Procedure At a Glance
The Direct Antiglobulin Test or also known as DAT is the cornerstone laboratory test for diagnosing autoimmune hemolytic anemia, drug-induced immune hemolytic anemia, hemolytic disease of the fetus and newborn, and hemolytic transfusion reactions [4,8]
- Collect an EDTA whole blood sample.
- Wash the patient's red cells in saline 3–4 times.
- Add antihuman globulin (AHG) reagent: polyspecific, anti-IgG, and anti-C3d.
- Centrifuge briefly.
- Resuspend gently and inspect for agglutination.
- Grade any agglutination from 0 to 4+.
- Validate every negative result by adding Coombs control cells; they must agglutinate.
*Click ▾ for more information
Why the DAT Matters
When the immune system turns on its own red blood cells, the cells get coated in antibody, complement, or both, and are destroyed early. The clinical picture (anemia, jaundice, dark urine) overlaps with many other causes of hemolysis. The DAT is the test that splits immune from non-immune hemolysis at the laboratory level. For a nursing or medical student rotating through hematology or transfusion medicine, the DAT is the single result that most often anchors the diagnosis.
Principle of Direct Antiglobulin (Coombs) Test (DAT)
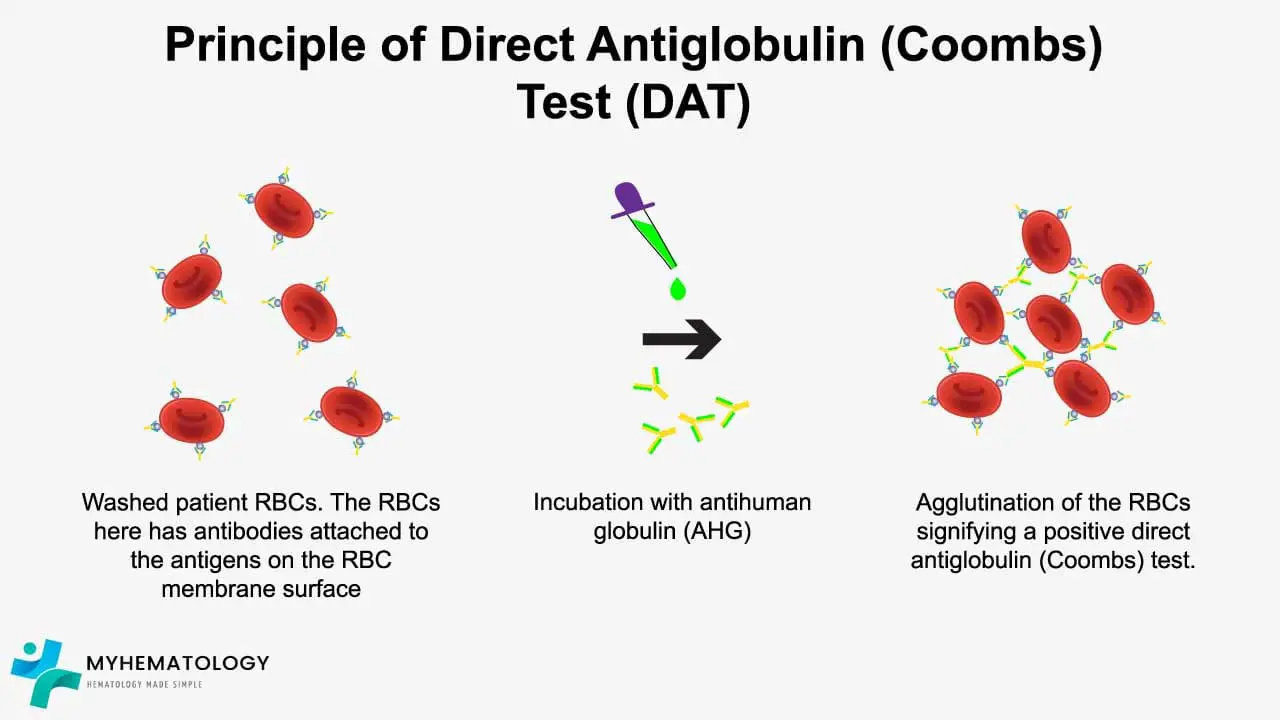
Red cells carry a net negative surface charge. In suspension they repel each other and stay apart. IgG antibodies bound to red cells are usually too small to bridge two cells across this gap on their own, so even sensitized cells often do not clump spontaneously [3,7].
