Key Takeaways
Ecchymoses are subcutaneous bleeding causing skin discoloration (bruise).
- Pathophysiology ▾: Small vessel damage leads to blood leakage into tissues; hemoglobin breakdown causes color changes.
- Causes ▾: Trauma, hematologic disorders, vascular issues, medications, nutritional deficiencies, infections, others.
- Symptoms ▾: Skin discoloration (evolving colors), pain, tenderness, swelling; systemic symptoms may indicate underlying issues.
- Treatment & Management ▾: Local measures (RICE), addressing underlying causes (medication changes, treating conditions), and recognizing when to seek medical help.
*Click ▾ for more information
Introduction
Ecchymoses are areas of skin discoloration, typically bluish-black or purplish, resulting from the leakage of blood into the subcutaneous tissue after small blood vessels rupture. They are commonly known as bruises.
Understanding ecchymoses is crucial because they can be a visible indicator of underlying medical conditions that might otherwise go unnoticed. While minor bruising from trauma is common, spontaneous, excessive, or unusual bruising patterns can signal serious issues such as bleeding disorders, blood dyscrasias, vascular abnormalities, medication side effects, nutritional deficiencies, or even non-accidental injury. Recognizing these patterns and knowing when to investigate further can lead to timely diagnosis and management of potentially life-threatening conditions.
Pathophysiology of Ecchymoses
The pathophysiology of ecchymoses begins with an insult, often a physical trauma, that causes damage to small subcutaneous blood vessels, primarily capillaries and venules. This damage disrupts the integrity of the vessel walls, leading to the extravasation, or leakage, of blood into the surrounding interstitial spaces within the dermis and subcutaneous tissue. The escaped erythrocytes release hemoglobin, which initially gives the