Key Takeaways
A blood tube is an evacuated (vacuum-sealed) container with a color-coded stopper also known as a vacutainer. The color tells you what additive is inside and what tests the tube is for.
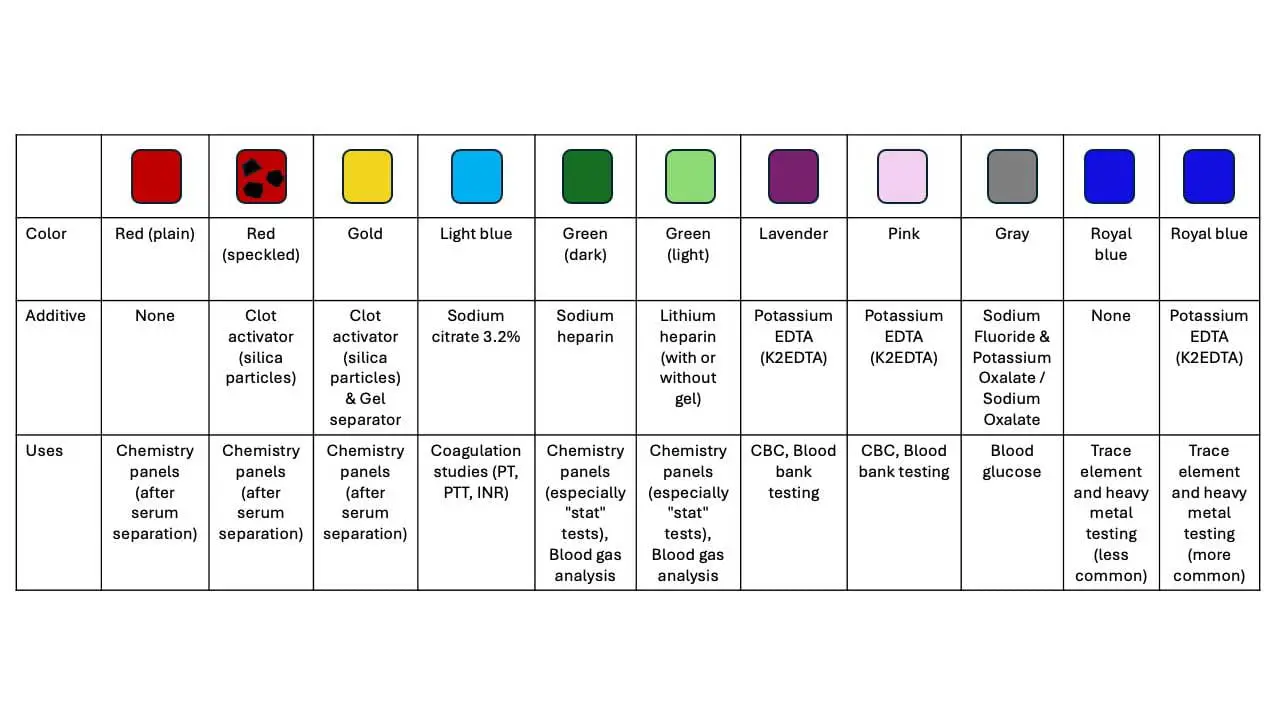
- The most common blood tube colors are light blue (citrate, for clotting tests), gold or red (serum, for chemistry), green (heparin, for plasma chemistry), lavender or pink (EDTA, for blood counts and blood bank), and gray (fluoride/oxalate, for glucose).
- Each additive works by a specific mechanism: citrate and EDTA bind calcium, heparin activates antithrombin, fluoride blocks glycolysis, and clot activators speed up clotting.
- The order of draw prevents one tube's additive from contaminating the next. Per the updated CLSI PRE02 (8th edition, 2025, formerly GP41), the standard sequence runs: blood culture → light blue → serum/SST → green → lavender/pink → gray [8].
- The biggest pre-analytical errors with blood tubes are underfilling, wrong order, insufficient mixing, and hemolysis — and most are preventable [2].
Why blood tubes matter
Most laboratory errors do not happen at the analyzer. They happen before the sample ever reaches it — during collection, labeling, mixing, or transport. These are called pre-analytical errors, and they account for the majority of preventable laboratory mistakes [2,6].
This guide walks you through each common blood tube color, what is inside it, how it works, and the tests it supports. It then explains the order of draw and the most common ways collection goes wrong.

