Key Takeaways
VTE is an umbrella term covering deep vein thrombosis (DVT), where a clot forms in a deep vein (usually in the leg or pelvis), and pulmonary embolism (PE), where a clot travels to the lungs. PE can be fatal without prompt treatment [1].
- Virchow's Triad ▾: Three forces drive clot formation in veins, summarized as Virchow's triad: damage to the vessel lining (endothelial injury), slow or pooled blood flow (stasis), and an increased tendency to clot (hypercoagulability) [4].
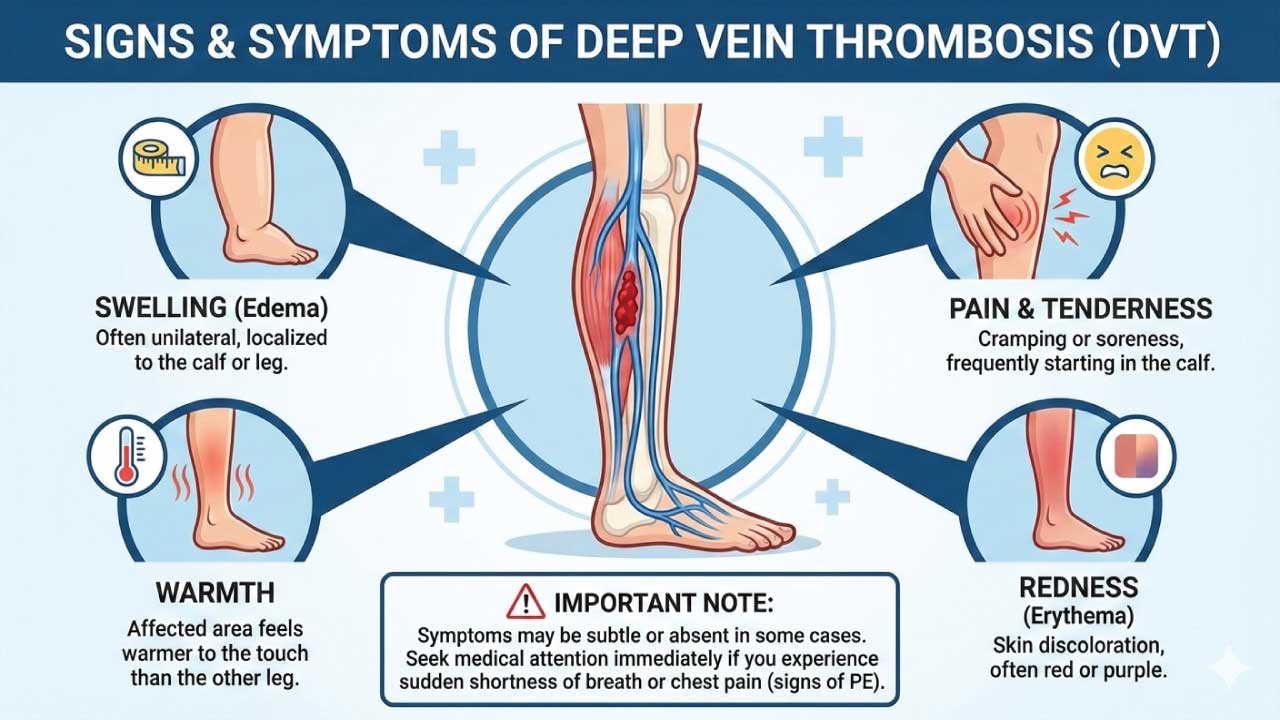
- Symptoms ▾: Classic DVT signs are one-sided leg pain, swelling, warmth, and redness. PE often presents with sudden shortness of breath and sharp chest pain that worsens on inspiration.
