TL;DR
Factor V Leiden thrombophilia is a genetic condition caused by a mutation in the F5 gene that results in a defective Factor V protein, making it resistant to inactivation by activated protein C (APC).
- Pathophysiology ▾: Because the mutated Factor V protein stays active for too long, it causes excessive and prolonged production of thrombin, which leads to an increased risk of blood clot formation.
- Signs and Symptoms ▾: The primary clinical consequence is venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and the life-threatening pulmonary embolism (PE). Many people with the mutation are asymptomatic unless they have other risk factors.
- Laboratory Diagnosis ▾: Diagnosis is a two-step process: an initial screening with the Activated Protein C (APC) Resistance Assay, followed by a definitive genetic test to confirm the presence of the mutation.
- Management ▾: For asymptomatic patients, no treatment is needed, but they are educated on preventive measures. For those with an acute clot, standard anticoagulant therapy is used to prevent the clot from growing or traveling. The duration of this therapy depends on the individual’s history and other risk factors.
*Click ▾ for more information
Introduction
Factor V Leiden thrombophilia is a common genetic condition that makes a person more likely to form blood clots (thrombosis). It’s the most frequently inherited cause of hypercoagulability, or an increased tendency for blood to clot.
The clinical importance of this condition lies in its connection to venous thromboembolism (VTE). People with Factor V Leiden are at a higher risk for developing deep vein thrombosis (DVT), which are clots that typically form in the deep veins of the legs, and pulmonary embolism (PE), a serious and potentially life-threatening complication that occurs when a DVT breaks off and travels to the lungs.
Definition of Factor V Leiden Thrombophilia
