Key Takeaways
Follicular Lymphoma is a type of slow-growing, non-Hodgkin lymphoma affecting B-cells.
Key Features
- Indolent Course: Often progresses slowly.
- Lymph Node Involvement: Commonly affects lymph nodes, especially in the neck, armpits, or groin.
- Histological Features: Characterized by a follicular growth pattern.
- Genetic Alterations: The t(14;18) translocation is a common genetic abnormality.
Symptoms ▾
- Swollen lymph nodes
- Fatigue
- Weight loss
- Night sweats
- Fever
Diagnosis ▾
- Blood tests
- Bone marrow biopsy
- Lymph node biopsy
- Imaging studies
Treatment ▾
- Watchful waiting
- Chemotherapy
- Immunotherapy
- Targeted therapy
- Radiotherapy
Prognosis
- Generally favorable, especially for early-stage disease.
- Treatment advancements have improved outcomes.
*Click ▾ for more information
Introduction
Follicular lymphoma is a type of slow-growing cancer that affects white blood cells called lymphocytes. It develops when these cells grow out of control and cluster together to form lumps in the lymph glands or other organs. Follicular lymphoma is one of the most common types of non-Hodgkin lymphoma.
Brief Overview of Lymphomas
Lymphomas are a group of cancers that originate in the lymphatic system, a network of vessels and glands that helps fight infection. They arise from lymphocytes, a type of white blood cell. There are two main types of lymphoma:
- Hodgkin lymphoma: Characterized by the presence of a specific type of cell called the Reed-Sternberg cell.
- Non-Hodgkin lymphoma (NHL): A more diverse group of cancers, including follicular lymphoma.
Follicular Lymphoma Classification and Grading
Classification According to the World Health Organization (WHO)
| Subtype | Definition | Characteristics |
| Classic Follicular Lymphoma | The most common type of FL. | Characterized by a follicular growth pattern with a mixture of centrocytes and centroblasts. |
| Predominantly Diffuse Follicular Lymphoma | A less common variant. | Primarily consists of centrocytes with few or no centroblasts, leading to a more diffuse growth pattern. |
| Follicular Lymphoma with Unusual Cytological Features | A rare subtype. | Exhibits unique cytological features that differentiate it from classic FL, often with larger cells and a more aggressive behavior. |
| Follicular Large B-cell Lymphoma (FLBCL) | A more aggressive form of FL. | Characterized by a diffuse growth pattern with large B-cell morphology. |
| In Situ Follicular B-cell Neoplasm | An early stage of FL. | Neoplastic B cells are confined to the germinal centers of lymph follicles. |
| Paediatric-Type Follicular Lymphoma | A rare variant primarily affecting children and young adults. | Often presents with a more aggressive clinical course and may exhibit features of anaplastic large cell lymphoma. |
| Duodenal-type Follicular Lymphoma | A rare extranodal form of FL. | Primarily affects the duodenum and can present with gastrointestinal symptoms. |
| Primary Cutaneous Follicle Center Lymphoma | A rare type of non-Hodgkin lymphoma. | Primarily affects the skin and presents as skin nodules or plaques. |
Grading of Follicular Lymphoma
Follicular lymphoma is graded based on the number of centroblasts present in the tissue sample. This grading system helps predict the aggressiveness of the disease and guides treatment decisions:
- Grade 1 and 2: Low-grade FL, characterized by a slow growth rate and a more indolent course.
- Grade 3: High-grade FL, associated with a more aggressive clinical behavior and a higher risk of transformation to a more aggressive lymphoma, such as diffuse large B-cell lymphoma.
Distinction Between Indolent and Aggressive Lymphomas
- Indolent Lymphomas: These lymphomas, like low-grade follicular lymphoma, tend to grow slowly and may not require immediate treatment. They can remain stable for many years.
- Aggressive Lymphomas: These lymphomas, such as high-grade follicular lymphoma or diffuse large B-cell lymphoma, grow rapidly and can spread quickly to other parts of the body. They often require more aggressive treatment.