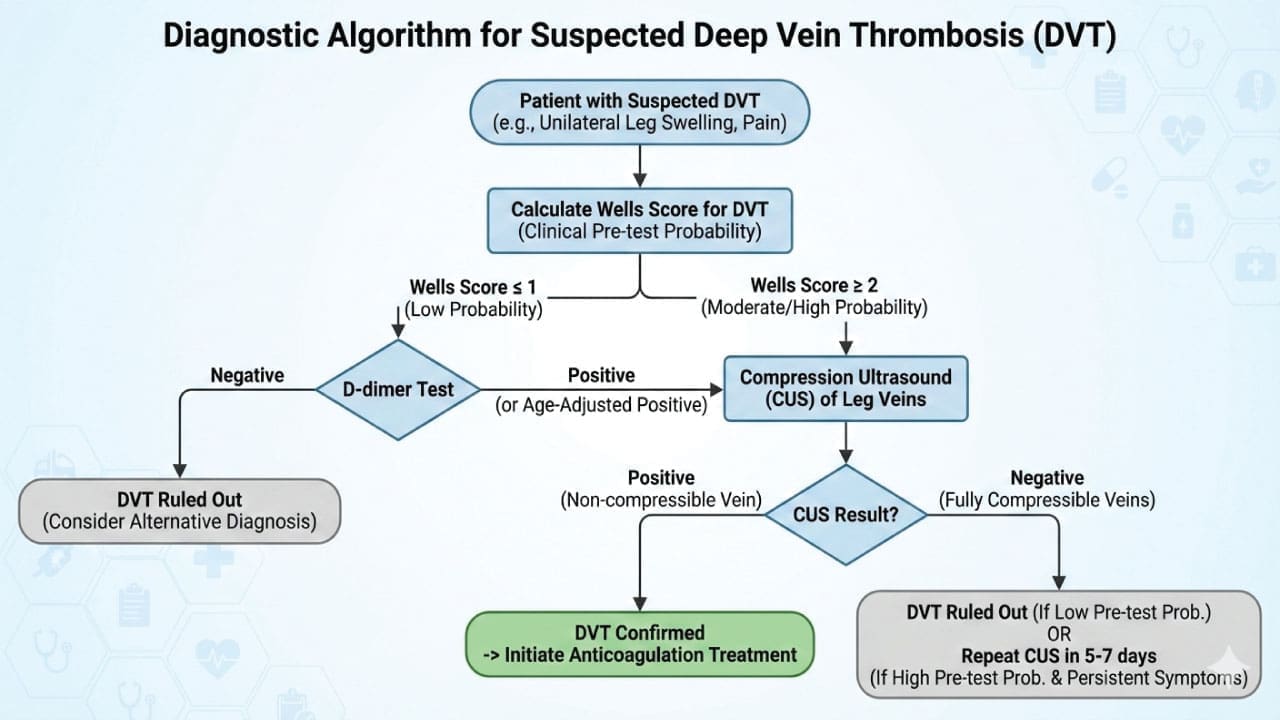
- Diagnosis ▾: Diagnosis uses a stepwise pathway: a clinical probability score (Wells, sometimes YEARS), followed by D-dimer for low-probability cases or imaging (compression ultrasound for DVT, CT pulmonary angiography for PE) for higher-probability cases [3,7].
- Treatment ▾: Direct oral anticoagulants (DOACs) are first-line treatment for most VTE patients today, replacing warfarin in routine use, with treatment lasting at least 3 months and often longer [2,3].
- Prevention ▾: VTE is largely preventable. Risk-assessment tools (Caprini for surgical patients, Padua for medical inpatients) plus mechanical or pharmacological prophylaxis cut hospital-acquired VTE rates substantially [1].
*Click ▾ for more information
What is venous thrombosis (VTE)?
Venous thromboembolism, or VTE, is the umbrella term for two linked problems:
- Deep vein thrombosis (DVT) — a clot that forms in a deep vein, most often in the calf, thigh, or pelvis.
- Pulmonary embolism (PE) — a piece of that clot breaks loose, becomes an embolus (a moving fragment), and lodges in the lung's blood vessels.
Both conditions belong to the same disease spectrum, which is why clinicians and researchers usually study them together as VTE [1].
VTE is one of the leading preventable causes of in-hospital death worldwide.
Virchow's Triad and Beyond
In 1856, Rudolf Virchow described three categories of factors that promote venous thrombosis. His framework still anchors modern teaching.
