Key Takeaways
Vitamin K deficiency bleeding (VKDB) is a preventable disorder in newborns and infants caused by low active levels of clotting factors II, VII, IX, and X.
- Causes: All newborns are physiologically vitamin K deficient at birth because of poor placental transfer, low liver stores, a sterile gut, and low vitamin K in breast milk.
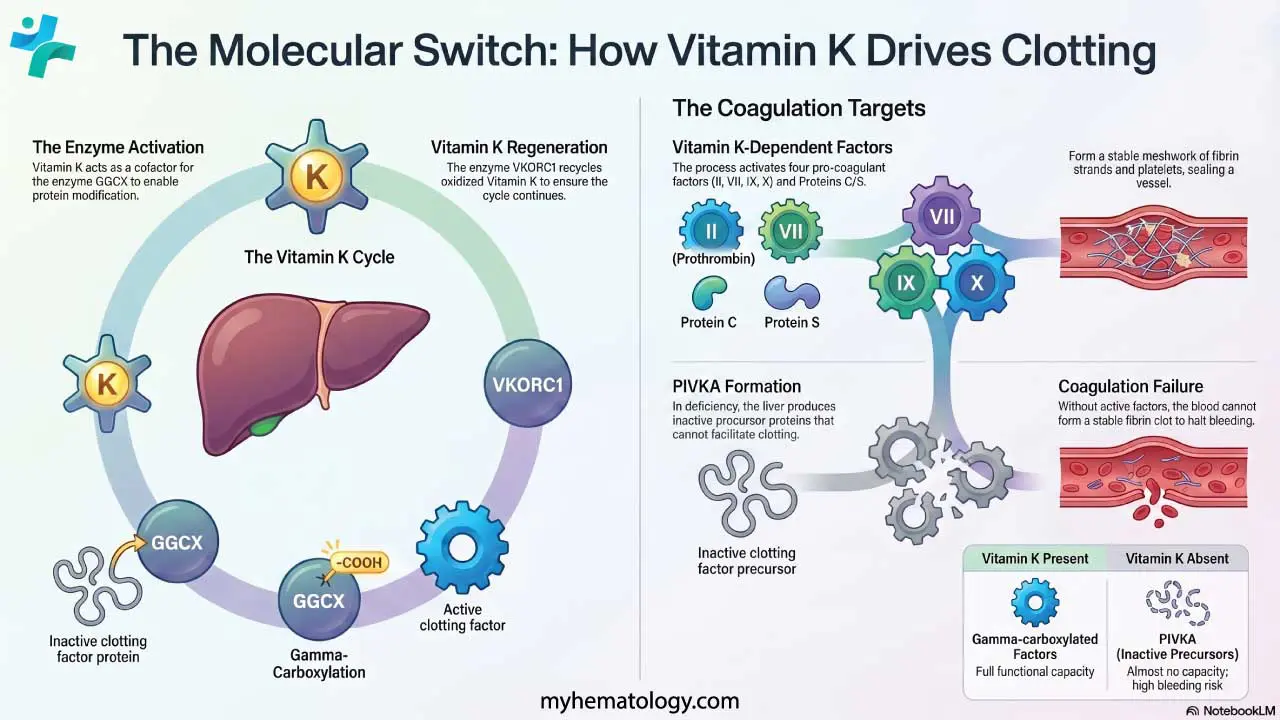
- Pathophysiology: Vitamin K is essential for the enzyme γ-glutamyl carboxylase (GGCX), which activates the clotting factors through γ-carboxylation. In deficiency, the liver produces inactive precursor factors called PIVKA (Proteins Induced by Vitamin K Absence or Antagonism), leading to coagulation failure.
- Types ▾: Late VKDB is the most dangerous form, with intracranial hemorrhage in about half to two-thirds of cases and a mortality rate near 1 in 5 untreated infants [1,7].