bruise its characteristic red or bluish-black appearance. Over time, enzymatic degradation of hemoglobin occurs, leading to predictable color changes as the heme molecule is converted to bilirubin (yellowish) and then hemosiderin (brownish), reflecting the different stages of the body's natural resorption of the leaked blood. The size and depth of the ecchymosis depend on the extent of vascular injury and the amount of blood that escapes into the tissues.
Causes of Ecchymoses
Ecchymoses, or bruising, can arise from a wide spectrum of causes, broadly categorized as traumatic and non-traumatic.
Traumatic causes are the most common and occur when external forces impact the body, causing small blood vessels beneath the skin to rupture without breaking the skin itself. These can range from minor incidents like bumps, falls, and sports injuries to more significant trauma such as road traffic accidents or surgical procedures. The extent and severity of the bruising often correlate with the force of the impact and the vascularity of the affected area.
Non-traumatic causes encompass a more diverse set of underlying medical conditions and external factors that predispose individuals to bruising more easily or spontaneously.
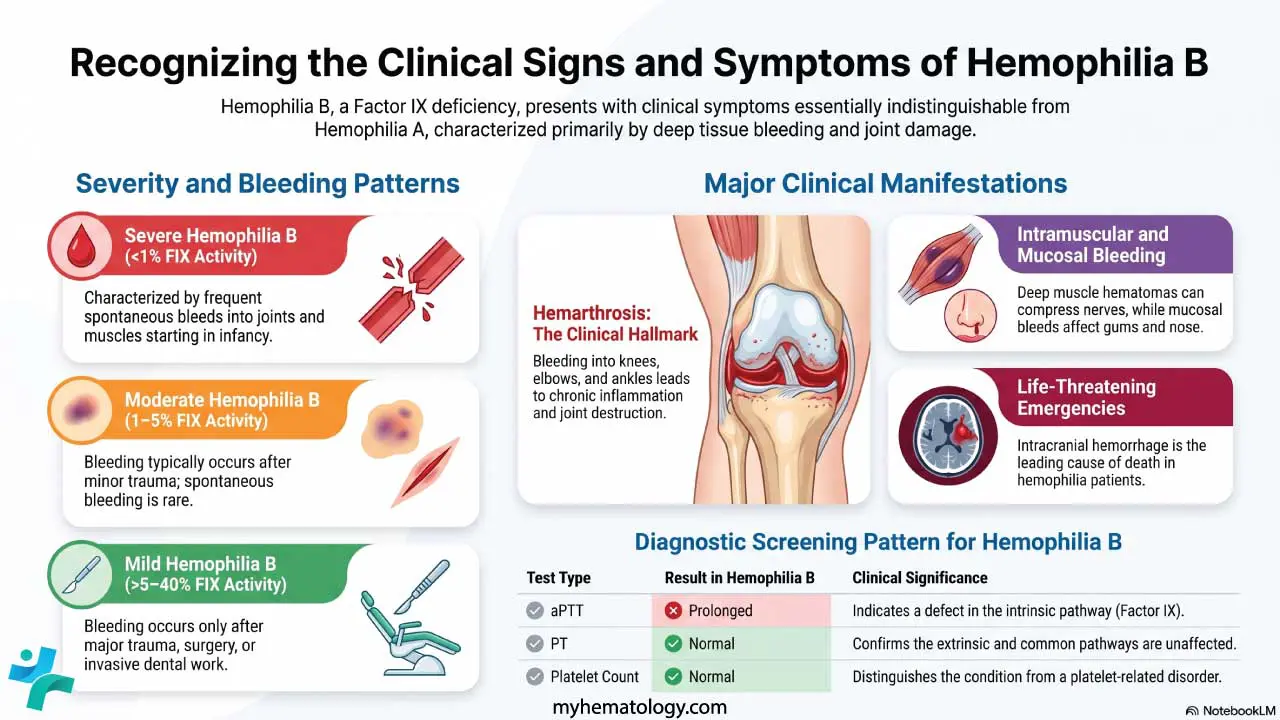
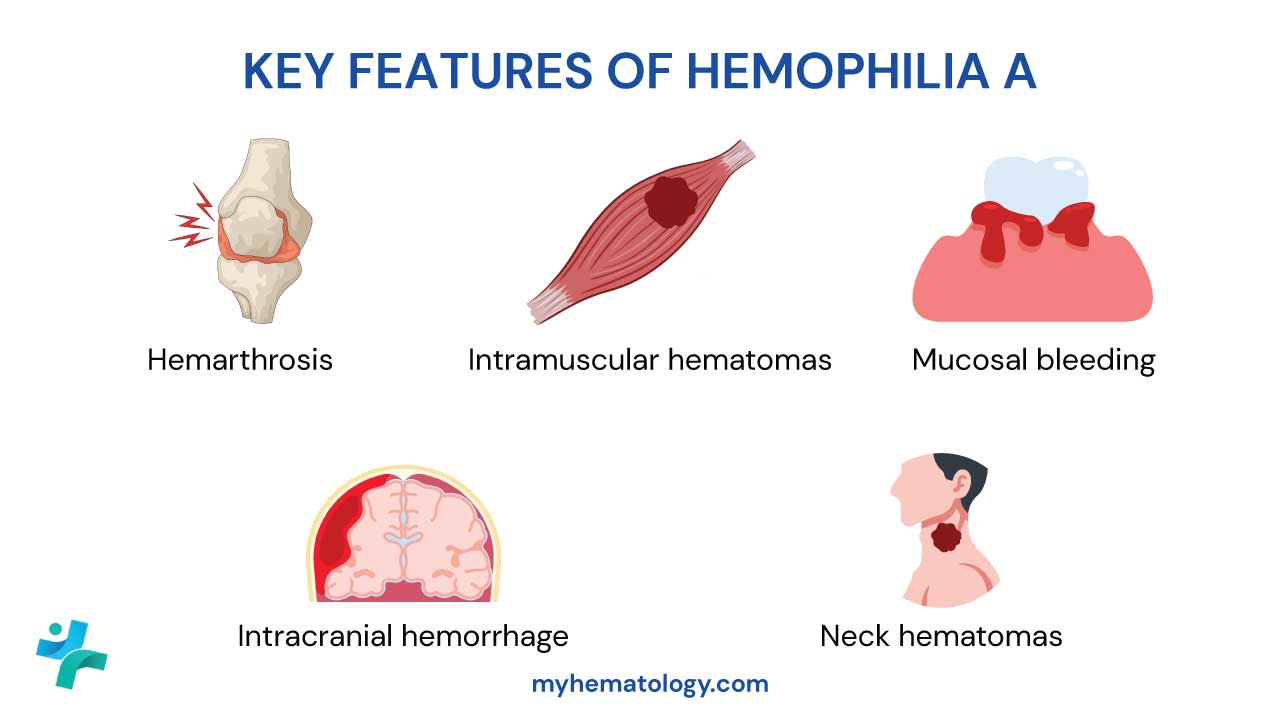
- Hematologic Disorders: Conditions affecting the blood's ability to clot properly are significant contributors. Thrombocytopenia, a low platelet count, reduces the number of cells responsible for forming blood clots. Platelet dysfunction refers to abnormalities in how platelets function, even if the count is normal. Coagulation factor deficiencies, such as Hemophilia A and B or von Willebrand disease, impair the cascade of proteins needed for effective clot formation. Hematological malignancies like leukemia can also lead to easy bruising due to bone marrow dysfunction and reduced platelet production.