This is where antihuman globulin (AHG) comes in. AHG is a reagent containing antibodies raised against human IgG and complement components. When AHG is added, each AHG molecule binds the Fc portion of an IgG already stuck to a red cell. Because AHG has two binding arms, it can grab IgG molecules on two adjacent cells at once. This cross-linking pulls cells together into visible clumps [3].
The same logic applies to complement-coated cells. Anti-C3d in the AHG reagent bridges C3d fragments on different cells.
AHG is the bridge that turns invisible antibody coating into visible agglutination.
Clinical Indications
Order a DAT when you suspect immune-mediated red cell destruction. The main indications are:
- Autoimmune hemolytic anemia (AIHA), including warm AIHA, cold agglutinin disease, and paroxysmal cold hemoglobinuria [4,6,8].
- Drug-induced immune hemolytic anemia, classically from cephalosporins, piperacillin, fludarabine, and others [5].
- Hemolytic disease of the fetus and newborn (HDFN), performed on cord blood at delivery [9].
- Hemolytic transfusion reactions, both acute and delayed.
- Investigation of unexplained hemolysis in hospitalized patients.
DAT in Pregnancy and the Newborn
Two Coombs tests run in parallel during pregnancy and after delivery, and they answer different questions.
The indirect antiglobulin test (IAT) is performed on the mother's serum during prenatal care. It looks for free antibodies, most importantly anti-D, that could cross the placenta. A positive IAT in an Rh-negative mother triggers titers, monitoring, and possibly intrauterine transfusion. Anti-D immunoglobulin (RhoGAM) is given prophylactically to non-sensitized Rh-negative mothers to prevent sensitization; it does not reverse sensitization that has already occurred.
The DAT is performed on the newborn's cord blood when there is ABO or Rh incompatibility, a positive maternal IAT, or signs of jaundice or anemia at birth [9]. A positive DAT confirms that maternal IgG has crossed the placenta and coated fetal red cells, supporting a diagnosis of HDFN and prompting bilirubin monitoring, phototherapy, or exchange transfusion as needed.
A 2025 systematic review found the DAT has moderate specificity but low sensitivity for predicting which babies will need phototherapy. It is best used alongside bilirubin trends and clinical assessment, not as a standalone predictor [14].
Materials
- Patient's EDTA-anticoagulated blood sample
- Normal saline (0.9% NaCl)
- AHG reagents: polyspecific, anti-IgG, and anti-C3d (anti-IgA, anti-IgM, anti-C3c, and anti-C4 reagents are available for atypical workup)
- Glass test tubes (or column agglutination gel cards / solid-phase strips, depending on method)
- Calibrated centrifuge
- Coombs control cells (IgG-sensitized red cells)
Protocol (Conventional Tube Method)
- Add a few drops of well-mixed EDTA blood to a clean tube. Wash the red cells in saline 3 to 4 times, decanting completely after each spin. Resuspend to a 3–5% suspension.
- Label four tubes: Polyspecific, Anti-IgG, Anti-C3d, Negative Control.
- Add 1 drop of the washed red cell suspension to each tube.
- Add 2 drops of the matching AHG reagent to the first three tubes. Add 2 drops of saline to the negative control.
- Mix gently by flicking the tube.
- Centrifuge for 15–20 seconds at 1000–1500 RPM (follow the manufacturer's settings).
- Resuspend the cell button gently. Read agglutination macroscopically, then microscopically if needed.
- Grade agglutination from 0 to 4+.
- If the result is negative, add Coombs control cells to that tube and recentrifuge. Visible agglutination confirms the test is valid; lack of agglutination invalidates the result and the test must be repeated.