- Diagnosis ▾: The diagnostic hallmark is a markedly prolonged PT/INR with normal platelets, fibrinogen, and D-dimer, and elevated PIVKA-II.
- Treatment and Prevention ▾: A single intramuscular dose of vitamin K1 at birth, recommended by the AAP since 1961, prevents nearly all cases and is the global standard of care [3,4].
*Click ▾ for more information
Vitamin K deficiency in newborns is one of the most preventable causes of catastrophic bleeding in infancy. It is also one of the most misunderstood. This guide walks through what vitamin K deficiency bleeding (VKDB) is, why every newborn is at risk, how doctors diagnose and treat it, and why the simple injection given at birth saves lives.
Why This Topic Still Matters
Since 1961, a single intramuscular dose of vitamin K at birth has nearly eliminated VKDB in countries that practice routine prophylaxis. But the disease is making a quiet comeback. Recent U.S. data show a nationwide drop in vitamin K administration since 2018, driven largely by parental refusal [4]. Refusal rates remain low in hospitals (under 3%), but climb to 14% at home births and over 30% in some birthing centers [5]. Babies who do not receive the shot are 81 times more likely to develop Late VKDB, a form that often causes bleeding in the brain [5,7]. Understanding this disease is therefore both a clinical and a public health priority.
What Is Vitamin K Deficiency Bleeding?
VKDB is a bleeding disorder in young infants caused by low levels of active vitamin K-dependent clotting factors. It was once called Hemorrhagic Disease of the Newborn (HDN). The name was updated for two reasons. First, "vitamin K deficiency" makes the cause clear. Second, "newborn" was misleading, since the most dangerous form of the disease can occur up to six months after birth, well past the strict newborn period [1,3].
The condition affects four pro-coagulant clotting factors (II, VII, IX, and X) and two anticoagulant proteins (C and S). Without enough active vitamin K, the liver cannot finish making these factors work, and the blood cannot form a stable clot.
Why Every Newborn Is at Risk
Every newborn enters the world in a state of mild vitamin K deficiency. This is normal biology, not a disease, but it is enough to cause bleeding if left unsupported. Three factors are responsible:
- Vitamin K does not cross the placenta well, so the fetus is born with low stores.
- The newborn liver is immature and stores only small amounts of the vitamin.
- The newborn gut is sterile at birth, so the bacteria that make vitamin K2 (menaquinone) in older children and adults are not yet present.
Breast milk also contains very little vitamin K compared with formula. Exclusively breastfed infants who do not receive prophylaxis are therefore at the highest sustained risk, particularly for Late VKDB [1,7].
How Vitamin K Drives Clotting
Vitamin K is a fat-soluble vitamin with two clinically important forms. Phylloquinone (K1) comes from leafy green vegetables and is the form used for prophylaxis. Menaquinones (K2) are made by gut bacteria.
Inside the liver, vitamin K acts as a cofactor for an enzyme called gamma-glutamyl carboxylase (GGCX). GGCX adds a carboxyl group to the precursor forms of clotting factors II, VII, IX, and X, plus proteins C and S. This step, called gamma-carboxylation, is what switches these proteins from inactive to active.
During this reaction, vitamin K is converted to its oxidized form (vitamin K epoxide). Another enzyme, vitamin K epoxide reductase (VKORC1), then regenerates the active vitamin. Warfarin works by blocking VKORC1, which is why it acts as an anticoagulant.
When vitamin K is missing, the liver still makes the precursor proteins but cannot activate them. These inactive proteins build up and are called PIVKA (Proteins Induced by Vitamin K Absence or Antagonism). The most measured form is PIVKA-II, the inactive precursor of factor II [1].
The result: clotting factor levels look "normal" by mass, but the body has almost no functional clotting capacity. Bleeding follows.