It’s important to note that while follicular lymphoma is generally considered an indolent lymphoma, it can transform into a more aggressive form over time. Regular monitoring and timely intervention are crucial for managing this disease.
Pathogenesis of Follicular Lymphoma
The pathogenesis of follicular lymphoma (FL) is a complex process involving multiple genetic and epigenetic alterations that lead to the malignant transformation of B lymphocytes.
Key Genetic Alteration
- t(14;18) translocation: This is the most common genetic abnormality found in FL. It results in the overexpression of the BCL-2 gene, which encodes an anti-apoptotic protein. This overexpression prevents cell death, allowing the malignant cells to accumulate and proliferate.
Role of the Microenvironment
The microenvironment within lymph nodes plays a crucial role in the growth and survival of FL cells. Follicular dendritic cells (FDCs) and T follicular helper (TFH) cells provide essential growth factors and survival signals to FL cells.
Stages of Follicular Lymphoma Development
- Early Stage: A B cell acquires the t(14;18) translocation and other genetic alterations.
- Premalignant Stage: The cell undergoes clonal expansion and accumulates additional genetic and epigenetic changes.
- Malignant Transformation: The cell becomes fully transformed and begins to proliferate uncontrollably.
Follicular Lymphoma Symptoms
Follicular lymphoma is often an indolent disease, meaning it can progress slowly and may not cause noticeable symptoms for many years. However, when symptoms do appear, they may include:
Common Symptoms
- Swollen Lymph Nodes: Painless swelling of lymph nodes, especially in the neck, armpits, or groin.
- Fatigue: Persistent tiredness and lack of energy.
- Weight Loss: Unexplained weight loss, often significant.
- Night Sweats: Excessive sweating, particularly at night.
- Fever: Low-grade fever that may occur intermittently.
Less Common Symptoms
- Shortness of Breath: Difficulty breathing, especially with exertion.
- Abdominal Pain or Swelling: Due to enlargement of lymph nodes in the abdomen.
- Bone Pain: Pain in the bones, especially in the back or chest.
- Itchy Skin: Skin irritation or rash.
It’s important to note that many people with follicular lymphoma may not experience any symptoms at all. In such cases, the disease may be detected during a routine physical exam or blood test.
Laboratory Investigations for Follicular Lymphoma
Laboratory investigations play a crucial role in diagnosing and staging follicular lymphoma.
Complete Blood Count (CBC) with Differential
- Function: To analyze the different blood cells and types of white blood cells.
- Expected Results: May show anemia, thrombocytopenia, or an increased white blood cell count, especially lymphocytes.
Bone Marrow Biopsy and Aspiration
- Function: To examine the bone marrow for evidence of lymphoma cells.
- Expected Results: May show infiltration of the bone marrow by lymphoma cells.
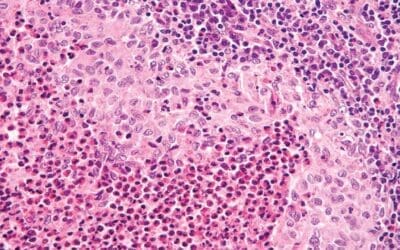
Lymph Node Biopsy
- Function: To obtain a tissue sample from a swollen lymph node for microscopic examination.
- Expected Results: May show a characteristic follicular pattern with a mixture of centrocytes and centroblasts.