*Optional 37°C incubation: some protocols include a 5-minute incubation at 37°C for the polyspecific and anti-C3d tubes to enhance complement detection. Follow your laboratory's standard operating procedure.
Method Comparison: Tube vs Gel Column vs Solid Phase
The DAT can be performed by three main techniques. Knowing which is in use in your laboratory is more useful than memorizing one.
| Method | Principle | Sensitivity | Where used |
| Conventional tube | Cells and AHG mixed in a tube; agglutination read after centrifugation. | Standard reference. | Teaching labs, low-throughput settings. |
| Column agglutination (gel card) | Sensitized cells fail to filter through a gel matrix containing AHG and stay on top. | Higher than tube, with better standardization. | Most modern transfusion services [7,10]. |
| Solid phase | Sensitized cells adhere across the surface of a coated well. | Sensitive but more false positives. | High-throughput automated platforms. |
* Gel microcolumn DAT can detect red-cell-bound antibodies that conventional tube DAT misses, and has helped diagnose AIHA cases that were previously DAT-negative [10].
Direct Antiglobulin (Coombs) Test (DAT) Interpretation
Positive Direct Antiglobulin (Coombs) Test (DAT)
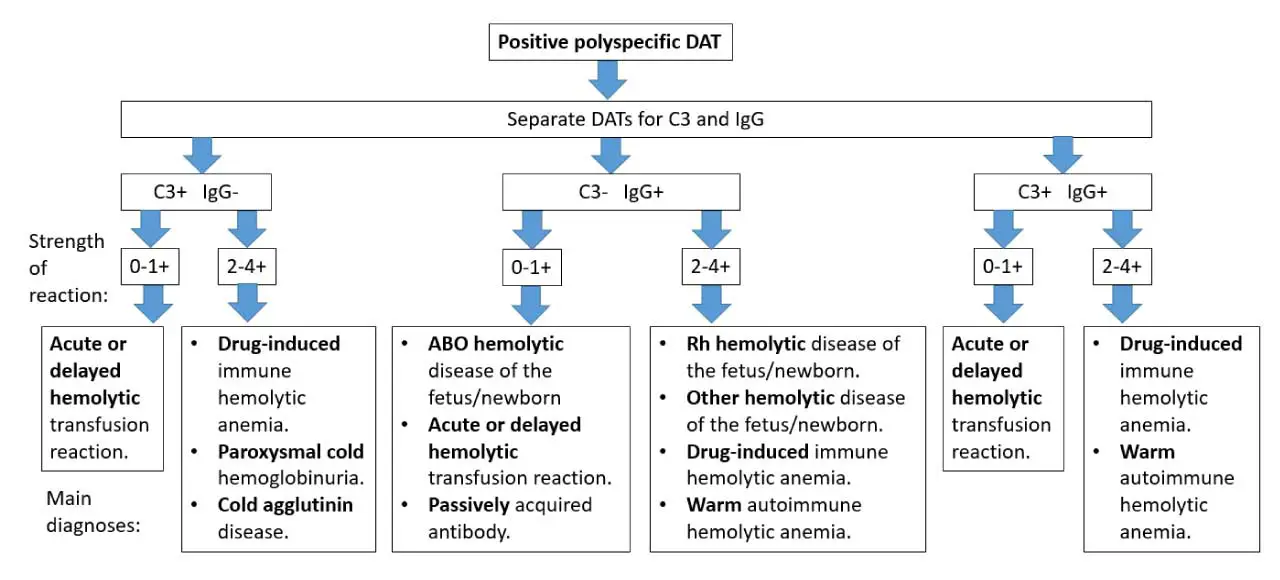
Agglutination indicates that antibodies, complement, or both are bound to the patient's red cells in vivo. The pattern across the three reagents narrows the cause:
- IgG only positive → typical of warm AIHA, drug-induced immune hemolytic anemia, HDFN.
- C3d only positive → typical of cold agglutinin disease.