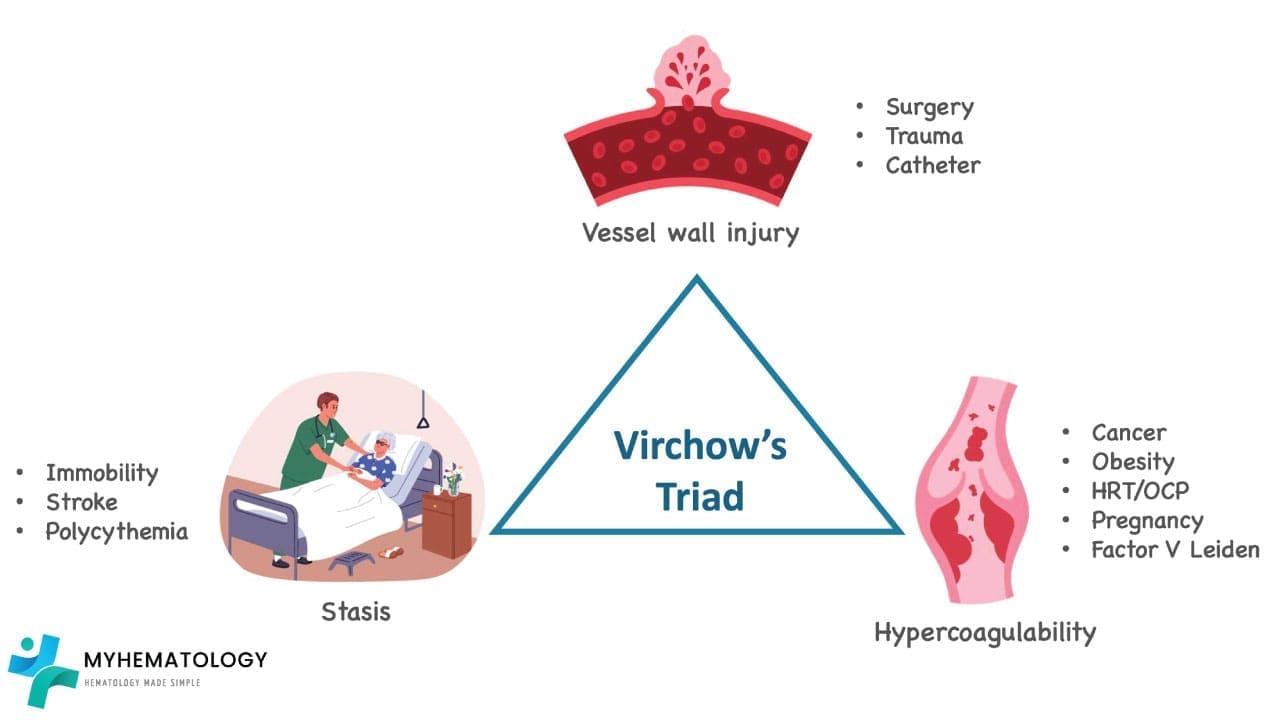
1. Endothelial Injury
The endothelium is the thin inner lining of blood vessels. When it tears or becomes inflamed, it exposes pro-clotting proteins underneath. Triggers include surgery, trauma, intravenous catheters, inflammation, and radiation therapy.
2. Stasis
Veins rely on muscle contraction and one-way valves to push blood back toward the heart. When blood slows or pools, clotting factors accumulate in the valve pockets of deep veins. Common causes include prolonged bed rest, long-haul flights, casts, obesity, pregnancy, and heart failure.
3. Hypercoagulability
Hypercoagulability means the blood clots more readily than normal. Causes can be inherited (factor V Leiden, prothrombin gene mutation, protein C or S deficiency, antithrombin deficiency) or acquired (cancer, antiphospholipid syndrome, estrogen-containing contraceptives, pregnancy, smoking, certain medications).
What Modern Research Adds
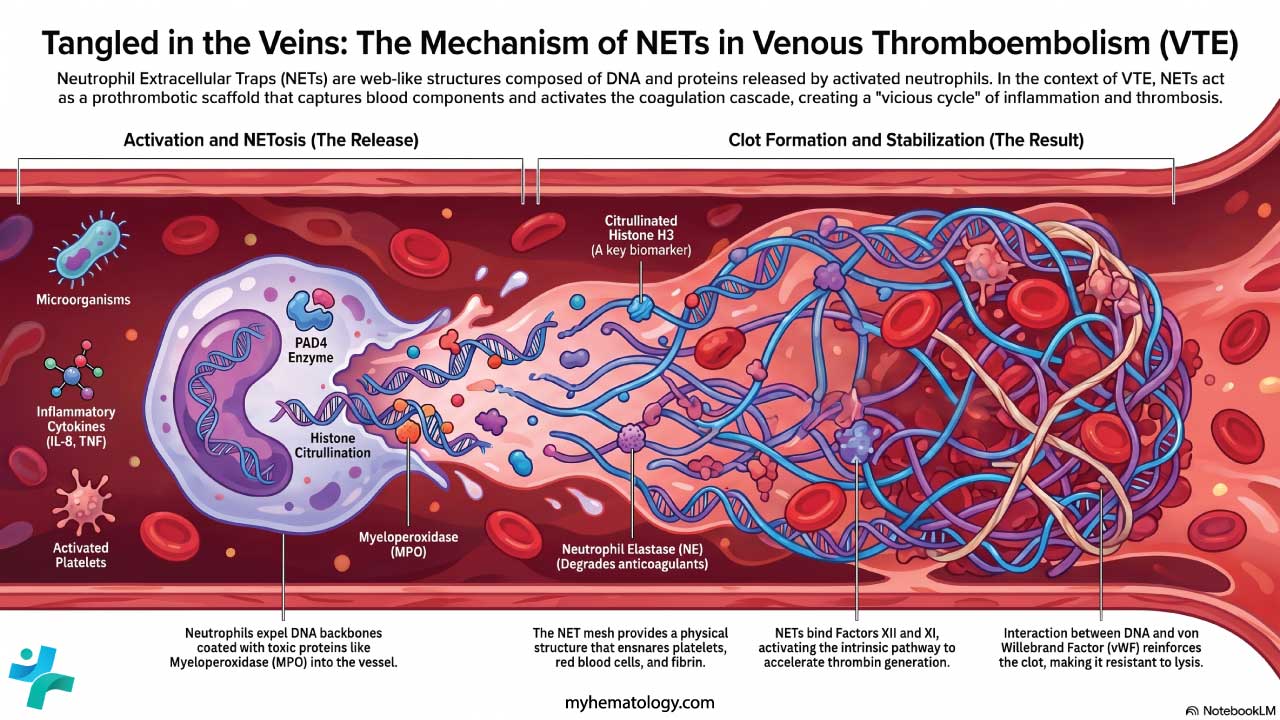
Virchow's triad is still right, but it's no longer the whole story. Recent work highlights neutrophil extracellular traps (NETs) — DNA-protein webs released by neutrophils — as active drivers of venous clot formation, especially in cancer- and infection-related VTE [4, 5]. Von Willebrand factor released from activated endothelium also helps anchor platelets and propagate the clot. These findings are why the field now talks about VTE as both an inflammatory and noninflammatory process, depending on context.
Major Risk Factors for VTE
Most VTE events involve more than one risk factor stacking up. Common contributors:
- Recent surgery, especially orthopedic (hip, knee, femur), major abdominal, pelvic, or neurosurgery
- Prolonged immobility from hospital admission, casts, or long travel
- Active cancer and cancer treatment
- Pregnancy and the postpartum period (risk is highest in the first 6 weeks after delivery)
- Estrogen-containing contraceptives and hormone replacement therapy
- Inherited thrombophilias (factor V Leiden is the most common in people of European descent)
