Procedure At A Glance
The ABO Rh test identifies a person's ABO group (A, B, AB, or O) and RhD type (positive or negative), and it is the single most important pre-transfusion test in any blood bank [1].
Key Steps ▾
- Prepare a 2–5% red cell suspension of the patient's washed red cells in saline.
- Separate the patient's plasma into a labeled tube.
- Forward grouping: add patient red cells to anti-A, anti-B, anti-A,B (optional), and anti-D. Centrifuge briefly. Read for agglutination.
- Reverse grouping: add patient plasma to known A, B, and O cells. Centrifuge briefly. Read for agglutination.
- Interpret the two patterns together. They must agree. Resolve any discrepancy before reporting.
Introduction
Every safe blood transfusion starts with a correct ABO Rh test. A mislabeled tube or a missed agglutination can trigger an acute hemolytic reaction within minutes of transfusion. The same test guides RhIG (anti-D immunoglobulin) decisions in pregnancy, organ allocation in transplantation, and antibody investigation in chronically transfused patients.
Background: The ABO and RhD Systems
The ABO Blood Group
The ABO system sorts red cells by which of two sugar antigens they carry on their surface — A, B, both, or neither. This gives four groups [2]:
- Group A: A antigen on red cells; anti-B in plasma.
- Group B: B antigen on red cells; anti-A in plasma.
- Group AB: A and B antigens on red cells; no anti-A or anti-B in plasma.
- Group O: no A or B antigen on red cells; both anti-A and anti-B in plasma.
The anti-A and anti-B antibodies in plasma are called isoagglutinins. They form naturally during infancy in response to environmental sugars that resemble the A and B antigens. They are mostly IgM and very efficient at activating complement, which is why ABO mismatch is so dangerous [1,3].
The RhD Blood Group
The RhD system is based on whether the D antigen sits on the red cell surface. RhD-positive individuals carry it; RhD-negative individuals do not. Unlike ABO, anti-D antibodies are not naturally occurring. They form only after an RhD-negative person is exposed to RhD-positive cells — through transfusion, pregnancy, or sensitization events [1].
Anti-D, when it forms, is IgG. It crosses the placenta. This is why RhD typing matters profoundly in obstetrics.
Clinical Significance of ABO Rh Test
Transfusion safety
ABO mismatch is the most common cause of fatal transfusion reactions worldwide. Pre-existing anti-A or anti-B antibodies in the recipient bind to incompatible donor red cells and trigger an acute hemolytic transfusion reaction: fever, chills, back pain, hemoglobin in the urine, kidney injury, disseminated intravascular coagulation, and sometimes death [1,3].
That is why the ABO Rh test is the first step of pre-transfusion testing and why it is performed twice on every patient in many hospitals before a unit is released.
Quick compatibility rules for red cells:
- Group A receives A or O.
- Group B receives B or O.
- Group AB receives any group.
- Group O receives only O.
- RhD-negative patients should receive RhD-negative red cells, especially women of childbearing potential.
For plasma, the rule is reversed: AB plasma is the universal donor; O plasma can only go to Group O recipients.
Type and screen, type and crossmatch, electronic crossmatch
In modern hospitals, ABO Rh testing is part of a workflow called type and screen (ABO/Rh + antibody screen) or type and crossmatch (T&S plus matching against a specific unit). When a patient has a confirmed historical ABO/Rh result and a negative antibody screen, many blood banks now release units by electronic (computer) crossmatch, skipping the physical serological crossmatch. None of this works without an accurate ABO Rh test on file [1].
Hemolytic Disease of the Fetus and Newborn (HDFN)
HDFN occurs when maternal antibodies cross the placenta and destroy fetal red cells.
Rh-HDFN is the historically severe form. An RhD-negative mother carrying an RhD-positive fetus can become sensitized during pregnancy or delivery. In a later RhD-positive pregnancy, her IgG anti-D crosses the placenta and attacks fetal red cells, causing fetal anemia, jaundice, kernicterus (bilirubin-induced brain damage), hydrops fetalis, and sometimes fetal death. Rh immunoglobulin (RhIG/RhoGAM) given antenatally and postpartum has dramatically reduced this outcome [1,3].