Factor V Leiden thrombophilia is a genetic condition caused by a specific mutation in the F5 gene, which provides instructions for making the Factor V protein. This mutation results in a modified Factor V protein that is resistant to being broken down and inactivated by activated protein C (APC), a natural anticoagulant in the body.
This resistance to inactivation means that the clotting process continues for longer than it should, leading to a higher risk of forming abnormal blood clots.
Epidemiology and Genetics
Prevalence and Demographics
Factor V Leiden is most prevalent among people of European ancestry. Approximately 3% to 8% of Caucasians carry one copy of the mutation (heterozygous). The mutation is significantly less common in other populations, including individuals of African, Hispanic, and Asian descent.
Inheritance Pattern
Factor V Leiden thrombophilia follows an autosomal dominant inheritance pattern. This means that a person only needs to inherit one copy of the mutated F5 gene from either parent to have the condition. There are two main genetic forms:
- Heterozygous: The individual inherits one mutated copy of the F5 gene and one normal copy. This is the most common form and is associated with a moderately increased risk of VTE (around 4 to 8 times the normal risk).
- Homozygous: The individual inherits two mutated copies of the F5 gene, one from each parent. This form is much rarer but is associated with a significantly higher risk of VTE (up to 80 times the normal risk).
Pathophysiology of Factor V Leiden Thrombophilia
Coagulation Cascade: An overview
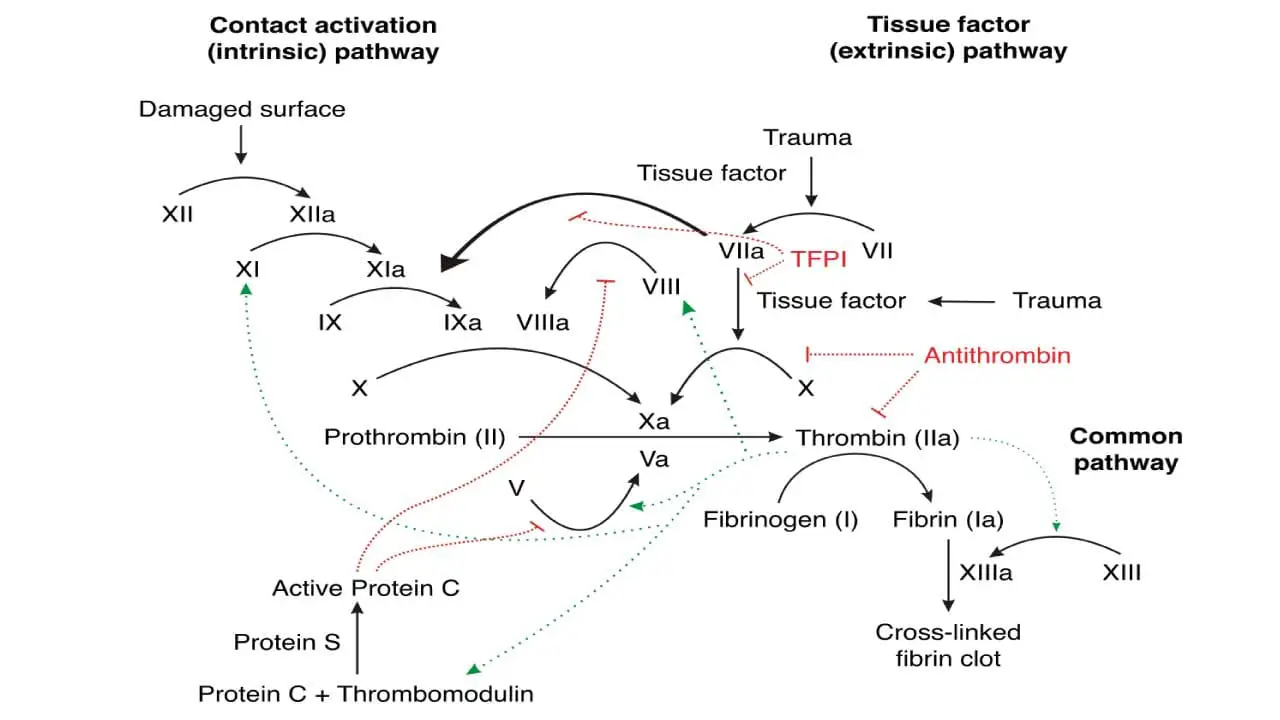
The coagulation cascade is a complex series of enzymatic reactions that leads to the formation of a blood clot. The process is a chain reaction where inactive proteins (coagulation factors) are activated sequentially. The final steps of this cascade involve the conversion of prothrombin into thrombin, which then converts soluble fibrinogen into an insoluble fibrin mesh that forms the basis of the clot.