- IgG and C3d positive → mixed AIHA or warm AIHA with complement activation; associated with more severe disease [8].
The strength of agglutination (0 to 4+) gives a rough estimate of how heavily coated the cells are.
Negative Direct Antiglobulin (Coombs) Test (DAT)
No agglutination suggests no significant antibody or complement coating. It does not exclude immune hemolysis. Around 5–10% of AIHA cases are routine DAT-negative because the antibody is below detection threshold, is IgA or IgM (not in standard reagents), or has a low affinity that washes off [4,8]. Suspected DAT-negative AIHA is investigated with an extended DAT panel (often termed a "Super Coombs test"), gel card DAT, or flow cytometry [11].
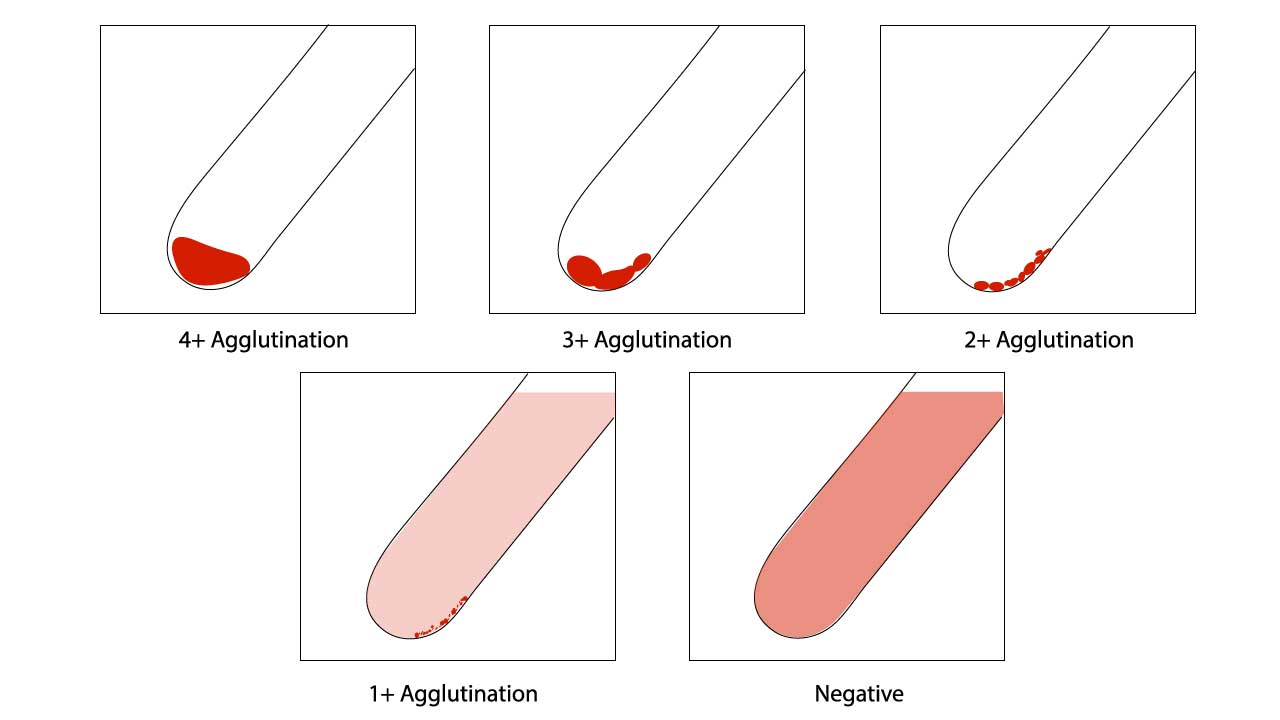
Assessment of red cell agglutination test grading
| Symbol | Description |
| 4+ / Complete (C) | One solid clump, clear supernatant. |
| 3+ | Several large clumps, clear supernatant. |
| 2+ | Many medium clumps, clear supernatant. |
| 1+ | Many small clumps, turbid red supernatant. |
| weak (w) | Only microscopically visible fine granules of the cell button and the supernatant is turbid.Tiny clumps visible only under microscope. |
| 0 | No clumps; even, cloudy red suspension. |
| MF (mixed field) | A mixture of agglutinated and unagglutinated cells together. Suggests recent transfusion or chimerism. |
| H | Complete hemolysis; supernatant grossly red, no intact cells. |
Function of Coombs Control Cells (CCC)
Coombs control cells are IgG-coated red cells that should agglutinate when AHG is added. They check that:
- The AHG reagent was added.