ABO-HDFN is usually milder. It typically affects Group A or B babies of Group O mothers, because Group O individuals produce some IgG anti-A and anti-B that can cross the placenta. Fetal red cells express ABO antigens weakly, and ABO antigens on other fetal tissues "soak up" some maternal antibody — both reasons the disease is usually less severe.
Chronic Transfusion Therapy and Molecular Genotyping
While serological tube testing is sufficient for acute scenarios, chronically transfused patients (such as those with Sickle Cell Disease or Thalassemia) require much higher resolution to prevent life-threatening alloimmunization. For these populations, standard practice now heavily emphasizes molecular RHD and RHCE genotyping over basic serology. Genotyping maps single nucleotide variants (SNVs) and hybrid rearrangements, allowing blood banks to match exact alleles rather than just the serological presence or absence of an antigen, thereby preventing the formation of complex alloantibodies [11].
Transplantation
ABO antigens sit on vascular endothelium throughout the body, so solid organ transplants must be ABO-matched to avoid hyperacute rejection. Hematopoietic stem cell transplants are more flexible because stem cells themselves do not express ABO antigens, but ABO mismatch can still cause delayed red cell engraftment or hemolysis [1].
Forensics and paternity (historical)
Both fields have been replaced by DNA-based methods. ABO typing is no longer used in modern forensics or paternity work.
Principle of ABO Rh Test (Tube Method)
The tube method uses an antigen-antibody reaction visible to the naked eye: agglutination. When antibodies in a reagent meet their matching antigen on a red cell, they bridge cells together into clumps.

Forward Grouping (Cell Grouping)
Patient red cells are mixed with known anti-A, anti-B, anti-A,B (optional), and anti-D antisera. Agglutination tells you which antigens the patient's cells carry.
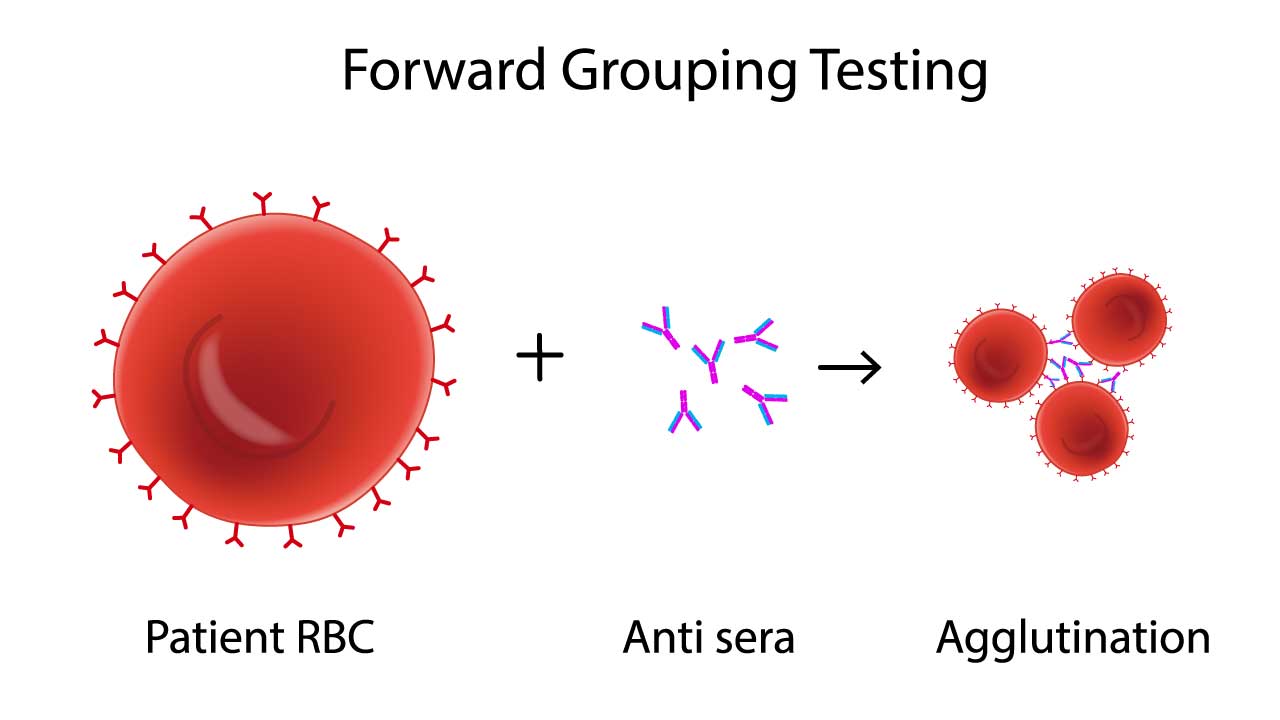
This image depicts the key principle involved in forward blood group testing, a process that determines an individual's blood type. It illustrates how antibodies in the serum react with antigens on red blood cells, causing them to clump together or "agglutinate." The pattern of agglutination reveals the person's ABO blood group, ensuring safe and effective transfusions.