What is a blood tube?
A blood tube is a sterile, vacuum-sealed tube used to draw a precise volume of blood from a vein. The internal vacuum pulls blood in automatically once the tube stopper is pierced. You will often hear them called "Vacutainers," but that is technically a Becton Dickinson brand name. The generic term used in laboratory standards is evacuated blood collection tube.
Every blood tube has three working parts:
- A color-coded stopper that tells you the additive inside at a glance.
- An additive that either prevents clotting (anticoagulant), promotes clotting (clot activator), or stabilizes a specific analyte (like fluoride for glucose).
- A draw volume indicated by a fill line. Reaching the correct line keeps the blood-to-additive ratio right, which is essential for accurate results.
Together, these features let one needle stick produce several samples, each prepared for a different test.
Common blood collection tubes
Serum tubes and serum separator tubes (red, speckled red, gold)
Stopper color: Red (plain), red-speckled (clot activator), or gold/tiger-top (clot activator with gel).
Additive: Plain red tubes contain no additive. Red-speckled tubes are coated on the inner wall with silica particles, a clot activator. Gold-top tubes contain the same silica plus a thixotropic gel separator.
How it works: Silica particles give clotting factors a surface to assemble on, triggering the coagulation cascade (the chain reaction that makes a clot). After centrifugation, the gel in a gold-top tube migrates to form a physical barrier between the clot and the serum above it [1].
Allow 15–30 minutes for the blood to clot fully at room temperature before centrifuging. Incomplete clotting can produce fibrin strands that interfere with analyzers, and over-vigorous handling can cause hemolysis (red cell rupture), which falsely raises potassium, LDH, and a number of other analytes [2].
Typical tests: liver function, kidney function, electrolytes, glucose (when processed quickly), lipid panels, thyroid and reproductive hormones, serology (antibody testing), therapeutic drug levels, and tumor markers.
A point of precision worth noting: a plain red tube is a serum tube, but only the gel-containing gold-top is technically a serum separator tube (SST).
Coagulation blood tube (Vacutainer) (light blue top)
Stopper color: Light blue.
Additive: Sodium citrate 3.2%, filled at a strict 9:1 ratio of blood to anticoagulant.
How it works: Citrate chelates (binds) calcium ions, and calcium is required at multiple steps of the coagulation cascade. With calcium tied up, the blood cannot clot. The action is reversible — in the lab, calcium is added back to start the reaction so clotting time can be measured [3].
The 9:1 ratio is non-negotiable. An underfilled tube concentrates the citrate and falsely prolongs PT and aPTT; an overfilled tube does the opposite. Patients with a hematocrit above ~55% need a citrate-adjusted tube, because their smaller plasma volume gets over-diluted [3]. Invert the tube gently 3–4 times immediately after collection to mix it.
If a butterfly (winged) collection set is being used and the light blue tube is the first tube drawn, a discard tube is required first to clear the air in the tubing dead space. Otherwise the first citrate tube will be underfilled and the ratio will be wrong [3,8].
Typical tests: Prothrombin time/INR (PT/INR), activated partial thromboplastin time (aPTT), D-dimer, fibrinogen, and specific clotting factor assays.
Heparin blood tube (green top)
Stopper color: Darker green for sodium heparin, lighter green for lithium heparin (with or without gel).
Additive: Sodium heparin, lithium heparin, or ammonium heparin.
How it works: Heparin binds to antithrombin (a natural anti-clotting protein) and dramatically accelerates its inactivation of thrombin and factor Xa. With these two factors switched off, fibrin cannot form and the blood stays liquid [1].
Because heparin works without removing calcium, it is well suited for chemistry tests that need rapid turnaround and for blood gas analysis, where pH and dissolved gases must not be altered.
Typical tests: STAT (immediate) chemistry panels — electrolytes, urea, creatinine, liver enzymes, amylase, lipase, lactate — arterial and venous blood gases, and cytogenetic studies for chromosome analysis. Note that heparin can interfere with PCR-based molecular tests and should not be used when DNA amplification is planned [2].
EDTA blood tube (lavender or pink top)
Stopper color: Lavender (or purple) for general hematology; pink for blood bank work.
Additive: Dipotassium EDTA (K2EDTA), the form recommended by the International Council for Standardisation in Haematology for cell counts [7].