Factor V plays a crucial role in this process. When it’s activated to Factor Va, it acts as a cofactor to dramatically increase the efficiency of the step that generates thrombin.
Specifically, Factor Va combines with Factor Xa to form a “prothrombinase complex,” which is essential for the rapid production of thrombin. Without Factor Va, thrombin generation is significantly reduced.
Activated Protein C (APC) is a natural anticoagulant that plays a critical role in regulating the coagulation cascade. Its job is to act as a “brake” on this process. It does this by inactivating two key pro-coagulant proteins: Factor Va and Factor VIIIa. By cleaving and deactivating these factors, APC slows down the production of thrombin, thereby limiting the size and duration of the blood clot.
The Mechanism of the Factor V Leiden Mutation
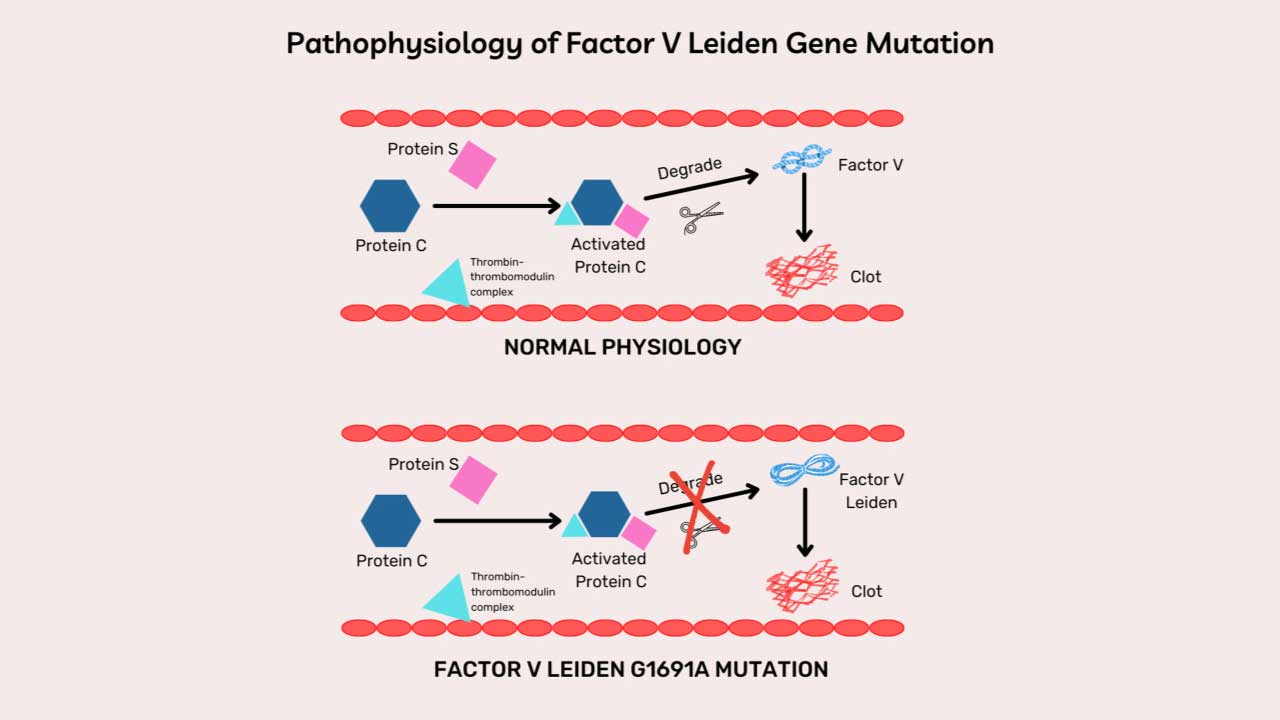
The Factor V Leiden mutation is a single-point mutation in the F5 gene. This genetic change results in a slight alteration to the Factor V protein, specifically at a site called arginine 506 (Arg506).
In a person with the mutation, this specific amino acid is replaced with another, making the Factor V protein resistant to inactivation by APC. While APC can still inactivate the protein, it does so much more slowly and inefficiently.
This resistance has a significant effect:
- The defective Factor V protein (Factor V Leiden) remains active longer than it should.
- This prolonged activity leads to excessive and prolonged thrombin generation.
- The result is a hypercoagulable state, where the blood has an increased tendency to form clots, leading to a higher risk of conditions like deep vein thrombosis (DVT) and pulmonary embolism (PE).
Signs and Symptoms of Factor V Leiden Thrombophilia
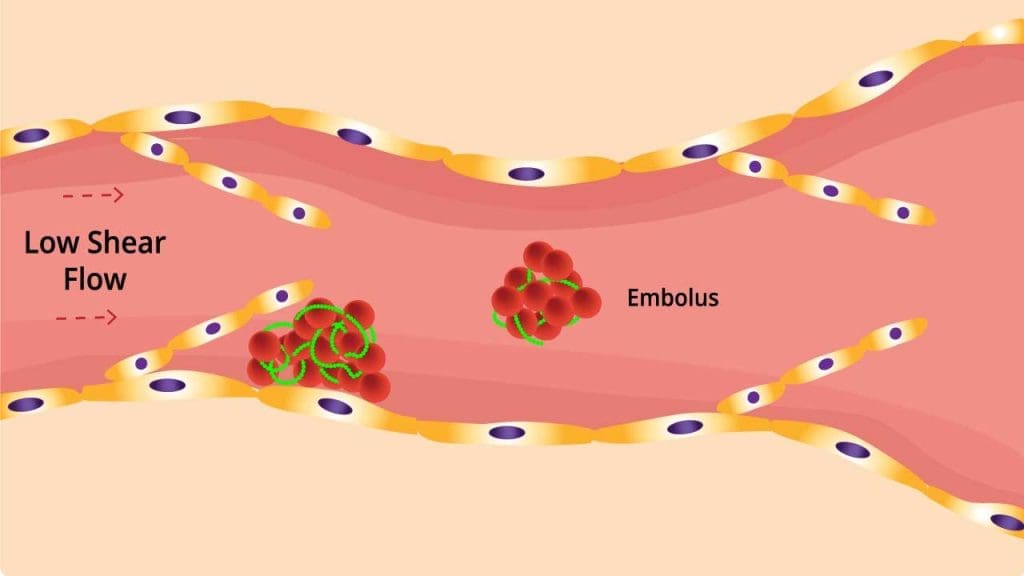
The main clinical manifestation of Factor V Leiden thrombophilia is the formation of abnormal blood clots, a process known as venous thromboembolism (VTE). This can present in two primary ways.