Reverse Grouping (Plasma/Serum Grouping)
Patient plasma is mixed with known A cells, B cells, and O cells. Agglutination tells you which antibodies the patient's plasma contains. Reverse grouping is a built-in cross-check on forward grouping. The O cell tube acts as an autocontrol — agglutination there suggests an unexpected (alloantibody or autoantibody) reaction rather than ABO antibodies.
A note on reagents: today's commercial anti-A, anti-B, and anti-D are almost always monoclonal antibodies produced from human B-cell hybridoma lines, not pooled human plasma or animal-derived sera [1]. Modern monoclonals give consistent strength and specificity, and most anti-D reagents are blends of IgM (for direct agglutination) and IgG (for weak D detection by indirect antiglobulin testing).
Materials
- Polypropylene or glass tubes, 10 × 75 mm
- Serofuge (calibrated)
- Refrigerated centrifuge (for plasma separation)
- Pasteur pipettes
- Commercial anti-A, anti-B, anti-A,B, and anti-D antisera (monoclonal)
- Commercial known A, B, and O reagent red cells
- Patient EDTA whole blood
- Normal saline (0.9% NaCl)
Protocol
Step 1: Prepare the 2–5% red cell suspension and plasma
- Centrifuge the patient's EDTA whole blood at approximately 1000 g for 5–10 minutes in a refrigerated centrifuge.
- Label two tubes with the patient ID — one for red cell suspension, one for plasma.
- Using a Pasteur pipette, transfer the upper plasma layer into the plasma tube, avoiding the buffy coat.
- From the red cell layer, transfer one drop of packed cells into the suspension tube.
- Add saline until the tube is about three-quarters full (≈ 0.5–1 mL). Resuspend gently.
Quality check. Visually compare the suspension to a 3% commercial reference. Adjust if needed. Use the suspension on the day it is prepared.
Step 2: Forward grouping
- Label four tubes: anti-A, anti-B, anti-A,B, anti-D.
- Add one drop of the corresponding antiserum to each tube.
- Add one drop of patient red cell suspension to each tube.
- Mix gently by flicking the base.
- Centrifuge per the reagent manufacturer's instructions. A typical immediate-spin step is approximately 1000 g for 15–20 seconds in a calibrated serofuge. (Note: RPM is rotor-specific; always confirm the equivalent g-force on your serofuge.)
- Gently resuspend the cell button. Read for agglutination.
- Record results.
Step 3: Reverse grouping
- Label three tubes: A cells, B cells, O cells.
- Add one drop of the corresponding reagent red cells to each tube.
- Add two drops of patient plasma to each tube. (More plasma than cells improves antibody detection.)
- Mix gently.
- Centrifuge as in forward grouping.
- Inspect the supernatant for hemolysis (which counts as a positive result).
- Resuspend gently. Read for agglutination.
- Record results.
Step 4: Cross-check forward and reverse
Forward and reverse must match according to the table below. If they do not, you have an ABO discrepancy to resolve.
Interpretation of ABO Rh Test
Forward grouping (ABO portion)
Agglutination with each antiserum maps to a blood group as follows:
| ABO Group | Anti-A | Anti-B | Anti-A,B |
|---|---|---|---|
| Group A | + | – | + |
| Group B | – | + | + |
| Group AB | + | + | + |
| Group O | – | – | – |
Forward grouping (Rh portion)
- Agglutination in the anti-D tube → RhD positive.