How it works: Like citrate, EDTA binds calcium, but it binds it so tightly that the effect is essentially irreversible in the tube. (Calcium is sequestered, not destroyed.) This preserves cell shape and size with minimal change for up to 24 hours at room temperature, which is exactly what is needed for a microscopic look at blood cells [1,7].
Invert 8–10 times after collection. Even small clots will jam automated counters and produce unreliable platelet and white cell counts.
Typical tests: Complete blood count (CBC), erythrocyte sedimentation rate (ESR), blood film examination, hemoglobin A1c, ABO/Rh blood typing and crossmatching, direct antiglobulin (Coombs) test, and molecular diagnostics including PCR.
Gray top tube (glucose and lactate)
Stopper color: Gray.
Additive: Sodium fluoride plus potassium oxalate (or sodium oxalate). Newer "citrate-buffered" versions add citrate.
How it works: Sodium fluoride is an antiglycolytic agent — it blocks glycolysis, the metabolic pathway by which red and white blood cells consume glucose. Without this block, glucose in the tube would keep falling between collection and testing, producing a falsely low result. The oxalate component binds calcium to prevent clotting [1].
A current pitfall students should know: sodium fluoride alone does not stop glycolysis quickly enough. It inhibits enolase, which sits far down the glycolytic pathway, so upstream glucose breakdown continues for up to 1–4 hours after collection [4,5]. The American Diabetes Association no longer recommends NaF alone if plasma cannot be separated from cells within 30 minutes. Current best practice is either immediate ice-water cooling and centrifugation within 30 minutes, or collection into a citrate-buffered fluoride tube, which acidifies the sample and stops glycolysis almost immediately [5].
Typical tests: Fasting glucose, oral glucose tolerance testing, lactate, and sometimes blood alcohol (fluoride also prevents bacterial fermentation that could distort alcohol levels).
Cell-Free DNA (cfDNA) tubes — NIPT and liquid biopsies
Stopper color: Varies by manufacturer, but often mottled (black and tan/"camo") or glass tiger-top (e.g., Streck Cell-Free DNA BCT).
Additive: K3EDTA and a proprietary cellular preservative.
How it works: The preservative stabilizes nucleated blood cells, preventing them from lysing and releasing their genomic DNA into the plasma. This allows laboratories to isolate and analyze only the free-floating DNA naturally present in the plasma. Tubes must be kept at room temperature and inverted gently 8–10 times [9].
Typical tests: Non-invasive prenatal testing (NIPT), liquid biopsies for oncology, and specialized molecular diagnostics.
Royal blue top blood tube (trace elements and heavy metals)
Stopper color: Royal blue, in two variants — no additive (rare) or with K2EDTA (more common).
Additive: None, or K2EDTA.
How it works: Royal blue tubes are manufactured under controlled conditions to keep trace metal contamination from the tube material itself to a minimum. Even tiny amounts of lead, zinc, or aluminum from a normal tube would distort results when the test is looking for nanogram quantities of those same elements [1].
Typical tests: Heavy metals such as lead, mercury, arsenic, and cadmium; trace elements such as zinc, copper, selenium, and iodine; and certain toxicology screens.
A quick reference: tube colors at a glance
| Stopper Color | Additive | Mechanism | Common Tests |
|---|---|---|---|
Red (plain) |
None | Natural clotting | Chemistry panels (serum) |
Red speckled |
Silica clot activator | Faster clotting | Chemistry, serology |
Gold (SST) |
Silica + gel | Clot + physical barrier | Routine chemistry |
Light blue |
Sodium citrate 3.2% | Chelates calcium (reversible) | PT/INR, aPTT, D-dimer, fibrinogen |
Dark green |
Sodium heparin | Activates antithrombin | Blood gases, STAT chemistry |
Light green |
Lithium heparin (±gel) | Activates antithrombin | Chemistry panels |
Lavender |
K2EDTA | Chelates calcium | CBC, ESR, blood film, HbA1c |
Pink |
K2EDTA | Chelates calcium | Blood bank, type and crossmatch |
Gray |
NaF + oxalate (±citrate) | Blocks glycolysis + chelates calcium | Glucose, lactate, BAC |
Royal blue |
None or K2EDTA | Low-contamination tube | Heavy metals, trace elements |

Order of proper draw
Once you understand what each tube does, the next question is the order in which to fill them during a single venipuncture. The reason an order exists is carryover — tiny amounts of additive from one tube can stick to the needle and contaminate the next [8].