- Vascular Disorders: Abnormalities in blood vessel structure or function can increase fragility. Vasculitis, inflammation of blood vessels, can lead to leakage and bruising. Connective tissue diseases like Ehlers-Danlos syndrome can cause fragile blood vessels and skin. Senile purpura is a common condition in older adults where the skin and blood vessels become more fragile, leading to easy bruising, often on the forearms and backs of the hands.
- Medications: Certain drugs can interfere with the body's clotting mechanisms. Anticoagulants like warfarin, heparin, and direct oral anticoagulants intentionally thin the blood and can increase the likelihood and extent of bruising even from minor trauma. Antiplatelet drugs such as aspirin and clopidogrel inhibit platelet function. Long-term use of corticosteroids can lead to thinning of the skin and blood vessel walls, making them more susceptible to damage.
- Nutritional Deficiencies: Certain vitamins play a crucial role in blood vessel integrity and coagulation. Vitamin C deficiency (Scurvy) can lead to fragile capillaries and widespread bruising. Vitamin K deficiency impairs the synthesis of several clotting factors.
- Infections: Severe infections, such as meningococcemia, can trigger disseminated intravascular coagulation (DIC), a condition characterized by widespread clotting followed by depletion of clotting factors, leading to both thrombosis and bleeding, including ecchymoses.
- Other Conditions: Liver disease can impair the liver's ability to produce clotting factors, leading to easy bruising. Amyloidosis, a condition where abnormal proteins deposit in tissues, can weaken blood vessel walls. Factitious bruising refers to self-inflicted bruising, which can be a sign of psychological issues.
Clinical Presentation and Symptoms

The primary sign of ecchymoses is the visible discoloration of the skin. This discoloration arises from the extravasated blood beneath the surface and undergoes a characteristic color progression over time as hemoglobin breaks down.
- Initially: The bruise often appears reddish or bluish-black, reflecting the presence of oxygenated and then deoxygenated blood.
- Within a few days: As hemoglobin is metabolized to biliverdin, the bruise may take on a bluish or purple hue.
- After about a week: The breakdown continues to bilirubin, causing the bruise to turn greenish.
- Over the following days to weeks: The bruise gradually fades to yellowish and then brownish as hemosiderin is formed, eventually disappearing as the blood is reabsorbed by the body.
Beyond the visual changes, ecchymoses can be associated with several symptoms, although these may vary depending on the size, location, and underlying cause of the bruising.
- Pain and Tenderness: Especially in the initial stages, the bruised area may be painful to the touch. The degree of pain can range from mild discomfort to significant tenderness, particularly if the bruising is extensive or involves deeper tissues.
- Swelling: Inflammation and the accumulation of blood can lead to localized swelling around the bruised area. This is more common with larger ecchymoses or those resulting from significant trauma.
- Warmth: The affected area might feel slightly warmer than the surrounding skin due to the inflammatory response.
- Limitations in Movement: If the ecchymosis is located near a joint or involves a large area, the associated pain and swelling can restrict movement in that part of the body.
- Palpable Mass (Hematoma): In some cases, especially with more significant bleeding, a collection of blood can form a palpable mass beneath the skin, known as a hematoma. While related to ecchymoses (both involve blood extravasation), hematomas are typically larger and more localized.
It's also crucial to consider associated systemic symptoms that might point towards an underlying cause beyond simple trauma. These "red flag" symptoms warrant further investigation.
- Easy or Spontaneous Bruising: Bruising that occurs without any identifiable injury or from minimal trauma.
- Frequent or Recurrent Bruising: Experiencing bruises regularly without a clear explanation.
- Bruising in Unusual Locations: Such as the trunk, back, or palms and soles (unless there's a clear history of trauma to these areas).
- Excessively Large Bruises: Bruises that are disproportionately large compared to the reported injury.
- Rapidly Expanding Bruises: Bruises that continue to grow in size after the initial injury.
- Bleeding from Other Sites: Such as nosebleeds (epistaxis), gum bleeding, heavy menstrual periods (menorrhagia), or blood in the urine or stool.
- Petechiae or Purpura: The presence of small, pinpoint red or purple spots (petechiae) or slightly larger purple spots (purpura) in addition to ecchymoses can suggest platelet or vascular issues.
- Fatigue, Weakness, or Pallor: These could indicate an underlying hematological disorder or anemia.
- Fever or Weight Loss: These systemic symptoms might suggest infection or malignancy.
- Joint Pain or Swelling: Could be associated with certain connective tissue diseases or vasculitis.
- Jaundice (Yellowing of the Skin and Eyes): May suggest liver disease, which can affect clotting factors.