- No agglutination → RhD negative (verify by weak D testing where required, e.g., donors and at-risk patients).
Reverse grouping (ABO confirmation)
| A Reagent Cells | B Reagent Cells | O Reagent Cells | Expected ABO Group |
|---|---|---|---|
| − | + | − | Group A Anti-B present in plasma |
| + | − | − | Group B Anti-A present in plasma |
| − | − | − | Group AB No anti-A or anti-B present |
| + | + | − | Group O Both anti-A and anti-B present |
Agglutination with the O reagent cells is unexpected and suggests an alloantibody or autoantibody — investigate before issuing a result.
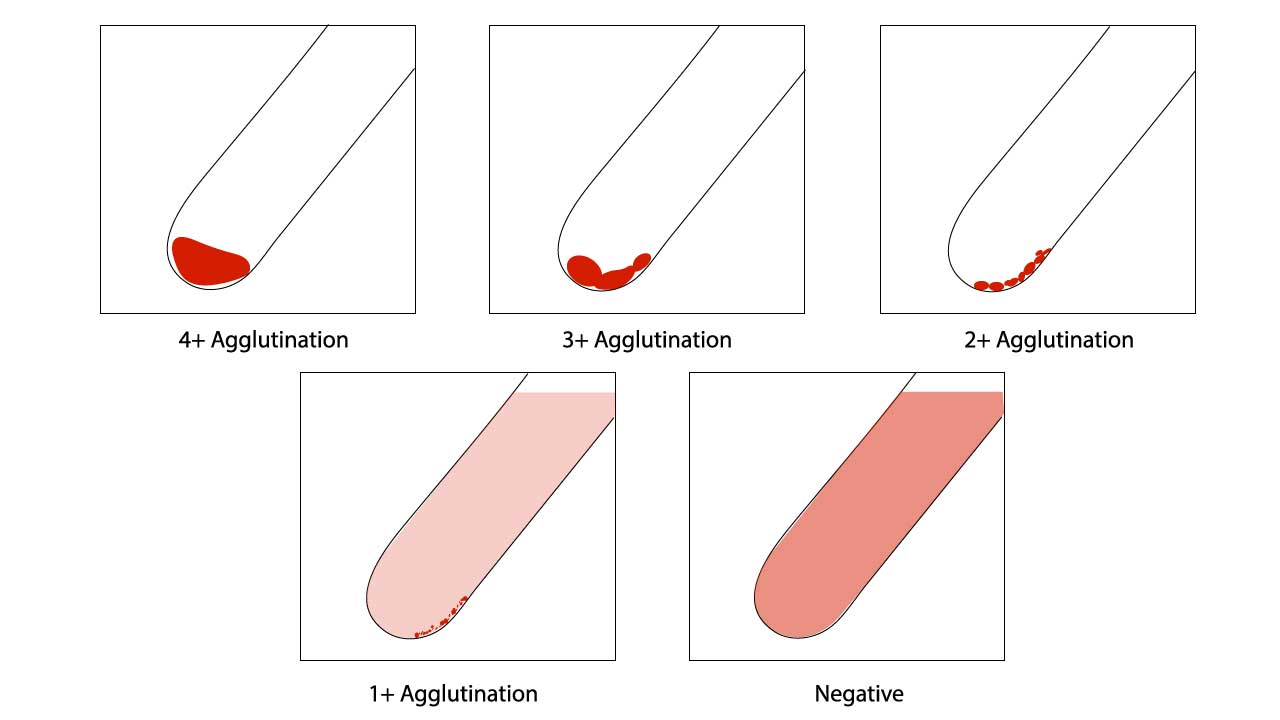
Agglutination grading
| Symbol | Score | Description | |
|---|---|---|---|
4+ (complete) |
12 | One solid cell button; clear supernatant | |
3+ |
10 | Several large clumps; clear supernatant | |
2+ |
8 | Many small clumps; clear supernatant | |
1+ |
5 | Fine granular clumps; turbid reddish supernatant | |
w (weak) |
3 | Microscopic granules only; turbid supernatant | |
0 |
0 | No agglutination; clear reddish supernatant | |
MF (mixed field) |
— | Agglutinated and unagglutinated cells together | |
H |
— | Complete hemolysis; supernatant grossly red |
Reading weak agglutination
Anything below 3+ deserves a second look. Weak reactions can mean an ABO subgroup, a weak D phenotype, a young or immunosuppressed patient, a recent large-volume transfusion, or a technical error. Mixed-field reactions are particularly important and they often indicate a recent transfusion of a different ABO group, twin chimerism, or post-stem-cell transplant.
