
- Ringed sideroblasts — Red blood cell precursors with iron-laden mitochondria forming a ring around the nucleus. Seen in copper deficiency and also in myelodysplastic syndrome.
- Cytoplasmic vacuolization — Small clear spaces (vacuoles) in the cytoplasm of bone marrow precursor cells. A characteristic finding in copper deficiency.
- Myelodysplastic syndrome (MDS) — A group of bone marrow disorders where blood cells develop abnormally. Copper deficiency can mimic MDS closely on bone marrow examination.
- Myeloneuropathy — A combined condition involving damage to the spinal cord (myelopathy) and to peripheral nerves (neuropathy). The classic neurological presentation of copper deficiency.
- Myelopathy — Disease or damage of the spinal cord, causing weakness, sensory loss, and difficulty with coordination.
- Subacute combined degeneration (SACDC) — Degeneration of the dorsal columns and lateral corticospinal tracts of the spinal cord. Classically caused by B12 deficiency but produced by copper deficiency in an almost identical pattern.
- Dorsal columns — Tracts at the back of the spinal cord that carry vibration sense, proprioception, and fine touch. Damage causes sensory ataxia and a positive Romberg sign.
- Lateral corticospinal tracts — Motor pathways in the spinal cord. Damage causes spasticity, brisk reflexes, and upgoing plantars (Babinski sign).
- Sensory ataxia — Loss of coordination caused by impaired sensation of joint position, rather than damage to the cerebellum. Patients often walk unsteadily, especially in the dark.
- Romberg sign — A clinical test in which the patient stands with feet together and eyes closed. Loss of balance suggests dorsal column or proprioceptive damage.
- Spastic gait — A stiff, scissoring walking pattern caused by damage to motor pathways in the spinal cord or brain.
- Paresthesia — Abnormal sensations such as tingling, numbness, or "pins and needles," typically caused by nerve damage.
- Bariatric surgery — Weight-loss surgery that alters the stomach or small intestine. Roux-en-Y gastric bypass is the procedure most strongly associated with acquired copper deficiency.
- Roux-en-Y gastric bypass — A bariatric procedure that bypasses most of the stomach and the duodenum, the main site of copper absorption.
- Total parenteral nutrition (TPN) — Intravenous feeding that bypasses the gastrointestinal tract entirely. Can cause copper deficiency if trace elements are not adequately supplemented.
- Menkes disease — A rare X-linked inherited disorder of copper transport, presenting in male infants with neurological deterioration, abnormal hair, and connective tissue problems. Distinct from acquired copper deficiency.
- Wilson's disease — An inherited disorder of copper excess, in which copper accumulates in the liver, brain, and eyes. The opposite end of the copper-disease spectrum from copper deficiency.
- Acute-phase reactant — A protein whose blood level rises in response to inflammation. Ceruloplasmin is an acute-phase reactant, which is why it can be misleadingly normal in copper-deficient patients with concurrent inflammation.
- 24-hour urinary copper — A test measuring copper excretion over a full day. Low in copper deficiency and high in Wilson's disease, helping distinguish the two.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Wazir, S. M., & Ghobrial, I. (2017). Copper deficiency, a new triad: anemia, leucopenia, and myeloneuropathy. Journal of community hospital internal medicine perspectives, 7(4), 265–268. https://doi.org/10.1080/20009666.2017.1351289
- Parish, C.R., & O'Donnell, K. (2020). Copper deficiency: Like a bad penny. Practical Gastroenterology.
- Halfdanarson, T. R., Kumar, N., Li, C. Y., Phyliky, R. L., & Hogan, W. J. (2008). Hematological manifestations of copper deficiency: a retrospective review. European journal of haematology, 80(6), 523–531. https://doi.org/10.1111/j.1600-0609.2008.01050.x
- Kumar N. (2006). Copper deficiency myelopathy (human swayback). Mayo Clinic proceedings, 81(10), 1371–1384. https://doi.org/10.4065/81.10.1371
- Gregg, X. T., Reddy, V., & Prchal, J. T. (2002). Copper deficiency masquerading as myelodysplastic syndrome. Blood, 100(4), 1493–1495. https://doi.org/10.1182/blood-2002-01-0256
- Huff, J. D., Keung, Y. K., Thakuri, M., Beaty, M. W., Hurd, D. D., Owen, J., & Molnár, I. (2007). Copper deficiency causes reversible myelodysplasia. American journal of hematology, 82(7), 625–630. https://doi.org/10.1002/ajh.20864
- Jaiser, S. R., & Winston, G. P. (2010). Copper deficiency myelopathy. Journal of neurology, 257(6), 869–881. https://doi.org/10.1007/s00415-010-5511-x
- Myint, Z.W., Oo, T.H., Thein, K.Z. et al. Copper deficiency anemia: review article. Ann Hematol 97, 1527–1534 (2018). https://doi.org/10.1007/s00277-018-3407-5
- Altarelli, M., Ben-Hamouda, N., Schneider, A., & Berger, M. M. (2019). Copper Deficiency: Causes, Manifestations, and Treatment. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition, 34(4), 504–513. https://doi.org/10.1002/ncp.10328
- Kumar N. (2014). Neurologic aspects of cobalamin (B12) deficiency. Handbook of clinical neurology, 120, 915–926. https://doi.org/10.1016/B978-0-7020-4087-0.00060-7
- Prodan, C. I., Bottomley, S. S., Vincent, A. S., Cowan, L. D., Greenwood-Van Meerveld, B., Holland, N. R., & Lind, S. E. (2009). Copper deficiency after gastric surgery: a reason for caution. The American journal of the medical sciences, 337(4), 256–258. https://doi.org/10.1097/MAJ.0b013e31818ad0ff
- Nations, S. P., Boyer, P. J., Love, L. A., Burritt, M. F., Butz, J. A., Wolfe, G. I., Hynan, L. S., Reisch, J., & Trivedi, J. R. (2008). Denture cream: an unusual source of excess zinc, leading to hypocupremia and neurologic disease. Neurology, 71(9), 639–643. https://doi.org/10.1212/01.wnl.0000312375.79881.94
- Duncan, A., Yacoubian, C., Watson, N., & Morrison, I. (2015). The risk of copper deficiency in patients prescribed zinc supplements. Journal of clinical pathology, 68(9), 723–725. https://doi.org/10.1136/jclinpath-2014-202837
- Baker D. H. (1999). Cupric oxide should not be used as a copper supplement for either animals or humans. The Journal of nutrition, 129(12), 2278–2279. https://doi.org/10.1093/jn/129.12.2278
- Parrott, J., Frank, L., Rabena, R., Craggs-Dino, L., Isom, K. A., & Greiman, L. (2017). American Society for Metabolic and Bariatric Surgery Integrated Health Nutritional Guidelines for the Surgical Weight Loss Patient 2016 Update: Micronutrients. Surgery for Obesity and Related Diseases, 13(5), 727-741. https://doi.org/10.1016/j.soard.2016.12.018