- The AHG reagent is active and not expired.
- Washing was thorough enough to remove free antibody (residual antibody would neutralize the AHG and cause a false negative).
If CCC fails to agglutinate, the negative DAT is invalid and the test must be repeated.
Causes of Positive DAT
A positive DAT is not a diagnosis on its own. It points to a category of causes that must be narrowed clinically.
- Autoimmune hemolytic anemia: warm AIHA, cold agglutinin disease, paroxysmal cold hemoglobinuria, mixed [4,6,8].
- Hemolytic disease of the fetus and newborn: maternal IgG against fetal antigens.
- Drug-induced immune hemolytic anemia: cephalosporins, piperacillin, fludarabine, methyldopa, and others [5].
- Hemolytic transfusion reactions: acute (ABO incompatibility) or delayed (alloantibody to minor antigens).
- Passive antibody transfer: IVIG, anti-D immunoglobulin, ATG, and intravenous Rh immunoglobulin can produce a positive DAT without hemolysis.
- Drug interference (Note on Daratumumab): Daratumumab, an anti-CD38 monoclonal antibody used in multiple myeloma, classically causes severe panreactive interference with the indirect antiglobulin test (IAT) and crossmatching because reagent red cells strongly express CD38. It does not typically cause a positive DAT because a patient's mature red blood cells have very low CD38 expression. Blood banks treat reagent red cells with dithiothreitol (DTT) to bypass the IAT interference [12].
- Solid organ and bone marrow transplantation: passenger lymphocyte syndrome and donor-recipient minor incompatibilities.
- Infections: cytomegalovirus, Epstein-Barr virus, mycoplasma, and others can cause transient positivity.
- Lymphoproliferative disorders: chronic lymphocytic leukemia, lymphomas, myelofibrosis [4].
- Healthy donors: roughly 1 in 1,000 to 1 in 14,000 healthy blood donors have a positive DAT with no hemolysis.
Limitations and Pitfalls
False negatives most often come from technique:
- Inadequate washing (residual free antibody neutralizes AHG).
- Delay between washing and adding AHG (bound antibody may dissociate).
- Inactive or expired AHG reagent.
- Antibody below the detection threshold of the tube method.
- IgA or IgM autoantibodies not detected by routine polyspecific and anti-IgG reagents [10].
False positives can come from:
- Cord blood contaminated with Wharton's jelly.
- Refrigerated samples picking up cold agglutinins.
- High serum protein states (hypergammaglobulinemia).
- Drug interference (daratumumab is the classic modern example).
- Septicemia or recent IV contrast in some cases.
A clean technique and a properly run CCC step prevent most of these problems.
How DAT Results Guide Management
The DAT pattern feeds directly into treatment decisions in AIHA [4,6]:
- Warm AIHA (IgG ± C3d positive): corticosteroids first line; rituximab or splenectomy second line.
- Cold agglutinin disease (C3d positive, often strong): avoid cold exposure; rituximab-based regimens; sutimlimab (anti-C1s, FDA-approved 2022) for chronic disease.
- Drug-induced immune hemolytic anemia: stop the offending drug; supportive care.
- HDFN: phototherapy, IVIG, or exchange transfusion based on bilirubin and hemoglobin trajectory.
- Emerging Therapies: The landscape is rapidly evolving with newer targeted agents like proximal complement inhibitors (e.g., pegcetacoplan, sutimlimab) and Bruton's tyrosine kinase (BTK) inhibitors (e.g., rilzabrutinib), actively changing how refractory AIHA is managed [13].