- Previous VTE — by far the strongest single predictor of recurrence
- Age over 60, obesity, smoking, and chronic inflammatory conditions like inflammatory bowel disease
- Acute illness including severe infection. COVID-19 in particular is associated with markedly elevated VTE risk in hospitalized patients [9].
VTE Symptoms and Signs
VTE is often described as silent because early signs can be subtle. Knowing what to look for makes timely diagnosis possible.
DVT: Typical Presentation
- One-sided leg pain, often in the calf, that may feel like a deep ache or cramp
- Swelling that makes one leg visibly larger than the other
- Warmth and tenderness over the affected area
- Redness or skin discoloration
DVT: Atypical or Subtle Presentation
Some DVTs cause only vague heaviness, mild swelling noticeable only on direct comparison, or general fatigue. This is one reason the disease is so easy to miss.
PE: Warning Signs That Need Emergency Care
A pulmonary embolism is a medical emergency. Suspect PE when there is:
- Sudden shortness of breath, even at rest
- Sharp chest pain that worsens with deep breathing or coughing (pleuritic pain)
- Rapid heart rate or unexplained fainting
- Coughing up blood (hemoptysis) — uncommon but serious

Pathophysiology of VTE
Venous clots tend to form in the valve pockets of deep leg veins, where blood naturally slows. As blood pools, activated clotting factors accumulate locally and push the system toward thrombosis. The endothelium, sensing low oxygen and shear stress, releases von Willebrand factor and pro-clotting signals. Platelets stick to the exposed surface, and fibrin strands weave through the growing thrombus, trapping red blood cells [4].
Recent research adds another layer. Neutrophils recruited to the site can release NETs, which provide an additional scaffold for clot growth and resist normal breakdown by the body's fibrinolytic system [5]. This helps explain why some VTE events occur in the absence of obvious endothelial injury or classical inflammation.