Deep Vein Thrombosis (DVT)

A DVT is a blood clot that forms in a deep vein, most commonly in the legs or less frequently in the arms. Symptoms often affect the limb where the clot is located.
Symptoms usually affect only one leg and may include:
- Pain or throbbing in the calf or thigh, especially when walking or standing.
- Swelling in the affected leg, ankle, or foot.
- Redness or warmth in the skin over the area of the clot.
- Tenderness when you touch the affected area.
However, some DVTs can be asymptomatic (without any symptoms).
Pulmonary Embolism (PE)
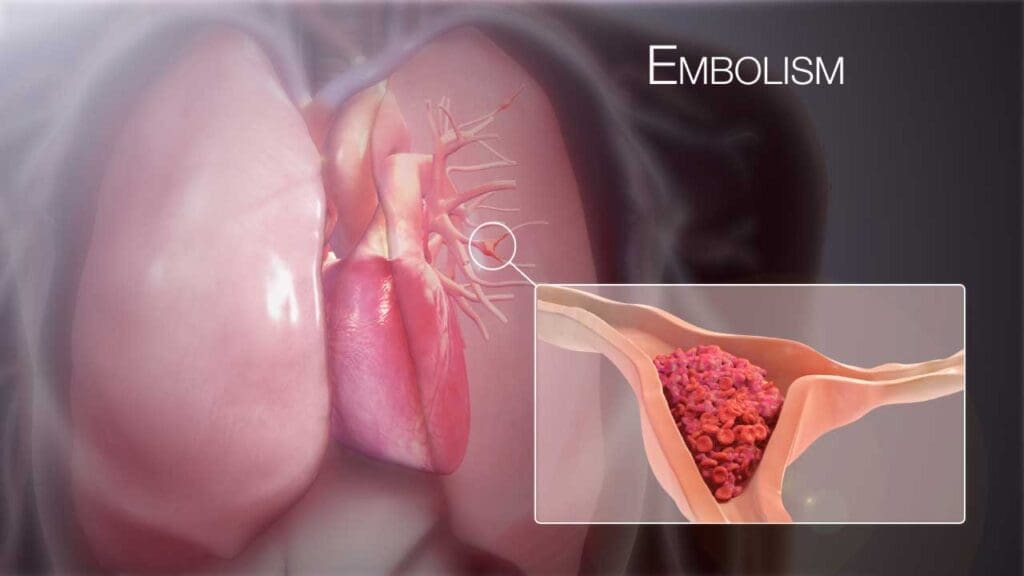
A PE is a much more serious and potentially life-threatening complication that occurs when a DVT breaks away from its original location and travels through the bloodstream to the lungs. There, it can block one of the main arteries supplying blood to the lungs.
Symptoms of a PE often come on suddenly and can be severe and may include:
- Sudden shortness of breath that is not related to activity.
- Chest pain that is sharp and may feel worse when you breathe deeply or cough.
- Coughing, which may sometimes produce blood.
- Rapid heart rate or a pounding heartbeat.
- Feeling dizzy or lightheaded, or fainting.
While Factor V Leiden significantly increases the risk of these events (DVT and PE), many people who carry the mutation never experience a clot. The condition often requires a “second hit” or additional risk factors, such as surgery, long-term immobilization (like a long plane flight), pregnancy, or the use of hormonal contraceptives, to trigger a thrombotic event.
Laboratory Investigations and Diagnosis of Factor V Leiden Thrombophilia
Activated Protein C (APC) Resistance Assay
The first step in diagnosing Factor V Leiden thrombophilia is typically a functional screening test known as the Activated Protein C (APC) Resistance Assay.
This assay measures how well a person’s plasma responds to the anticoagulant effects of activated protein C. The test involves two clotting time measurements: one with a normal amount of APC added, and one without.
In a healthy individual, the addition of APC will significantly prolong the clotting time, as it efficiently inactivates Factor V. In a person with the Factor V Leiden mutation, the clotting time is not prolonged as much (or at all) because their mutated Factor V is resistant to inactivation. The result is a lower-than-normal “APC resistance ratio,” indicating that their blood is resistant to APC’s anticoagulant effects.