Example: residual EDTA carried into a heparin tube will falsely lower calcium and falsely raise potassium [2]. Residual citrate carried into an EDTA tube can alter cell counts. Following the standardized order keeps each tube's chemistry intact.
CLSI PRE02 order of draw
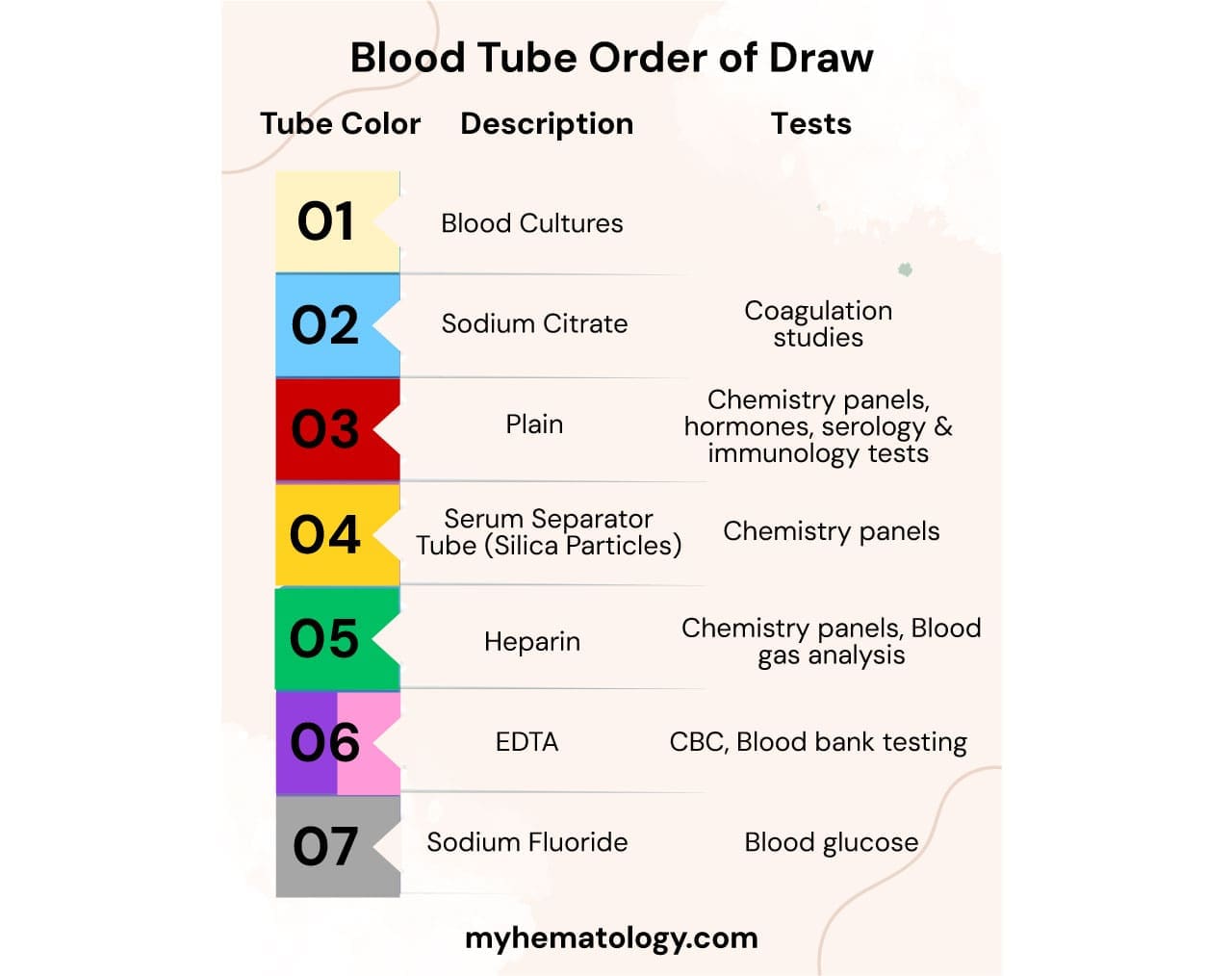
The current standard is set by the Clinical and Laboratory Standards Institute in document PRE02 (8th edition, 2025), which officially replaced the legacy GP41 standard [8]:
- Blood culture bottles (drawn first to maintain sterility)
- Light blue — sodium citrate (coagulation)
- Red, red-speckled, or gold — serum and SST
- Green — heparin
- Lavender or pink — EDTA
- Gray — fluoride/oxalate
A common mnemonic is "Boys Love Ravishing Girls Like Gold" — Blood culture, Light blue, Red/SST, Green, Lavender, Gray.