- Family History of Bleeding Disorders: A personal or family history of easy bleeding or bruising is significant.
Therefore, while the visual appearance and local symptoms of ecchymoses are important, it's the context of how they arise and any accompanying systemic symptoms that often provide crucial clues to the underlying etiology.
Differential Diagnoses of Ecchymoses
| Condition | Key Features | Distinguishing from Ecchymoses | Potential Underlying Causes |
| Petechiae | Small, pinpoint hemorrhages (< 3 mm), red or purple spots. | Smaller size, often indicate capillary fragility or low platelets, may not show the same color progression. | Thrombocytopenia, vasculitis, infections, increased intravascular pressure. |
| Purpura (intermediate) | Hemorrhages 3 mm - 1 cm in size. | Smaller than typical ecchymoses, but underlying causes can overlap. | Platelet disorders, vasculitis, coagulation abnormalities. |
| Hematoma | Localized collection of blood, often larger, may form a palpable mass, swelling. | More localized, often associated with significant swelling and pain, may not be as superficial or spread out. | More significant trauma, bleeding disorders. |
| Telangiectasias | Small, widened blood vessels visible on the skin as fine lines or webs, red/purple. | Do not involve blood leakage into tissue, do not change color like bruises, appear as fixed vascular markings. | Rosacea, spider angiomas, hereditary hemorrhagic telangiectasia. |
| Cherry Angiomas | Small, benign, bright red to purplish papules. | Raised papules, bright red color, do not represent bleeding into the skin, do not change color over time. | Benign vascular proliferation. |
| Venous Lakes | Small, dark blue or purple, compressible papules, often on lips/ears (elderly). | Dark blue/purple color, compressible, represent dilated venules, not blood extravasation. | Dilated venules, common in older adults. |
| Mongolian Spots | Bluish-gray birthmarks, typically on lower back/buttocks of infants. | Present at birth, characteristic bluish-gray color, do not follow the color progression of bruises, fade over time. | Presence of melanocytes deep in the dermis. |
| Hyperpigmentation | Increased skin pigmentation, various colors (brown, tan, etc.). | Lack the initial red/blue/black color of a fresh bruise and the subsequent color changes, no associated pain or swelling. | Post-inflammatory hyperpigmentation, melasma, drug reactions. |
| Vasculitic Rashes | Purpuric or ecchymotic-like lesions often with papules, nodules, ulcerations. | Often have other types of lesions present, may be associated with systemic symptoms. | Inflammation of blood vessels (vasculitis). |
| Drug Eruptions (purpuric) | Purpuric or ecchymotic-like lesions as part of a broader rash. | Occur in the context of a drug reaction, often with other rash elements, distribution may be suggestive. | Adverse reaction to certain medications. |
| Non-Accidental Injury (NAI) | Bruises in unusual locations, patterns, inconsistent with history. | Location, pattern, and history are inconsistent with accidental trauma, may have other injuries present. | Physical abuse. |
| Factitious Bruising | Bruises in unusual patterns or easily accessible locations, lack of credible history. | Pattern and location may be self-inflicted, inconsistent history of trauma. | Psychological disorders. |
| Ehlers-Danlos Syndrome | Easy bruising along with joint hypermobility and skin hyperextensibility. | Presence of other characteristic features of the connective tissue disorder. | Inherited defects in collagen synthesis. |
Treatment and Management of Ecchymoses
Local Measures for Traumatic Ecchymoses
RICE Therapy (for the initial 24-48 hours)
- Rest: Avoid using the injured area as much as possible to prevent further bleeding and tissue damage.
- Ice: Apply ice packs wrapped in a cloth to the bruised area for 15-20 minutes at a time, several times a day. Cold constricts blood vessels, which can help reduce swelling and limit the extent of bleeding into the tissues, thus minimizing the size and severity of the bruise.
- Compression: If the bruise is on a limb, applying a gentle elastic bandage can help reduce swelling. Ensure the bandage is not too tight to avoid restricting blood flow.
- Elevation: Elevating the injured limb above the level of the heart can help drain excess fluid and reduce swelling.
Pain Management
- Acetaminophen (Paracetamol): Can be used to relieve mild to moderate pain associated with bruising.
- Avoid Non-Steroidal Anti-inflammatory Drugs (NSAIDs): Medications like ibuprofen and naproxen can inhibit platelet function and potentially worsen bleeding, so they are generally not recommended, especially in individuals with known bleeding disorders or those taking anticoagulants.
Warm Compresses (after 48 hours)
After the initial 24-48 hours, applying warm compresses to the bruised area several times a day can help increase blood flow and promote the reabsorption of the pooled blood, thus speeding up the healing process and the resolution of the discoloration.
