Key Takeaways
- Interferon-alpha is the only PV treatment that targets the root cause. Unlike phlebotomy or hydroxyurea, recombinant interferon-alpha directly attacks the mutant stem cells driving polycythemia vera. In some patients, after 2 to 5 years of treatment, the cancer-driving mutation becomes undetectable. No other approved PV drug achieves this.
- Two randomised trials now support interferon across all patient groups. The PROUD-CONTI trial showed interferon outperformed hydroxyurea in high-risk patients. The Low-PV trial showed it outperformed phlebotomy alone in low-risk patients. Both findings contributed to FDA and European regulatory approval of ropeginterferon alfa-2b (Besremi).
- "Low-risk" does not mean no risk. Patients classified as low-risk PV still carry a blood clot risk 2 to 3 times higher than the general population. Repeated phlebotomy causes iron deficiency and can raise platelet counts, potentially adding to that risk. Watchful waiting may not be as safe as previously assumed.
- Starting treatment early matters. The earlier interferon is introduced, the lower the mutation burden and the greater the chance of achieving a deep molecular response. Delaying treatment allows the mutant cell population to grow and accumulate additional genetic changes, making remission harder to achieve over time.
This paper is a narrative review published in Leukemia (2026) by Richard T. Silver, MD and Hans Carl Hasselbalch, MD. Their review synthesises over 35 years of clinical evidence to argue that the current standard treatment for polycythemia vera (PV) is fundamentally inadequate. Where standard treatments such as phlebotomy and hydroxyurea manage symptoms without addressing the underlying disease, the authors make the case that recombinant interferon-alpha (rIFNα) is the only available therapy that directly targets the mutant stem cells driving PV, and in some patients can reduce the mutation to undetectable levels over time
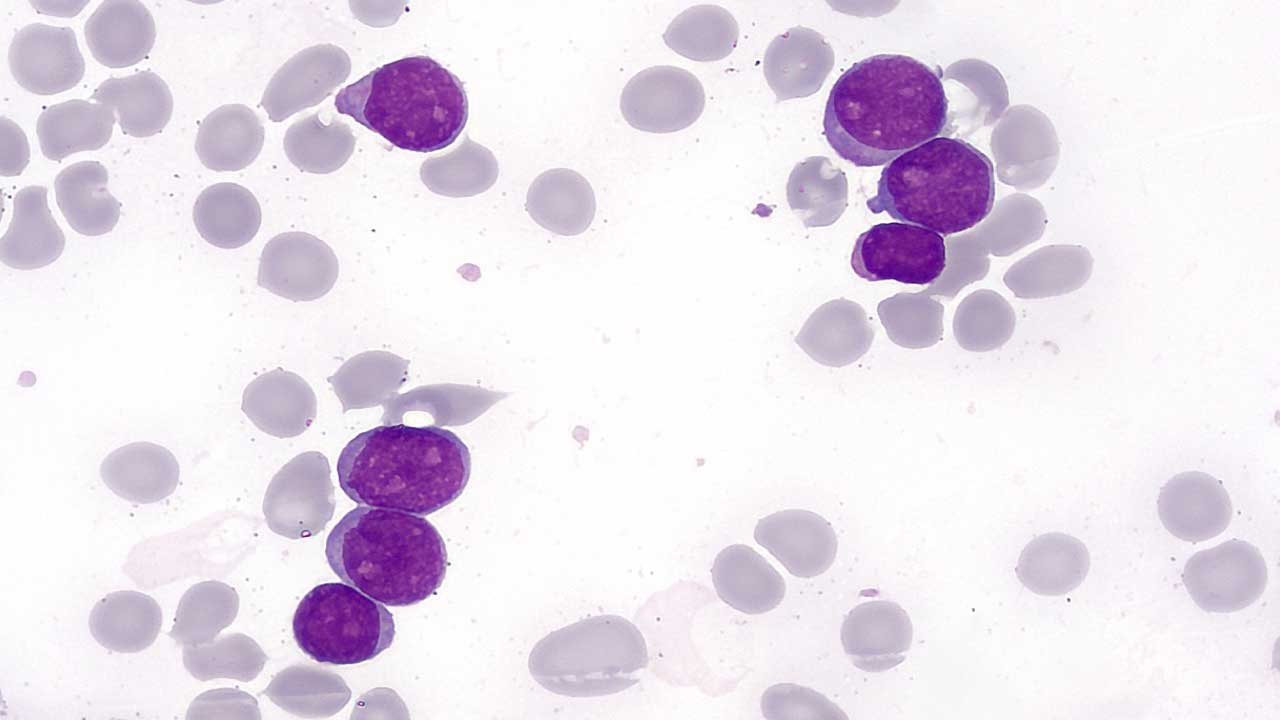
What is polycythemia vera?