Inversions per tube
Mixing matters as much as order. CLSI PRE02 recommends:
- Blood culture bottles: 8–10 inversions
- Light blue (citrate): 3–4 inversions
- Red plain: none
- Red speckled / gold SST: 5 inversions
- Green (heparin): 8–10 inversions
- Lavender/pink (EDTA): 8–10 inversions
- Gray (fluoride/oxalate): 8–10 inversions
Each inversion is a gentle 180° turn and back — not a shake.
What goes wrong, and how to prevent it
Pre-analytical errors are the single largest source of laboratory mistakes [2,6]. Most fall into a handful of patterns:
- Underfilling. Worst for light blue (citrate) tubes, where the 9:1 ratio is critical. Always fill to the line.
- Wrong order. Causes additive carryover, which can change calcium, potassium, and clotting results.
- Insufficient mixing. Produces microclots in EDTA tubes (rejected CBCs) and localized clotting in citrate tubes (false PT/aPTT).
- Excessive mixing or rough handling. Causes hemolysis, especially in red and gold tubes.
- Prolonged tourniquet time. Beyond ~1 minute, it concentrates analytes and activates platelets and white cells [6].
- Delayed processing of glucose samples. As discussed above, NaF alone does not stop glycolysis fast enough; ice the tube or use a citrate-buffered tube if the sample cannot be processed within 30 minutes [4, 5].
- Mislabeling. The most preventable, and the most dangerous — label the tube at the bedside, in front of the patient [6, 8].
Frequently Asked Questions (FAQs)
Why does a blood draw need so many different colored tubes?
Each tube color signals a different additive inside, and each additive prepares the blood for a different kind of test. For example, EDTA (lavender top) preserves whole blood cells for a complete blood count, while sodium citrate (light blue) is needed for clotting tests. Using the wrong tube can make a test result inaccurate or unusable.
What does "order of draw" mean and why does it matter?
Order of draw is the standardized sequence in which tubes are filled during a single venipuncture. It exists to prevent the additive in one tube from carrying over into the next tube and changing results. According to CLSI guideline GP41, the order is: blood culture bottles, then light blue citrate, then red/gold serum tubes, then green heparin, then lavender/pink EDTA, then gray fluoride/oxalate.
What happens if a blood tube is not filled to the line?
Underfilling changes the ratio of blood to additive. For citrate (light blue) tubes this is critical — an underfilled tube makes PT and aPTT clotting times look falsely prolonged. Some tubes (like EDTA) tolerate slight underfilling better, but every tube should be filled to within ±10% of its draw volume.
What is the difference between serum and plasma?
Serum is the liquid left after blood has been allowed to clot, so it contains no clotting proteins. Plasma is the liquid separated from blood that was prevented from clotting (using an anticoagulant), so it still contains clotting proteins like fibrinogen. Different tests need one or the other.
Why is a gray-top tube used specifically for glucose?
Gray-top tubes contain sodium fluoride, which slows the breakdown of glucose by blood cells (glycolysis). Without it, glucose levels in the sample would keep falling during transport. More recent guidelines from the American Diabetes Association recommend tubes containing both citrate buffer and fluoride, because fluoride alone takes 1–4 hours to fully stop glycolysis.
Are "Vacutainer" and "blood tube" the same thing?
Functionally yes, but technically no. "Vacutainer" is a brand name owned by Becton Dickinson. The generic term used in guidelines is "evacuated blood collection tube." All Vacutainers are blood tubes, but not all blood tubes are Vacutainers.
Glossary of Related Medical Terms
- Additive — a substance pre-loaded into a blood tube that either prevents the blood from clotting (anticoagulant) or helps it clot faster (clot activator).
- Anticoagulant — a chemical that stops blood from clotting in the tube; examples include EDTA, citrate, and heparin.
- Antithrombin (AT) — a natural protein in blood that switches off clotting factors; heparin makes it work much faster.