If part of the clot detaches, it travels as an embolus through progressively larger veins, through the right side of the heart, and into the pulmonary arteries. Depending on its size and where it lodges, the result ranges from a small infarct to massive PE with hemodynamic collapse.

Conditions Closely Related to VTE
- Post-thrombotic syndrome (PTS): A long-term complication of DVT in which damaged vein valves cause chronic leg pain, swelling, skin changes, and sometimes ulcers. Up to one-third of DVT survivors develop some degree of PTS.
- Chronic thromboembolic pulmonary hypertension (CTEPH): A rare but serious sequela of PE in which clots fail to fully resolve, causing high pressure in the lung arteries.
- Chronic venous insufficiency: Often overlaps with PTS and reflects long-term venous valve dysfunction.
- Cerebral venous thrombosis: A less common form of VTE involving the dural venous sinuses, with distinct presentation and management.
Investigations of VTE
Modern VTE diagnosis is built around clinical probability scoring. This avoids unnecessary imaging, contrast exposure, and cost [3,6].
Step 1: Calculate the Pre-Test Probability
The Wells score is the most widely used tool. It assigns points for clinical features and stratifies patients into "likely" or "unlikely" categories (the simplified, dichotomized model is now standard).
Wells Score for Deep Vein Thrombosis (DVT)
| Clinical Feature | Points |
|---|---|
| Active cancer (current treatment, within 6 months, or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of the lower limb | +1 |
| Recently bedridden ≥3 days or major surgery within 12 weeks | +1 |
| Localized tenderness along the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling >3 cm vs. asymptomatic leg (10 cm below tibial tuberosity) | +1 |
| Pitting edema confined to the symptomatic leg | +1 |
| Collateral superficial (non-varicose) veins | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely as DVT | −2 |
Interpretation (dichotomized): ≤1 point = DVT unlikely (proceed to D-dimer). ≥2 points = DVT likely (proceed to compression ultrasound). This Wells Score for DVT calculator can be accessed here.
Wells Score for Pulmonary Embolism (PE)
| Clinical Feature | Points |
|---|---|
|
Clinical signs/symptoms of DVT
|
+3.0 |
|
PE more likely than alternative diagnosis
|
+3.0 |
|
Heart rate >100 bpm
|
+1.5 |
|
Immobilization ≥3 days or surgery within 4 weeks
|
+1.5 |
|
Previous DVT or PE
|
+1.5 |
|
Hemoptysis
|
+1.0 |
|
Malignancy (active, within 6 months, or palliative)
|
+1.0 |
Interpretation (dichotomized): ≤4 points = PE unlikely (proceed to D-dimer). >4 points = PE likely (proceed to CTPA).
In emergency settings, the PERC rule can rule out PE in very low-risk patients without any blood test, and the YEARS algorithm is increasingly used to safely reduce CTPA use [7].
Step 2: D-Dimer (When Probability Is Low)
D-dimer is a fragment released when a clot breaks down. It's sensitive but not specific as many conditions can raise it (infection, surgery, pregnancy, malignancy). A negative D-dimer in a low-probability patient effectively rules out VTE.
Age-adjusted D-dimer (age × 10 µg/L for patients over 50) reduces false positives in older adults and avoids unnecessary scans.
Step 3: Imaging (When Probability Is High or D-Dimer Is Positive)
- Compression ultrasound is the gold standard for proximal DVT. A vein that does not compress under the probe indicates clot.
- CT pulmonary angiography (CTPA) is the first-line imaging for PE. It shows clots as filling defects in the pulmonary arteries [6].
- V/Q (ventilation-perfusion) scan is reserved for patients who cannot receive contrast (severe renal impairment, severe contrast allergy, sometimes pregnancy).
- MRI and conventional venography are used in special situations.
General Treatment and Management
VTE management has shifted from inpatient warfarin protocols to outpatient DOAC therapy for most stable patients [2,3]. Treatment is divided into three phases.
Phase 1: Acute (First 5–21 Days)
Stop the clot from growing and prevent fatal PE. Options:
- DOAC with a loading dose (apixaban or rivaroxaban) — convenient, no bridging needed
- Parenteral anticoagulant (low molecular weight heparin or unfractionated heparin) bridging to warfarin or to dabigatran/edoxaban
Phase 2: Long-Term (Up to 3–6 Months)
Allow the body's own fibrinolytic system to dissolve residual clot while preventing early recurrence. Standard DOAC doses are continued.