Immunohistochemistry
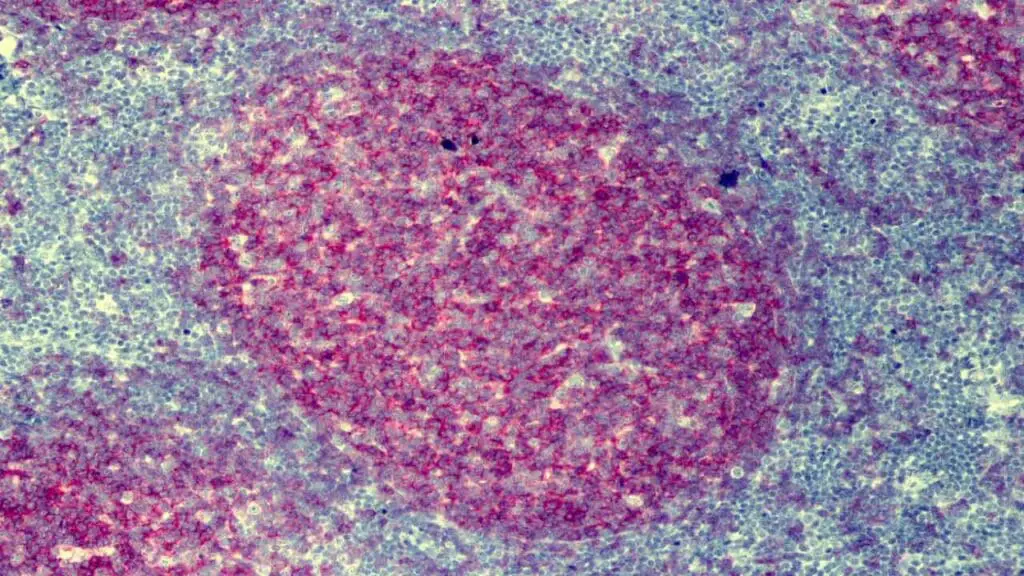
- Function: To identify specific proteins on the surface of lymphoma cells.
- Expected Results: May show positive staining for markers like CD20, CD10, BCL-2, and BCL-6.
Flow Cytometry
- Function: To analyze the expression of specific proteins on the surface of lymphoma cells.
- Expected Results: May show abnormal expression of B-cell markers.
Molecular Testing
- Function: To detect genetic abnormalities, such as the t(14;18) translocation.
- Expected Results: May identify the presence of the t(14;18) translocation or other genetic alterations related to follicular lymphoma.
Staging of Follicular Lymphoma
Staging is a process used to determine the extent of the disease. The most commonly used staging system for lymphoma is the Ann Arbor staging system, which is modified by the Lugano classification. This system categorizes lymphoma into stages based on the number of lymph node regions involved, the presence of extranodal involvement, and the presence of systemic symptoms:
- Stage I: Involvement of a single lymph node region or a single extranodal site.
- Stage II: Involvement of two or more lymph node regions on the same side of the diaphragm or localized extranodal involvement.
- Stage III: Involvement of lymph node regions on both sides of the diaphragm.
- Stage IV: Disseminated disease with involvement of one or more extranodal sites.
The Lugano classification is a more recent staging system that provides additional prognostic information. It incorporates factors such as the International Prognostic Index (IPI) score and the presence of bulky disease. The IPI considers factors such as age, performance status, lactate dehydrogenase level, number of extranodal sites, and stage of disease.
Understanding the stage of the disease helps determine the appropriate treatment plan and predict the prognosis.
Treatment and Management of Follicular Lymphoma
The treatment approach for follicular lymphoma (FL) depends on various factors, including the stage of the disease, the patient’s overall health, and their individual preferences. While there’s no cure for FL, treatment aims to control the disease, alleviate symptoms, and improve quality of life.
Treatment Options
Watchful Waiting
For early-stage, asymptomatic disease, a “watch and wait” approach may be adopted. Regular monitoring through physical exams, blood tests, and imaging studies is essential to detect any disease progression.
Combination Chemotherapy
This involves using multiple drugs to target cancer cells. Common regimens include R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and R-CVP (rituximab, cyclophosphamide, vincristine, and prednisone).
Immunotherapy
Monoclonal antibodies: These drugs target specific proteins on cancer cells, helping the immune system to destroy them. Rituximab is a commonly used monoclonal antibody.
CAR-T cell therapy: This advanced therapy involves modifying a patient’s own T cells to target and kill cancer cells.
Other Immunotherapy Agents: Newer immunotherapy drugs, such as polatuzumab vedotin and obinutuzumab, are being used in combination with other therapies.
Targeted Therapy
Ibrutinib: A targeted therapy that inhibits the Bruton’s tyrosine kinase (BTK) enzyme, which is crucial for B-cell signaling.