Misclassifying a weak D as RhD-negative carries real risk, which is why blood banks utilize a dual standard for donors versus patients. For blood donors, laboratories must perform serological weak D testing; if positive, the unit is labeled RhD-positive to protect RhD-negative recipients from forming anti-D [1]. For patients, weak D testing is generally avoided because classifying a weak D recipient as RhD-positive could expose them to conventional RhD-positive blood and induce alloimmunization. Instead, patients typing RhD-negative on immediate spin are safely transfused with RhD-negative blood [10]. However, to preserve the RhD-negative blood supply and avoid unnecessary RhIG administration, current AABB and CAP guidance recommends RHD genotyping for pregnant patients with serologic weak D phenotypes 1, 2, and 3, as molecular testing confirms they can be safely managed as RhD-positive [5,10].
Troubleshooting: ABO Discrepancies
A useful framework, used widely in immunohematology teaching, sorts ABO discrepancies into four groups [6]:
Group I — Weak or missing antibodies (reverse grouping problem)
- Newborns and infants under 4–6 months (have not yet produced their own ABO antibodies).
- Elderly patients with reduced antibody production.
- Immunosuppression: chemotherapy, hypogammaglobulinemia, multiple myeloma, chronic lymphocytic leukemia, immunosuppressive drugs.
- Dilution from massive plasma exchange or large-volume IV fluids.
- ABO subgroups with anti-A1 (e.g., A2 individuals).
- Bombay (Oh) phenotype: lacks H antigen; produces strong anti-A, anti-B, and anti-H. Forward types as O but reverse reacts with all reagent cells.
Resolution: prolonged incubation at room temperature, or low-temperature (4 °C) incubation with a concurrent autocontrol to exclude cold autoantibodies.
Group II — Weak or missing antigens (forward grouping problem)
- ABO subgroups (A3, Ax, Aend, B3, Bx, Bel) — genetically weakened antigen expression.
- Disease states: leukemia, hematologic malignancies, chemotherapy.
- Acquired B phenomenon: bacterial enzymes (often colon-cancer–associated) deacetylate the A antigen, making it react weakly with anti-B. Reverts on recovery; detected with acidified anti-B.
- Massive transfusion of Group O to a non-O recipient: dilutes the patient's own red cells.
- Neonates: ABO antigens not fully developed.
- Weak D: low-density D antigen requiring IAT to confirm.
Resolution: extra incubation, anti-A,B reagent, weak D testing by IAT, washing patient cells, saliva secretor studies, or molecular genotyping.
Group III — Plasma protein abnormalities
- Rouleaux: stacking of red cells from elevated plasma proteins (multiple myeloma, Waldenström, hyperfibrinogenemia). Disperses with saline replacement.
- Cold autoantibodies: react at room temperature; cause non-specific clumping.
Resolution: saline replacement technique for rouleaux; warm the sample to 37 °C and run an autocontrol for cold autoantibodies.
Group IV — Miscellaneous
- Recent transfusion of a different ABO group (mixed-field).
- Post–stem cell transplant chimerism.
- Twin chimerism.
- Polyagglutination.
- Reagent contamination or alloantibodies to low-incidence antigens in reagent cells.
Pre-, analytical, and post-analytical errors
Before chasing biology, rule out these technical causes:
- Pre-analytical: patient misidentification, wrong tube type, contaminated or hemolyzed sample.
- Analytical: incorrect cell:antiserum ratio, under- or over-centrifugation, expired reagents, vigorous shaking when reading, poor mixing.
- Post-analytical: transcription error, subjective grading, miscommunication of results.
Resolution strategies
When forward and reverse disagree:
- Repeat the test, ideally on a fresh sample.