Genetic Testing
If the APC resistance assay is positive (indicating resistance), a genetic test for F5 gene mutation is then performed through PCR assay to definitively confirm the diagnosis.
This test confirms the presence or absence of the specific single-point mutation at Arg506. It can also distinguish between heterozygous (one mutated gene copy) and homozygous (two mutated gene copies) forms of the disorder, which is important for risk assessment.
Other Related Laboratory Investigations
For a complete evaluation of a patient with suspected hypercoagulability, a broader thrombophilia workup is often performed. These tests look for other potential inherited or acquired clotting disorders.
- Protein C/S activity: To check for deficiencies in these natural anticoagulants.
- Antithrombin III levels: To check for a deficiency in another key coagulation inhibitor.
- Prothrombin gene mutation (G20210A): Another common inherited cause of hypercoagulability.
- Lupus anticoagulant and anticardiolipin antibodies: To screen for Antiphospholipid Syndrome, an acquired cause of clotting.
Differential Diagnosis of Factor V Leiden Thrombophilia
Other inherited and acquired causes of hypercoagulability should be considered in the differential diagnosis of Factor V Leiden Thrombophilia.
Other Inherited Causes
Several other genetic conditions can lead to hypercoagulability. These include deficiencies in natural anticoagulants, which have a similar effect to Factor V Leiden where they disrupt the body’s ability to turn off the clotting process.
- Antithrombin Deficiency: Antithrombin is a protein that inactivates thrombin and other coagulation factors. A deficiency in this protein can lead to excessive clotting.
- Protein C or Protein S Deficiencies: As with the Factor V Leiden mutation, a lack of these proteins reduces the body’s natural “off switch” for coagulation, allowing the clotting process to continue unregulated.
- Prothrombin G20210A Mutation: This is another common genetic mutation that leads to higher-than-normal levels of prothrombin, the precursor to thrombin, which increases the risk of clots.
Acquired Causes
Hypercoagulable states aren’t always genetic. Some conditions and situations can also increase a person’s risk of clotting.
- Antiphospholipid Syndrome: This is an autoimmune disorder where the body produces antibodies that attack certain proteins in the blood, leading to an increased risk of blood clots.
- Malignancy: Cancer, especially certain types, is a well-known risk factor for thrombosis. This is due to a variety of factors, including the tumor’s ability to activate the coagulation system.
- Hyperhomocysteinemia: Elevated levels of homocysteine in the blood can be a risk factor for blood clots, though the mechanism is not fully understood.
- Other Factors: A patient’s recent history is also crucial. Conditions like recent surgery, major trauma, or even prolonged immobilization (such as a long flight or bed rest) can all increase the risk of a clot and should be considered in the differential diagnosis.
Treatment and Management of Factor V Leiden Thrombophilia
Treatment and management for Factor V Leiden thrombophilia depend heavily on whether a person has experienced a blood clot. For those who are asymptomatic, the focus is on prevention.
Asymptomatic Patients
No routine treatment is needed. The primary goal is to educate the patient about their condition and potential risks.
This includes advising them on prophylactic measures, such as avoiding long periods of immobilization, staying hydrated, and potentially using prophylactic anticoagulation (like low-dose heparin) during high-risk situations such as surgery or long-distance travel.
Acute Thrombosis
When a person with Factor V Leiden experiences an acute clot, the treatment is standard anticoagulant therapy. The goal is to prevent the clot from growing and to stop it from breaking off and traveling to the lungs.
This is typically done with a combination of medications: an initial short-acting anticoagulant like heparin or a low molecular weight heparin, followed by a long-term oral medication such as warfarin or a newer class of drugs called DOACs (Direct Oral Anticoagulants).
Long-term Management
The duration of anticoagulation therapy is a critical decision that depends on several factors, including whether it was a first-time clot, if there were other risk factors involved, and the location of the clot. A person who has experienced a life-threatening PE or a recurrent clot will likely require long-term or even lifelong anticoagulation.
Special Considerations
- Pregnancy: Pregnancy significantly increases the risk of VTE. For pregnant women with Factor V Leiden, prophylactic anticoagulation is often considered, especially during the pregnancy and in the postpartum period, to minimize this risk.