Management of Underlying Causes
The definitive treatment for ecchymoses hinges on identifying and addressing the root cause.
- Discontinuation or Adjustment of Medications: If medications like anticoagulants or antiplatelet drugs are contributing to easy bruising, the prescribing physician may need to adjust the dosage or consider alternative medications, balancing the risk of bleeding with the therapeutic benefit of the drug. Corticosteroid use may also need to be reviewed.
- Treatment of Infections: If an infection is the underlying cause (e.g., meningococcemia leading to DIC), prompt and aggressive treatment with antibiotics and supportive care is crucial.
- Management of Hematological Disorders
- Thrombocytopenia: Treatment may involve addressing the underlying cause (e.g., treating leukemia, stopping causative medications), platelet transfusions in severe cases, or medications to increase platelet production (e.g., corticosteroids, thrombopoietin receptor agonists).
- Coagulation Factor Deficiencies (e.g., Hemophilia): Management involves replacement therapy with the deficient clotting factor, either on demand for bleeding episodes or prophylactically to prevent bleeding.
- Von Willebrand Disease: Treatment can include desmopressin (DDAVP) to release stored vWF, vWF-containing blood products, or antifibrinolytic agents.
- Addressing Nutritional Deficiencies: Supplementation with the deficient vitamin (e.g., Vitamin C for scurvy, Vitamin K if deficient) is essential. Dietary changes may also be recommended.
- Management of Vascular Disorders: Treatment depends on the specific condition. Vasculitis may require immunosuppressive medications. Connective tissue disorders are managed based on their specific manifestations.
- Liver Disease Management: Addressing the underlying liver dysfunction is crucial. This may involve lifestyle changes, medications, or in severe cases, liver transplantation.
- Psychological Support for Factitious Bruising: Individuals with factitious bruising may benefit from psychological evaluation and therapy.
- Intervention in Non-Accidental Injury (NAI): Suspected cases of child abuse require immediate reporting to child protective services and a comprehensive evaluation to ensure the safety and well-being of the child.
The treatment and management of ecchymoses primarily focus on alleviating symptoms and addressing any underlying causes. For simple bruises resulting from minor trauma, the approach is usually conservative and aimed at promoting healing. However, when ecchymoses are extensive, recurrent, or suggestive of an underlying medical condition, a more comprehensive evaluation and targeted treatment are necessary.
Frequently Asked Questions (FAQs)
What is the difference between ecchymosis and purpura?
Ecchymosis and purpura are both caused by blood leaking from small blood vessels into the skin, resulting in discoloration, but they differ primarily in size: purpura are defined as purple or red spots ranging from 3 to 10 millimeters in diameter, while ecchymoses are larger, flat bruises with a diameter greater than 1 centimeter. Purpura can sometimes appear more like a rash of spots, whereas ecchymoses tend to be larger, more diffuse areas of discoloration often associated with trauma, though both can be signs of underlying medical conditions affecting platelets, blood vessels, or coagulation.
What deficiency causes ecchymosis?
Deficiencies in Vitamin K and Vitamin C are the most directly linked to causing ecchymoses due to their roles in blood clotting and blood vessel integrity, respectively. Vitamin K is essential for the synthesis of several clotting factors, and a deficiency can lead to impaired coagulation and increased bleeding, resulting in ecchymoses. Vitamin C is crucial for the production of collagen, a protein that provides structural support to blood vessels; a deficiency weakens these vessels, making them fragile and prone to rupture, leading to bruising. While less common, deficiencies in other nutrients like Vitamin B12 have also been rarely associated with ecchymoses, possibly due to effects on platelet function or blood cell production.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Gaurav V, Pandhi D, Kotru M. Ecchymosis: A Subtle Sign Unmasking Malignancy. Indian Dermatol Online J. 2022 Mar 3;13(2):262-265. doi: 10.4103/idoj.idoj_388_21. PMID: 35287413; PMCID: PMC8917491.
- Hernandez-Amaris MF, Victoria-Chaparro J. Spontaneous ecchymoses in a young woman leading to the diagnosis of hypermobile Ehlers-Danlos syndrome. Actas Dermosifiliogr. 2022 Jul-Aug;113(7):719-720. English, Spanish. doi: 10.1016/j.ad.2020.08.032. Epub 2021 Dec 31. PMID: 35282858.
- Asirdizer M, Besik EZ, Kartal E. Non-traumatic ecchymoses: A literature review from a medico-legal perspective. J Forensic Leg Med. 2023 Apr;95:102490. doi: 10.1016/j.jflm.2023.102490. Epub 2023 Feb 3. PMID: 36758310.