Phase 3: Extended/Indefinite (Beyond 6 Months)
Reserved for patients with high recurrence risk. After the first 6 months, reduced-dose DOACs (apixaban 2.5 mg twice daily or rivaroxaban 10 mg daily) are widely used to balance recurrence prevention against bleeding [2].
Choosing the Right Anticoagulant
| Agent | Mechanism | Half-life | Reversal |
|---|---|---|---|
| Apixaban | Factor Xa inhibitor | ~12 h | Andexanet alfa |
| Rivaroxaban | Factor Xa inhibitor | 5–13 h | Andexanet alfa |
| Edoxaban | Factor Xa inhibitor | 10–14 h | Andexanet alfa off-label |
| Dabigatran | Direct thrombin (IIa) inhibitor | 12–17 h | Idarucizumab |
Andexanet alfa is effective at reversing factor Xa inhibitors, but the 2024 ANNEXA-I trial highlighted concerns about thrombotic events, so its use is balanced against risk [10].
While DOACs are the current standard of care, Factor XI and Factor XIa inhibitors (such as abelacimab, milvexian, and asundexian) represent the next frontier in oral anticoagulation. Currently in advanced clinical trials, these agents are designed to "uncouple" hemostasis from thrombosis thereby potentially preventing pathological clots with a significantly lower risk of bleeding than current DOACs. They are particularly anticipated for patients with high bleeding risks, such as the frail elderly or those with end-stage renal disease [11].
When to use what:
- DOACs: First-line for most provoked and unprovoked VTE [2,3]
- Low molecular weight heparin (LMWH): Preferred in pregnancy (does not cross the placenta) and remains an option in cancer-associated thrombosis, especially with luminal GI or GU tumors
- Warfarin: Used for severe renal impairment (CrCl <15–30 mL/min), mechanical heart valves, and triple-positive antiphospholipid syndrome (where DOACs are contraindicated)
Special Populations
- Cancer-associated thrombosis (CAT): Modern trials, including Caravaggio, support apixaban and other DOACs as alternatives to LMWH. However, LMWH remains the preferred agent for patients with un-resected or active luminal gastrointestinal or genitourinary cancers due to a high risk of mucosal bleeding. If the tumor has been surgically removed, DOACs are generally considered safe and effective [13].
- Antiphospholipid syndrome (triple-positive): DOACs are contraindicated. Warfarin (target INR 2.0–3.0) remains standard.
- Severe thrombocytopenia (platelets <50,000/µL): Full-dose anticoagulation may be hazardous. Reduced-dose LMWH or, rarely, a retrievable IVC filter is considered.
- Pregnancy: LMWH throughout pregnancy and at least 6 weeks postpartum.
Duration: Provoked vs. Unprovoked
- Provoked by a transient factor (surgery, trauma, immobilization): typically 3 months
- Provoked by a persistent factor (active cancer, ongoing immobility): indefinite while the factor persists
- Unprovoked: recurrence risk approaches 30% at 5 years if anticoagulation stops, so most patients with low bleeding risk continue indefinitely on a reduced-dose DOAC [2]
Adjunctive and Advanced Therapies
- Catheter-directed therapies and Mechanical Thrombectomy: Considered for intermediate-high risk or hemodynamically unstable PE, or extensive limb-threatening DVT (e.g., phlegmasia cerulea dolens). Beyond traditional catheter-directed thrombolysis (CDT), percutaneous mechanical thrombectomy (large-bore clot aspiration without the use of systemic "clot-busting" drugs) has rapidly become a primary modality. It is highly favored for patients with right ventricular strain who have contraindications to thrombolytics due to bleeding risks [12].
- Inferior vena cava (IVC) filters: Limited to patients with acute proximal DVT or PE who have an absolute contraindication to anticoagulation. Retrievable filters should be removed once anticoagulation can resume.
Preventing VTE
Prevention is one of the highest-yield topics in hospital medicine. Most hospitalized patients should be assessed using a validated risk score:
- Caprini score for surgical patients
- Padua Prediction Score for medical inpatients
Based on the score, prophylaxis options include:
- Mechanical: Graduated compression stockings, intermittent pneumatic compression devices, and early mobilization
- Pharmacological: Low-dose LMWH, low-dose DOACs, or fondaparinux
- Combined: For very high-risk patients, both mechanical and pharmacological methods
For long-haul travelers, simple measures help: walking every 1–2 hours, calf exercises during seated periods, hydration, and graduated compression stockings for higher-risk individuals.
Frequently Asked Questions (FAQs)
What is VTE in simple terms?