Venetoclax: A targeted therapy that inhibits BCL-2, a protein that prevents cell death.
Stem Cell Transplant
Considered for patients with aggressive disease or those who have not responded to other treatments. It involves high-dose chemotherapy followed by a stem cell transplant to restore bone marrow function.
Treatment Strategies
- First-line therapy: For advanced-stage disease, initial treatment often involves a combination of chemotherapy and immunotherapy.
- Relapsed/Refractory disease: For patients whose disease returns or does not respond to initial treatment, various salvage therapies may be considered, including different chemotherapy regimens, targeted therapies, and immunotherapy.
- Maintenance therapy: After initial treatment, maintenance therapy with rituximab may be used to prolong remission.
Supportive Care
In addition to specific treatments, supportive care is essential to manage side effects and improve quality of life. This may include:
- Pain Management: To alleviate pain associated with lymph node enlargement or bone involvement.
- Fatigue Management: To address fatigue, which is a common symptom of FL.
- Nutritional Support: To maintain adequate nutrition and prevent weight loss.
- Psychological Support: To help patients cope with the emotional and psychological impact of the diagnosis.
The optimal treatment approach for a specific patient should be determined by a healthcare team, including a hematologist-oncologist. Regular follow-up care is crucial to monitor the disease and adjust treatment as needed.
Frequently Asked Questions (FAQs)
How serious is follicular lymphoma?
Follicular lymphoma is generally considered a serious condition, but it’s important to remember that it’s often slow-growing and manageable.
While it’s not typically curable, with advancements in treatment, many people can live with it for many years. The severity can vary depending on factors like the stage of the disease, the patient’s overall health, and their response to treatment.
How long do people live with follicular lymphoma?
The prognosis for follicular lymphoma has significantly improved in recent years, thanks to advancements in treatment. While it’s not typically curable, it’s often considered a chronic, manageable condition. Overall, the 5-year survival rate for follicular lymphoma is quite high, often exceeding 90%. However, it’s important to note that individual outcomes can vary.
Is stage 4 follicular lymphoma terminal?
No, stage 4 follicular lymphoma is not necessarily terminal. While it’s a more advanced stage, with advancements in treatment, many people with stage 4 follicular lymphoma can live for many years.
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. WHO Classification of Tumours, Revised 4th Edition, Volume 2. 2017.
- Adler EM. Living with Lymphoma: A Patient’s Guide (Johns Hopkins Press Health Books (Paperback)). 2016.
- Leukemia & Lymphoma Society (LLS)
- Freedman A, Jacobsen E. Follicular lymphoma: 2020 update on diagnosis and management. Am J Hematol. 2020 Mar;95(3):316-327. doi: 10.1002/ajh.25696. Epub 2019 Dec 22. PMID: 31814159.
- Flowers CR, Matasar MJ, Herrera AF, Hertzberg M, Assouline S, Demeter J, McMillan A, Mehta A, Opat S, Trnňný M, Musick L, Hirata J, Yang A, Sehn LH. Polatuzumab vedotin plus bendamustine and rituximab or obinutuzumab in relapsed/refractory follicular lymphoma: a phase Ib/II study. Haematologica. 2024 Apr 1;109(4):1194-1205. doi: 10.3324/haematol.2023.283557. PMID: 37767550; PMCID: PMC10985435.
- Nastoupil LJ, Hess G, Pavlovsky MA, Danielewicz I, Freeman J, García-Sancho AM, Glazunova V, Grigg A, Hou JZ, Janssens A, Kim SJ, Masliak Z, McKay P, Merli F, Munakata W, Nagai H, Özcan M, Preis M, Wang T, Rowe M, Tamegnon M, Qin R, Henninger T, Curtis M, Caces DB, Thieblemont C, Salles G. Phase 3 SELENE study: ibrutinib plus BR/R-CHOP in previously treated patients with follicular or marginal zone lymphoma. Blood Adv. 2023 Nov 28;7(22):7141-7150. doi: 10.1182/bloodadvances.2023010298. PMID: 37722354; PMCID: PMC10709678.