- Centrifugation — spinning a blood sample at high speed so heavier cells settle to the bottom and lighter plasma or serum rises to the top.
- Chelation — when a chemical "grabs and holds" a metal ion (like calcium), keeping it out of action.
- Clot activator — a substance (usually silica particles) that triggers clotting faster than blood would clot on its own.
- Coagulation cascade — the chain of enzyme reactions that forms a blood clot.
- EDTA — ethylenediaminetetraacetic acid; an anticoagulant that binds calcium and preserves blood cells.
- Glycolysis — the metabolic pathway by which cells break down glucose for energy; continues in the tube and lowers measured glucose if not stopped.
- Hemolysis — rupture of red blood cells, releasing hemoglobin and skewing many lab results.
- Plasma — the liquid part of blood when an anticoagulant prevents clotting; still contains clotting proteins.
- Pre-analytical — anything that happens before the sample is actually analyzed (collection, labeling, transport, storage). Most lab errors happen here.
- Serum — the liquid that remains after blood has been allowed to clot; lacks clotting proteins.
- Serum separator tube (SST) — a tube containing both a clot activator and a thixotropic gel that forms a barrier between cells and serum during centrifugation.
- STAT — "immediately"; a test that must be processed without delay, often in emergency settings.
- Vacutainer — Becton Dickinson's brand name for evacuated blood tubes; often used generically.
- Venipuncture — puncturing a vein with a needle to draw blood.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Bayot ML, Tadi P. Laboratory Tube Collection. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555991/
- Bowen, R. A., & Remaley, A. T. (2014). Interferences from blood collection tube components on clinical chemistry assays. Biochemia medica, 24(1), 31–44. https://doi.org/10.11613/BM.2014.006
- Kitchen, S., Adcock, D. M., Dauer, R., Kristoffersen, A. H., Lippi, G., Mackie, I., Marlar, R. A., & Nair, S. (2021). International Council for Standardisation in Haematology (ICSH) recommendations for collection of blood samples for coagulation testing. International journal of laboratory hematology, 43(4), 571–580. https://doi.org/10.1111/ijlh.13584
- Dimeski, G., Yow, K. S., & Brown, N. N. (2015). What is the most suitable blood collection tube for glucose estimation? Annals of Clinical Biochemistry, 52(2), 270–275. https://doi.org/10.1177/0004563214544708
- Gambino R. (2013). Sodium fluoride: an ineffective inhibitor of glycolysis. Annals of clinical biochemistry, 50(Pt 1), 3–5. https://doi.org/10.1258/acb.2012.012135
- Simundic, A. M., Bölenius, K., Cadamuro, J., Church, S., Cornes, M. P., van Dongen-Lases, E. C., Eker, P., Erdeljanovic, T., Grankvist, K., Guimaraes, J. T., Hoke, R., Ibarz, M., Ivanov, H., Kovalevskaya, S., Kristensen, G. B. B., Lima-Oliveira, G., Lippi, G., von Meyer, A., Nybo, M., De la Salle, B., … Working Group for Preanalytical Phase (WG-PRE), of the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) and Latin American Working Group for Preanalytical Phase (WG-PRE-LATAM) of the Latin America Confederation of Clinical Biochemistry (COLABIOCLI) (2018). Joint EFLM-COLABIOCLI Recommendation for venous blood sampling. Clinical chemistry and laboratory medicine, 56(12), 2015–2038. https://doi.org/10.1515/cclm-2018-0602
- Nell, E. M., Bailly, J., Oelofse, D., Linström, M., Opie, J., Chapanduka, Z. C., Vreede, H., & Korf, M. (2023). Multicentre verification of haematology laboratory blood collection tubes during a global blood collection tube shortage. International journal of laboratory hematology, 45(5), 707–716. https://doi.org/10.1111/ijlh.14129
- Clinical and Laboratory Standards Institute. (2025). Collection of diagnostic venous blood specimens (CLSI standard PRE02, 8th ed.). CLSI.
- Medina Diaz, I., Nocon, A., Mehnert, D. H., Fredebohm, J., Diehl, F., & Holtrup, F. (2016). Performance of Streck cfDNA Blood Collection Tubes for Liquid Biopsy Testing. PloS one, 11(11), e0166354. https://doi.org/10.1371/journal.pone.0166354