VTE stands for venous thromboembolism. It's an umbrella term for two related conditions: deep vein thrombosis (DVT), where a clot forms in a deep vein, usually in the leg, and pulmonary embolism (PE), where a piece of that clot travels to the lungs. Both can be serious, and PE can be fatal if untreated.
What are the early warning signs of a DVT?
The classic signs are pain, swelling, warmth, and redness in one leg, usually the calf. The leg may feel heavy or tender when pressed. Symptoms can be mild at first, so any new one-sided leg swelling lasting more than a day deserves medical attention.
When should someone with VTE go to the emergency room?
Sudden shortness of breath, sharp chest pain that worsens with breathing, coughing up blood, fainting, or a rapid heart rate can all signal a pulmonary embolism. These need emergency care immediately. For DVT alone, urgent same-day medical review is appropriate, but the ER is reserved for any suspicion of PE.
How is VTE diagnosed?
Diagnosis follows a stepwise process. A clinician calculates a clinical probability score (most often the Wells score), then uses a D-dimer blood test for low-probability cases or imaging for higher-probability cases. Compression ultrasound is the standard for DVT, and CT pulmonary angiography (CTPA) is the standard for PE.
How long do people stay on blood thinners after a VTE?
At minimum, three months. If the clot was caused by a temporary trigger like surgery, three months is often enough. If it was unprovoked or driven by ongoing factors like cancer, treatment usually continues for six months or indefinitely, often at a reduced dose.
Can VTE be prevented?
Yes, in many cases. Hospitals routinely screen patients with tools like the Caprini or Padua scores and offer prophylaxis with compression devices, low-dose anticoagulants, or both. Staying mobile after surgery, managing weight, not smoking, and discussing clot risk before starting estrogen-containing contraceptives all help reduce risk.s now use an "age-adjusted" cutoff for patients over 50 years old (calculated by multiplying the patient's age by 10 µg/L).
Glossary of Related Medical Terms
- Anticoagulant: A medication that slows clot formation. Often called a "blood thinner."
- Catheter-directed thrombolysis (CDT): A procedure that delivers clot-dissolving medication directly into the clot through a thin tube.
- D-dimer: A protein fragment released when a clot breaks down. Elevated levels suggest active clotting.
- Direct oral anticoagulant (DOAC): A class of oral blood thinners (apixaban, rivaroxaban, edoxaban, dabigatran) that block specific clotting proteins.
- Embolus: A piece of clot or other material that breaks free and travels through the bloodstream.
- Endothelium: The thin inner lining of blood vessels.
- Factor Xa: A clotting protein blocked by several DOACs.
- Fibrinolysis: The body's natural process of dissolving clots.
- Hypercoagulability: A tendency to clot more easily than normal.
- Neutrophil extracellular traps (NETs): DNA-protein webs that contribute to venous clot formation.
- Post-thrombotic syndrome (PTS): Chronic leg pain, swelling, and skin changes after a DVT.
- Pulmonary embolism (PE): A blockage in a lung artery from a traveling clot.
- Thrombus: A clot that forms inside a vessel and stays attached.
- Virchow's triad: Endothelial injury, stasis, and hypercoagulability — the three main drivers of thrombosis.
- VTE prophylaxis: Preventive measures to stop clots from forming in at-risk patients.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Lutsey, P. L., & Zakai, N. A. (2023). Epidemiology and prevention of venous thromboembolism. Nature reviews. Cardiology, 20(4), 248–262. https://doi.org/10.1038/s41569-022-00787-6
- Ortel, T. L., Neumann, I., Ageno, W., Beyth, R., Clark, N. P., Cuker, A., Hutten, B. A., Jaff, M. R., Manja, V., Schulman, S., Thurston, C., Vedantham, S., Verhamme, P., Witt, D. M., D Florez, I., Izcovich, A., Nieuwlaat, R., Ross, S., J Schünemann, H., Wiercioch, W., … Zhang, Y. (2020). American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood advances, 4(19), 4693–4738. https://doi.org/10.1182/bloodadvances.2020001830