This is why the DAT is more than a yes/no test. The pattern across reagents tells the clinician which arm of the immune system is involved and shapes therapy.
Frequently Asked Questions (FAQs)
What is a direct antiglobulin test (DAT) used for?
The DAT detects antibodies or complement proteins already attached to a patient's red blood cells inside the body. It is the central test for diagnosing immune-mediated hemolysis, including autoimmune hemolytic anemia, drug-induced immune hemolytic anemia, hemolytic disease of the fetus and newborn, and acute or delayed hemolytic transfusion reactions.
What is the difference between a direct and indirect Coombs test?
The direct Coombs test (DAT) checks for antibodies already stuck to the patient's red cells. The indirect Coombs test (IAT) checks for free antibodies floating in plasma that have the potential to attack red cells later. The DAT is used to investigate hemolysis happening now; the IAT is used for antibody screening before transfusion and during pregnancy.
Can a DAT be positive without hemolysis?
Yes. Up to 8–15% of hospitalized patients can have a positive DAT with no evidence of hemolysis. Causes include clinically insignificant low-level antibodies, recent transfusion, certain drugs (such as daratumumab, IVIG, or anti-D immunoglobulin), high serum protein levels, and underlying conditions like systemic lupus erythematosus. A positive DAT must always be interpreted alongside hemoglobin, reticulocyte count, lactate dehydrogenase, haptoglobin, bilirubin, and the blood film.
Can a DAT be negative even when immune hemolysis is happening?
Yes. Around 5–10% of autoimmune hemolytic anemia cases have a routine negative DAT. This can occur when the antibody is below the test's detection threshold, when the autoantibody is IgA or IgM (not covered by standard reagents), or when low-affinity IgG washes off during processing. Enhanced methods such as gel card DAT, anti-IgA reagents, or flow cytometry can confirm the diagnosis.
What does a positive DAT mean for a newborn?
A positive DAT in a newborn indicates that maternal antibodies have crossed the placenta and attached to the baby's red cells. This is the laboratory hallmark of hemolytic disease of the fetus and newborn, most often from ABO or Rh incompatibility. A positive result triggers monitoring of bilirubin and hemoglobin levels and may guide the use of phototherapy or, in severe cases, exchange transfusion. Recent evidence suggests the DAT alone has limited accuracy for predicting which babies will need phototherapy, so clinicians use it with bilirubin trends and clinical signs.
Why do we wash the red cells before adding AHG?
Washing removes free antibodies and plasma proteins that did not bind to the red cells. If they are not washed away, they neutralize the AHG reagent and cause a false-negative result. Adequate washing (usually three to four times with saline) is the most common technical determinant of an accurate DAT.
Glossary of Related Medical Terms
- Agglutination — visible clumping of red blood cells caused by antibodies bridging multiple cells.
- Antihuman globulin (AHG) — a reagent containing antibodies that bind to human IgG and complement; sometimes called Coombs reagent.
- Autoantibody — an antibody made by a person's immune system that targets the body's own cells, in this case red blood cells.
- C3d — a fragment of complement protein C3 that remains attached to the red cell surface after complement activation; a marker of past or ongoing complement-mediated damage.
- Coombs control cells (CCC) — IgG-coated red cells used to confirm that AHG reagent and washing steps are working in a negative test.
- DAT (direct antiglobulin test) — laboratory test that detects antibodies or complement already attached to a patient's red cells.
- EDTA — an anticoagulant used in blood collection tubes that prevents in vitro complement activation; the preferred sample type for DAT.
- Hemolysis — destruction of red blood cells, releasing hemoglobin into plasma.
- IAT (indirect antiglobulin test) — companion test that detects free antibodies in plasma that could attack red cells later.
- IgG, IgM, IgA — immunoglobulin classes; IgG and IgA usually cause warm hemolysis, IgM usually causes cold hemolysis.
- In vivo — occurring inside the body, as opposed to in vitro (in the test tube).