- Review history: age, diagnosis, transfusions, transplants, medications, pregnancy.
- Adjust incubation conditions (prolonged or 4 °C) with appropriate controls.
- Use anti-A,B to detect weak A or B subgroups.
- Run a weak D test by IAT for borderline RhD results.
- Wash patient red cells to remove interfering plasma proteins.
- Send to a reference laboratory for molecular typing if needed [6].
Tube Method in Context: How It Compares
| Feature | Tube Method | Column Agglutination (Gel) | Solid-Phase Red Cell Adherence |
|---|---|---|---|
| Setup | Tubes, serofuge | Gel cards, dedicated centrifuge/incubator | Microplates, dedicated reader |
| Reading | Visual macroscopic + microscopic | Visual or photographic | Photographic, fully automated |
| Throughput | Low to moderate | Moderate to high | High, fully automated |
| Reaction Stability | Read immediately | Stable for hours | Stable for hours |
| Strengths | Reference method; resolves discrepancies | Standardized reading; documentation | High-throughput automation |
| Limitations | Subjective reading; technique-dependent | Higher per-test cost | Higher capital cost |
In high-resource blood banks, gel and solid-phase methods now run most routine ABO Rh testing. The tube method remains the reference technique, the teaching standard, and the workhorse in resource-limited settings and for resolving complex cases [4,7].
Quality Assurance
Reliable ABO Rh testing depends on systematic QC:
- Daily reagent QC with known A1, B, and O cells against each antiserum.
- Two-person verification for all final blood type reports in many institutions.
- Proficiency testing (CAP, NEQAS, RCPA) at scheduled intervals.
- Equipment calibration: serofuge timer and RCF, centrifuge balance, pipette accuracy.
Frequently Asked Questions (FAQs)
What is the ABO Rh test and why is it done?
The ABO Rh test identifies a person's ABO group (A, B, AB, or O) and RhD type (positive or negative). It is performed before transfusion, during pregnancy, before transplantation, and any time blood compatibility is needed. The test detects antigens on red cells (forward grouping) and confirms by detecting antibodies in plasma (reverse grouping) [1].
What is the difference between forward and reverse grouping?
Forward grouping tests the patient's red cells against known antisera to identify antigens. Reverse grouping tests the patient's plasma against known A and B cells to identify antibodies. The two should match for example, a Group A person has A antigens (forward) and anti-B (reverse). Disagreement signals an ABO discrepancy that must be resolved before issuing a blood type [3].
Why is reverse grouping unreliable in newborns?
Babies under about 4 to 6 months have not yet produced their own anti-A or anti-B. Because any isoagglutinins present in neonatal plasma are almost exclusively maternal IgG that crossed the placenta, blood banks strictly prohibit performing reverse grouping on neonates. Reporting a reverse group on an infant risks fatally misidentifying the baby’s actual blood type based on the mother’s circulating antibodies. Only forward grouping is performed and reported for this age group [1,3].
What is a weak D phenotype and why does it matter?
Weak D is a phenotype in which the D antigen is present at low density on red cells, so it may not react in routine RhD testing. Misclassification as RhD-negative can lead to unnecessary RhIG use and may complicate later transfusion or pregnancy. AABB and CAP guidance recommends RHD genotyping for serologic weak D phenotypes 1, 2, and 3, particularly in pregnant patients and recipients of childbearing potential [5].
What centrifuge force is correct for the tube method?
Most serofuges run an immediate-spin step of approximately 1000 g for 15–20 seconds. RPM alone is not interchangeable between centrifuges because it depends on rotor radius. Only relative centrifugal force in g is reproducible. Always follow the reagent manufacturer's specification and the centrifuge calibration record [1].
Is the tube method still used given gel and solid-phase alternatives?
Yes. The tube method remains the reference technique and the universal teaching standard. Gel-based column agglutination and solid-phase red cell adherence have become routine in automated blood banks because they offer easier reading and high-throughput automation, but the tube method is essential for backup, resource-limited settings, and resolving discrepancies [4,7].
What happens if there is no time for an ABO Rh test in an emergency?