- Stevens, S. M., Woller, S. C., Kreuziger, L. B., Bounameaux, H., Doerschug, K., Geersing, G. J., Huisman, M. V., Kearon, C., King, C. S., Knighton, A. J., Lake, E., Murin, S., Vintch, J. R. E., Wells, P. S., & Moores, L. K. (2021). Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest, 160(6), e545–e608. https://doi.org/10.1016/j.chest.2021.07.055
- Brill A. (2021). Multiple Facets of Venous Thrombosis. International journal of molecular sciences, 22(8), 3853. https://doi.org/10.3390/ijms22083853
- Smith, S. R. M., Morgan, N. V., & Brill, A. (2025). Venous thrombosis unchained: Pandora's box of noninflammatory mechanisms. Blood advances, 9(12), 3002–3013. https://doi.org/10.1182/bloodadvances.2024014114
- Konstantinides, S. V., Meyer, G., Becattini, C., Bueno, H., Geersing, G. J., Harjola, V. P., Huisman, M. V., Humbert, M., Jennings, C. S., Jiménez, D., Kucher, N., Lang, I. M., Lankeit, M., Lorusso, R., Mazzolai, L., Meneveau, N., Áinle, F. N., Prandoni, P., Pruszczyk, P., Righini, M., … The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC) (2019). 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). The European respiratory journal, 54(3), 1901647. https://doi.org/10.1183/13993003.01647-2019
- van der Hulle, T., Cheung, W. Y., Kooij, S., Beenen, L. F. M., van Bemmel, T., van Es, J., Faber, L. M., Hazelaar, G. M., Heringhaus, C., Hofstee, H., Hovens, M. M. C., Kaasjager, K. A. H., van Klink, R. C. J., Kruip, M. J. H. A., Loeffen, R. F., Mairuhu, A. T. A., Middeldorp, S., Nijkeuter, M., van der Pol, L. M., Schol-Gelok, S., … YEARS study group (2017). Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet (London, England), 390(10091), 289–297. https://doi.org/10.1016/S0140-6736(17)30885-1
- Agnelli, G., Becattini, C., Meyer, G., Muñoz, A., Huisman, M. V., Connors, J. M., Cohen, A., Bauersachs, R., Brenner, B., Torbicki, A., Sueiro, M. R., Lambert, C., Gussoni, G., Campanini, M., Fontanella, A., Vescovo, G., Verso, M., & Caravaggio Investigators (2020). Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. The New England journal of medicine, 382(17), 1599–1607. https://doi.org/10.1056/NEJMoa1915103
- Connors, J. M., & Levy, J. H. (2020). COVID-19 and its implications for thrombosis and anticoagulation. Blood, 135(23), 2033–2040. https://doi.org/10.1182/blood.2020006000
- Connolly, S. J., Sharma, M., Cohen, A. T., Demchuk, A. M., Członkowska, A., Lindgren, A. G., Molina, C. A., Bereczki, D., Toni, D., Seiffge, D. J., Tanne, D., Sandset, E. C., Tsivgoulis, G., Christensen, H., Beyer-Westendorf, J., Coutinho, J. M., Crowther, M., Verhamme, P., Amarenco, P., Roine, R. O., … ANNEXA-I Investigators (2024). Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage. The New England journal of medicine, 390(19), 1745–1755. https://doi.org/10.1056/NEJMoa2313040
- Galli, M., Laborante, R., Ortega-Paz, L., Franchi, F., Rollini, F., D'Amario, D., Capodanno, D., Tremoli, E., Gibson, C. M., Mehran, R., & Angiolillo, D. J. (2023). Factor XI Inhibitors in Early Clinical Trials: A Meta-analysis. Thrombosis and haemostasis, 123(6), 576–584. https://doi.org/10.1055/a-2043-0346
- Toma, C., Bunte, M. C., Cho, K. H., Jaber, W. A., Chambers, J., Stegman, B., Gondi, S., Leung, D. A., Savin, M., Khandhar, S., Kado, H., Koenig, G., Weinberg, M., Beasley, R. E., Roberts, J., Angel, W., Sarosi, M. G., Qaqi, O., Veerina, K., Brown, M. A., … Pollak, J. S. (2022). Percutaneous mechanical thrombectomy in a real-world pulmonary embolism population: Interim results of the FLASH registry. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions, 99(4), 1345–1355. https://doi.org/10.1002/ccd.30091
- Farge, D., Frere, C., Connors, J. M., Khorana, A. A., Kakkar, A., Ay, C., Muñoz, A., Brenner, B., Prata, P. H., Brilhante, D., Antic, D., Casais, P., Guillermo Esposito, M. C., Ikezoe, T., Abutalib, S. A., Meillon-García, L. A., Bounameaux, H., Pabinger, I., Douketis, J., & International Initiative on Thrombosis and Cancer (ITAC) advisory panel (2022). 2022 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer, including patients with COVID-19. The Lancet. Oncology, 23(7), e334–e347. https://doi.org/10.1016/S1470-2045(22)00160-7