- Polyspecific AHG — a Coombs reagent that detects both IgG and complement in one step.
- Sensitization — coating of red cells with antibody or complement, with or without immediate destruction.
Spherocyte — small, round red cell without central pallor; a clue to immune or hereditary hemolysis on a blood film.
Disclaimer: This protocol is intended for informational purposes only and may need to be modified depending on the specific laboratory procedures and patient circumstances. Always consult with a qualified healthcare professional for guidance. See additional information.
References
- American Association of Blood Banks (AABB). Technical Manual, 21st Edition, 2023.
- Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2261/
- Bain BJ, Bates I, Laffan MA. Dacie and Lewis Practical Haematology: Expert Consult: Online and Print 12th Edition (Elsevier). 2016.
- Hill, Q. A., Stamps, R., Massey, E., Grainger, J. D., Provan, D., Hill, A., & British Society for Haematology (2017). The diagnosis and management of primary autoimmune haemolytic anaemia. British journal of haematology, 176(3), 395–411. https://doi.org/10.1111/bjh.14478
- Hill, Q. A., Stamps, R., Massey, E., Grainger, J. D., Provan, D., Hill, A., & British Society for Haematology Guidelines (2017). Guidelines on the management of drug-induced immune and secondary autoimmune, haemolytic anaemia. British journal of haematology, 177(2), 208–220. https://doi.org/10.1111/bjh.14654
- Jäger, U., Barcellini, W., Broome, C. M., Gertz, M. A., Hill, A., Hill, Q. A., Jilma, B., Kuter, D. J., Michel, M., Montillo, M., Röth, A., Zeerleder, S. S., & Berentsen, S. (2020). Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting. Blood reviews, 41, 100648. https://doi.org/10.1016/j.blre.2019.100648
- Zantek, N. D., Koepsell, S. A., Tharp, D. R., Jr, & Cohn, C. S. (2012). The direct antiglobulin test: a critical step in the evaluation of hemolysis. American journal of hematology, 87(7), 707–709. https://doi.org/10.1002/ajh.23218
- Loriamini, M., Cserti-Gazdewich, C., & Branch, D. R. (2024). Autoimmune Hemolytic Anemias: Classifications, Pathophysiology, Diagnoses and Management. International journal of molecular sciences, 25(8), 4296. https://doi.org/10.3390/ijms25084296
- Theis SR, Hashmi MF. Coombs Test. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547707/
- Berentsen, S., & Barcellini, W. (2021). Autoimmune Hemolytic Anemias. The New England journal of medicine, 385(15), 1407–1419. https://doi.org/10.1056/NEJMra2033982
- Costa, A., Mulas, O., Mereu, A. M., Schintu, M., Greco, M., & Caocci, G. (2025). Beneath the surface in autoimmune hemolytic anemia: pathogenetic networks, therapeutic advancements and open questions. Frontiers in immunology, 16, 1624667. https://doi.org/10.3389/fimmu.2025.1624667
- Chapuy, C. I., Nicholson, R. T., Aguad, M. D., Chapuy, B., Laubach, J. P., Richardson, P. G., Doshi, P., & Kaufman, R. M. (2015). Resolving the daratumumab interference with blood compatibility testing. Transfusion, 55(6 Pt 2), 1545–1554. https://doi.org/10.1111/trf.13069
- Fattizzo, B., & Motta, I. (2023). Rise of the planet of rare anemias: An update on emerging treatment strategies. Frontiers in medicine, 9, 1097426. https://doi.org/10.3389/fmed.2022.1097426
- Kumar Krishnegowda, V., Ramaswamy, V. V., Abiramalatha, T., Bandyopadhyay, T., S, A. K. P., & Kannan Loganathan, P. (2025). Direct antiglobulin test for the prediction of neonatal hyperbilirubinemia needing an intervention: a systematic review and diagnostic test accuracy meta-analysis. Frontiers in pediatrics, 12, 1475623. https://doi.org/10.3389/fped.2024.1475623