Polycythemia vera (PV) is a rare but serious blood cancer in which the bone marrow produces too many red blood cells. The resulting thickening of the blood raises the risk of dangerous clots in arteries and veins. Over time, if the disease is poorly managed, it can progress to a condition called myelofibrosis (permanent scarring of the bone marrow) which dramatically worsens a patient's outlook.
For most of the past four decades, the standard approach has been straightforward: remove blood regularly through a procedure called phlebotomy, and in higher-risk patients, add a chemotherapy tablet called hydroxyurea (HU). Both approaches manage the symptoms. Neither one targets the underlying cause of the disease.
A different kind of treatment
That underlying cause, in the vast majority of PV cases, is a single genetic mutation: JAK2V617F. This "typo" in the DNA of a blood stem cell causes it and all cells descending from it to overproduce blood cells uncontrollably. Phlebotomy and hydroxyurea reduce the number of those cells. They do not reduce the number of cells carrying that mutation.
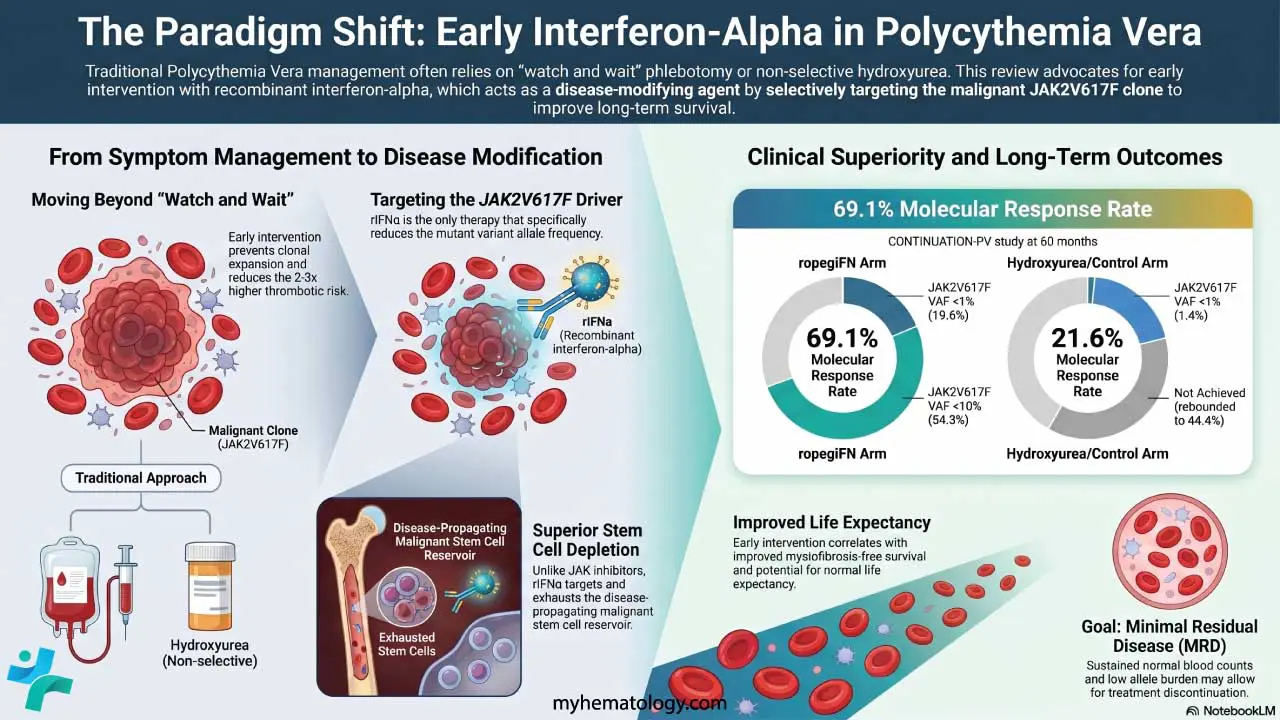
Recombinant interferon-alpha (rIFNα) does something different. Interferons are naturally occurring immune-signalling proteins that the body uses to regulate cell growth and fight abnormal cells. The lab-made version, rIFNα, appears to directly target the mutant stem cells driving PV — driving dormant mutant stem cells into active division, where they become vulnerable to stress and exhaustion. Over time, with sustained treatment, the burden of the JAK2V617F mutation measurably decreases. In a minority of patients treated for two to five years, it has become undetectable. No other approved PV drug achieves this.
Targeting JAK2 V617F with Interferon
"Interferon is the only drug used in treating PV that specifically reduces the mutant JAK2V617F variant allele frequency — a measure of how dominant the cancer-driving mutation is in the blood system."