In a true life-threatening emergency, uncrossmatched Group O blood is issued immediately. However, due to chronic blood shortages and evolving trauma protocols, O RhD-negative blood is no longer the universal default. Current guidelines restrict O RhD-negative red cells primarily to females of childbearing potential and pediatric patients to prevent alloimmunization that could cause Hemolytic Disease of the Fetus and Newborn (HDFN). For adult males and females beyond childbearing potential (typically over 50 years of age), the standard of care is now the rapid release of O RhD-positive red cells or Low Titer O Whole Blood (LTOWB) [1,9]. Even in trauma, an ABO Rh test is performed as quickly as possible so type-specific blood can take over.
Glossary of Related Medical Terms
- Agglutination — visible clumping of red cells caused by antibody binding to surface antigens.
- Antigen — a molecule on the cell surface that the immune system can recognize.
- Antibody — a protein produced by the immune system that binds to a specific antigen.
- Antiserum — a reagent containing known antibodies, used to test for antigens.
- Forward grouping — testing the patient's red cells with known antisera.
- Reverse grouping — testing the patient's plasma with known A, B, and O cells.
- ABO discrepancy — disagreement between forward and reverse results.
- Weak D — D antigen present at low density; needs further testing to detect.
- Hemolysis — destruction of red cells releasing hemoglobin.
- HDFN — hemolytic disease of the fetus and newborn.
- Rouleaux — non-immune stacking of red cells that mimics agglutination; disperses with saline.
- Isoagglutinin — naturally occurring anti-A or anti-B in plasma.
- Monoclonal antibody — antibody from a single clone with uniform specificity; the basis of modern blood typing reagents.
- Type and screen / Type and crossmatch — pre-transfusion workflows built around ABO Rh testing.
- RCF (g) — relative centrifugal force; the standardized unit for centrifugation.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cohn CS, Delaney M, Johnson ST, Katz LM, eds. Technical Manual. 21st ed. Bethesda, MD: AABB; 2023.
- Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2261/
- Harmening DM. Modern Blood Banking & Transfusion Practices. 7th ed. Philadelphia: F.A. Davis; 2018.
- Li, H. Y., & Guo, K. (2022). Blood Group Testing. Frontiers in medicine, 9, 827619. https://doi.org/10.3389/fmed.2022.827619
- Sandler, S. G., Flegel, W. A., Westhoff, C. M., Denomme, G. A., Delaney, M., Keller, M. A., Johnson, S. T., Katz, L., Queenan, J. T., Vassallo, R. R., Simon, C. D., & College of American Pathologists Transfusion Medicine Resource Committee Work Group (2015). It's time to phase in RHD genotyping for patients with a serologic weak D phenotype. College of American Pathologists Transfusion Medicine Resource Committee Work Group. Transfusion, 55(3), 680–689. https://doi.org/10.1111/trf.12941
- Fathima S, Killeen RB. ABO Typing Discrepancies. [Updated 2025 Feb 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK585061/
- Yousuf, R., Abdul Ghani, S. A., Abdul Khalid, N., & Leong, C. F. (2018). Study on ABO and RhD blood grouping: Comparison between conventional tile method and a new solid phase method (InTec Blood Grouping Test Kit). The Malaysian journal of pathology, 40(1), 27–32.
- Younes, R., Spinella, P. C., Shea, S. M., Bailey-Kroll, L., Neal, M. D., Leeper, C., & Yazer, M. H. (2023). A rapid ABO and RhD test demonstrates high fidelity to blood bank testing for RhD typing. Transfusion, 63 Suppl 3, S208–S212. https://doi.org/10.1111/trf.17326
- Yazer, M. H., & Spinella, P. C. (2018). The use of low-titer group O whole blood for the resuscitation of civilian trauma patients in 2018. Transfusion, 58(11), 2744–2746. https://doi.org/10.1111/trf.14869
- Sandler, S. G., Chen, L. N., & Flegel, W. A. (2017). Serological weak D phenotypes: a review and guidance for interpreting the RhD blood type using the RHD genotype. British journal of haematology, 179(1), 10–19. https://doi.org/10.1111/bjh.14757
- Khandelwal A. RH genotyping by next-generation sequencing. Annals of Blood. 2022;7:22.