- Hormonal Contraceptives: Estrogen-containing hormonal contraceptives are a major risk factor for VTE, and their use is generally advised against in individuals with Factor V Leiden due to the significantly increased risk of clot formation. Non-estrogen-based birth control methods are safer alternatives.
Frequently Asked Questions (FAQs)
Can I donate blood if I have factor V Leiden mutation?
In general, many blood donation services, particularly in the UK and Australia, allow individuals who carry the Factor V Leiden mutation to donate, provided they have never had a blood clot (thrombosis) and are not currently on blood-thinning medication. The reasoning is that for these individuals, the risk to the donor is minimal, and the risk to the recipient is considered negligible.
However, other organizations and countries may have different rules. In some cases, people with Factor V Leiden may be deferred from donating to ensure the safety of both the donor and the recipient. It’s always best to check with your specific local blood donation center to confirm their eligibility criteria for this condition.
Does factor V Leiden affect menstruation?
Factor V Leiden is an inherited condition that increases the risk of blood clotting. It does not directly affect menstruation by causing bleeding issues. In fact, some studies even suggest that carriers of the mutation may experience less menstrual blood loss.
However, if an individual with the mutation develops a blood clot (like a DVT or PE) and is prescribed anticoagulant medications (also known as blood thinners), a common side effect of these drugs can be heavier or more prolonged menstrual bleeding.
This is because the medication is designed to reduce the blood’s ability to clot, which can lead to increased bleeding during a normal physiological event like menstruation.
Therefore, while the genetic condition itself doesn’t cause menstrual problems, the treatment used for its complications can.
Can factor V Leiden cause a stroke?
Factor V Leiden is not considered a direct risk factor for stroke in most cases.
While Factor V Leiden can increase the risk of venous clots, it does not typically increase the risk of arterial clots that cause most strokes.
A very rare exception could be a paradoxical embolism, where a clot from a vein travels to the heart and then passes through a small hole (like a patent foramen ovale) into the arterial circulation, potentially leading to a stroke. However, this is not the primary or most common complication of the condition.
What are the travel guidelines for factor V Leiden?
The primary travel guideline for individuals with Factor V Leiden is to take proactive measures to prevent blood clots during prolonged periods of immobility, such as long flights, car rides, or train trips.
The risk of developing deep vein thrombosis (DVT) and pulmonary embolism (PE) increases significantly after about four hours of continuous travel.
Here are some key travel guidelines to help manage the risk:
- Move Around: Get up and walk around every 1-2 hours. On a plane, walk up and down the aisle. If you’re in a car, take frequent breaks to stretch your legs.
- Exercise Your Legs: Even while seated, you can perform simple exercises. Flex and extend your ankles, rotate your feet in circles, and press your toes and heels up and down. These movements help keep blood circulating in your lower legs.
- Stay Hydrated: Drink plenty of water throughout your trip and avoid alcohol and caffeine, as they can contribute to dehydration.
- Wear Compression Stockings: Properly fitted, knee-high compression stockings can help improve blood flow in the legs and reduce the risk of clot formation.
- Consult Your Doctor: Before a long trip, it is important to talk to your doctor. They can assess your individual risk factors and may recommend a prophylactic anticoagulant (blood thinner) for the duration of your travel. This is particularly important if you have a history of blood clots or other risk factors.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Pastori D, Menichelli D, Valeriani E, et al. Factor V Leiden Thrombophilia. 1999 May 14 [Updated 2024 May 16]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1368/
- Albagoush SA, Koya S, Chakraborty RK, et al. Factor V Leiden Mutation. [Updated 2023 Apr 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534802/
- Kujovich J. L. (2011). Factor V Leiden thrombophilia. Genetics in medicine : official journal of the American College of Medical Genetics, 13(1), 1–16. https://doi.org/10.1097/GIM.0b013e3181faa0f2
- Jehangir, W., Enakuaa, S., Udezi, V., Malik, N., Sen, S., Yousif, A., & Islam, M. (2014). Treatment for Factor V Leiden, Stuck Between a Rock and a Hard Place: A Case Report and Review of Literature. Journal Of Hematology, 3(2), 43-45.