What do the clinical trials show?
The argument for interferon rests on two pivotal randomised trials, alongside 35 years of supporting observational data.
The PROUD-CONTI trial was a Phase III randomised controlled trial comparing ropeginterferon alpha-2b (brand name Besremi — a newer, longer-acting pegylated form of interferon) against hydroxyurea in patients with high-risk PV. Ropeg outperformed HU on both blood count control and molecular response. This led to European Medicines Agency approval in 2019 and unrestricted US FDA approval in 2021, making it the first PV-specific therapy to achieve regulatory approval in either region.
The Low-PV trial, a Phase 2 randomised study, then tested ropegIFN against phlebotomy alone in patients classified as low-risk PV — patients typically under 60 years old with no prior blood clots. The results were striking: after just one year, ropegIFN was already clearly superior. This was the first randomised evidence that a disease-modifying drug outperforms phlebotomy even in patients previously considered to need only minimal treatment.
The problem with "low-risk"
One of the most significant arguments the authors make concerns the current risk classification system. PV patients are divided into "low-risk" (under 60, no prior clots) and "high-risk" (over 60 or with prior clots). Low-risk patients are frequently managed on phlebotomy and aspirin alone, under a watchful waiting approach.
The review challenges this directly. Even low-risk patients carry a blood clot risk two to three times higher than the general population. Most PV patients have symptoms at diagnosis like fatigue, itching, night sweats, and circulation disturbances regardless of which risk category they fall into. Repeated phlebotomy itself causes progressive iron deficiency, which worsens symptoms and, through a rise in platelet count (thrombocytosis), may add to the very clot risk the procedure is meant to address.
Retrospective studies suggest that patients managed on phlebotomy alone progress to bone marrow scarring (myelofibrosis) sooner than those treated with interferon or hydroxyurea. The authors argue this makes passive management not merely insufficient, but potentially harmful over time.
The case for starting early
The core proposal of the review is this: rIFNα should be offered to all newly diagnosed PV patients, both low-risk and high-risk, unless a specific reason prevents it. Treatment should begin early, ideally at diagnosis, not after phlebotomy has failed or symptoms have worsened.
The rationale follows from the biology. When the mutant cell burden is low and the disease is early, interferon has the best chance of driving the mutation toward undetectable levels. Waiting allows the mutant clone to expand and accumulate additional genetic changes, making remission progressively harder to achieve. The authors use the analogy of treating cancer early when the tumour is small — the same principle, they argue, applies here.
Practically, interferon is given as a subcutaneous (under-the-skin) injection. The two approved pegylated formulations are Besremi (ropegIFNα-2b), injected every two to four weeks, and Pegasys (pegIFNα-2a), injected weekly. The authors favour a "start low, go slow" dosing strategy (beginning at low doses and increasing gradually) to minimise side effects and improve tolerability over the long course of treatment required.
What about side effects?
Interferon is not without side effects. They fall broadly into five categories: flu-like symptoms (the most common, especially early in treatment), liver enzyme changes, thyroid disturbances, autoimmune effects, and neurological or psychiatric effects. The authors note that most of these are manageable with dose adjustments, supportive care, or temporary interruptions, and that many patients' symptoms including depression actually improve once the disease itself is being treated.
They also point out that long-term hydroxyurea is not as benign as commonly assumed. A German study found that prolonged HU use led to multiple side effects requiring discontinuation in half of patients. Interferon is contraindicated in pregnancy and requires particular care in patients with active autoimmune disease, uncontrolled psychiatric conditions, or hyperthyroidism.
How does interferon compare to JAK inhibitors like ruxolitinib?
The review also addresses a common question for students and clinicians: how does interferon differ from JAK inhibitors such as ruxolitinib, another drug used in myeloproliferative diseases? The answer is mechanistically important. Ruxolitinib primarily blocks signalling that drives myeloproliferation (overproduction of blood cells) and reduces inflammation-driven symptoms. It does not meaningfully reduce the JAK2V617F mutation burden or target the disease-propagating stem cells. Interferon does both. The two may therefore be complementary rather than competing, and early-phase combination studies are ongoing.
Where do guidelines currently stand?
Both the US National Comprehensive Cancer Network (NCCN) [1] and the European LeukemiaNet (ELN) [2] now include ropegIFN as a recommended option for both low-risk and high-risk PV. However, the strength of that recommendation for low-risk patients remains conditional in ELN guidelines, and the NCCN's low-risk endorsement is classified as a softer category II-B recommendation. Phlebotomy plus aspirin remains a first-line option for low-risk patients under current international guidelines. The review argues this is no longer scientifically justified and calls for universal early interferon as the standard of care.
Limitations to know
This is a narrative review and expert opinion, not a new clinical trial. It synthesises and advocates based on existing data.
Complete disappearance of the JAK2V617F mutation occurs in only a minority of patients, even with prolonged treatment.
Interferon's effect on additional genetic mutations beyond JAK2 (such as TET2, ASXL1, DNMT3A) is inconsistent as some mutations persist or expand during treatment.
Long-term head-to-head data comparing interferon to hydroxyurea across all patient groups over many decades remains limited.
The authors hold a clearly stated pro-interferon position; readers should weigh this alongside the broader guideline landscape.
Interferon is contraindicated in pregnancy and requires caution in patients with autoimmune disease, active psychiatric conditions, or hyperthyroidism.
Why this matters
For patients with PV, the practical implication is worth raising with a hematologist particularly for those currently managed on phlebotomy alone. The data now supports asking whether a disease-modifying treatment started early could reduce the long-term risk of clots, symptoms, and bone marrow progression.
The treatment of PV has not changed quickly. But after 35 years of accumulating data, two randomised trials, and regulatory approvals on both sides of the Atlantic, the field appears to be at a genuine inflection point.
Source: Silver RT & Hasselbalch HC. "A paradigm shift in the treatment of patients with polycythemia vera. The initial early use of recombinant interferon-alpha." Leukemia 40, 1122–1136 (2026). DOI: 10.1038/s41375-026-02882-w. Open access.
References
- National Comprehensive Cancer Network. (2024). NCCN clinical practice guidelines in oncology: Myeloproliferative neoplasms (Version 1.2024). https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
- Marchetti, M., Vannucchi, A. M., Griesshammer, M., Harrison, C., Koschmieder, S., Gisslinger, H., Álvarez-Larrán, A., De Stefano, V., Guglielmelli, P., Palandri, F., Passamonti, F., Barosi, G., Silver, R. T., Hehlmann, R., Kiladjian, J. J., & Barbui, T. (2022). Appropriate management of polycythaemia vera with cytoreductive drug therapy: European LeukemiaNet 2021 recommendations. The Lancet. Haematology, 9(4), e301–e311. https://doi.org/10.1016/S2352-3026(22)00046-1
- Gisslinger, H., Klade, C., Georgiev, P., Krochmalczyk, D., Gercheva-Kyuchukova, L., Egyed, M., Rossiev, V., Dulicek, P., Illes, A., Pylypenko, H., Sivcheva, L., Mayer, J., Yablokova, V., Krejcy, K., Grohmann-Izay, B., Hasselbalch, H. C., Kralovics, R., Kiladjian, J. J., & PROUD-PV Study Group (2020). Ropeginterferon alfa-2b versus standard therapy for polycythaemia vera (PROUD-PV and CONTINUATION-PV): a randomised, non-inferiority, phase 3 trial and its extension study. The Lancet. Haematology, 7(3), e196–e208. https://doi.org/10.1016/S2352-3026(19)30236-4
- Kiladjian, J. J., Klade, C., Georgiev, P., Krochmalczyk, D., Gercheva-Kyuchukova, L., Egyed, M., Dulicek, P., Illes, A., Pylypenko, H., Sivcheva, L., Mayer, J., Yablokova, V., Krejcy, K., Empson, V., Hasselbalch, H. C., Kralovics, R., Gisslinger, H., & PROUD-PV Study Group (2022). Long-term outcomes of polycythemia vera patients treated with ropeginterferon Alfa-2b. Leukemia, 36(5), 1408–1411. https://doi.org/10.1038/s41375-022-01528-x
- Gisslinger, H., Klade, C., Georgiev, P., Krochmalczyk, D., Gercheva-Kyuchukova, L., Egyed, M., Dulicek, P., Illes, A., Pylypenko, H., Sivcheva, L., Mayer, J., Yablokova, V., Krejcy, K., Empson, V., Hasselbalch, H. C., Kralovics, R., Kiladjian, J. J., & PROUD-PV Study Group (2023). Event-free survival in patients with polycythemia vera treated with ropeginterferon alfa-2b versus best available treatment. Leukemia, 37(10), 2129–2132. https://doi.org/10.1038/s41375-023-02008-6
- Barbui, T., Vannucchi, A. M., De Stefano, V., Carobbio, A., Ghirardi, A., Carioli, G., Masciulli, A., Rossi, E., Ciceri, F., Bonifacio, M., Iurlo, A., Palandri, F., Benevolo, G., Pane, F., Ricco, A., Carli, G., Caramella, M., Rapezzi, D., Musolino, C., Siragusa, S., … Rambaldi, A. (2023). Ropeginterferon versus Standard Therapy for Low-Risk Patients with Polycythemia Vera. NEJM evidence, 2(6), EVIDoa2200335. https://doi.org/10.1056/EVIDoa2200335