Causes of VKDB
The universal physiological vulnerability described above explains why all newborns need protection. Specific situations raise the risk further:
- Maternal medications during pregnancy. Anticonvulsants (such as phenytoin and phenobarbital), antitubercular drugs (isoniazid, rifampin), warfarin, and certain cephalosporins can interfere with vitamin K metabolism in the fetus.
- Exclusive breastfeeding without prophylaxis. Breast milk is low in vitamin K.
- Underlying malabsorption. Cholestasis, cystic fibrosis, alpha-1-antitrypsin deficiency, and other conditions that impair fat absorption reduce vitamin K uptake.
- Failure to receive prophylaxis at birth. This is the single biggest modifiable risk factor [5,7].
Three Forms of VKDB
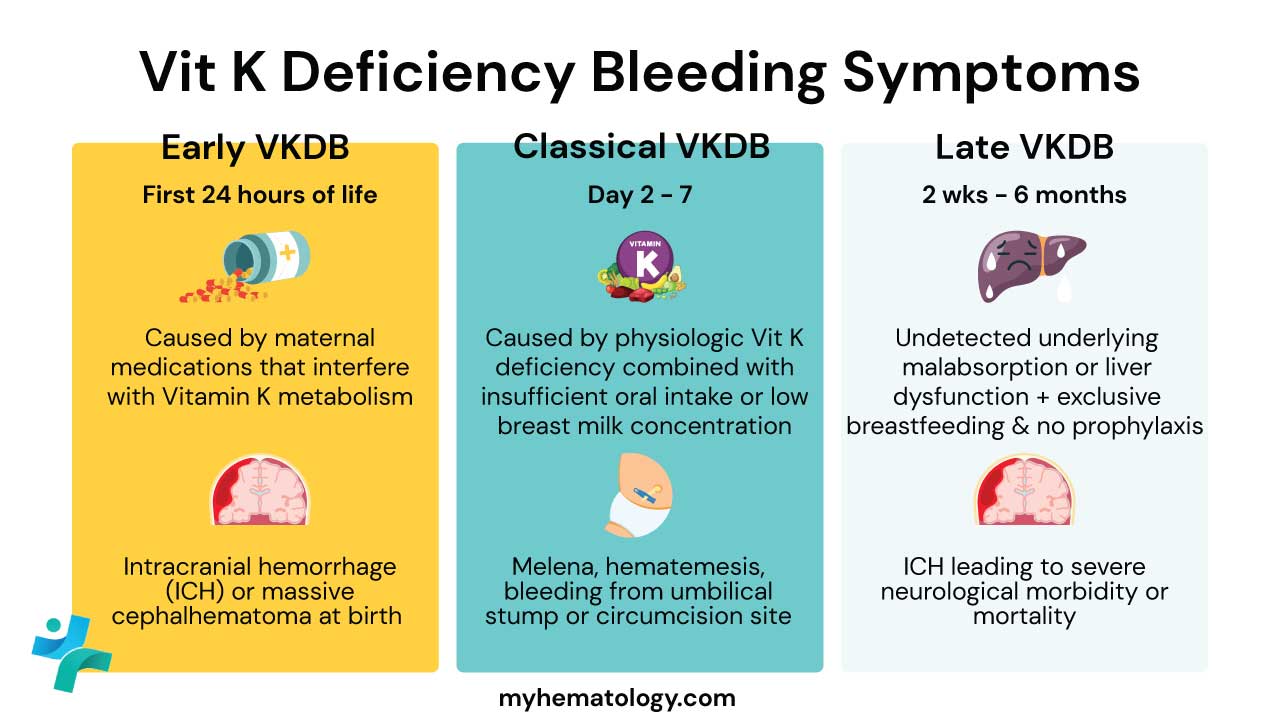
Without prophylaxis, early and classical VKDB occur in roughly 1 in 60 to 1 in 250 newborns. Late VKDB occurs in 1 in 14,000 to 1 in 25,000 unprophylaxed infants [7].
Laboratory Investigations and Diagnosis
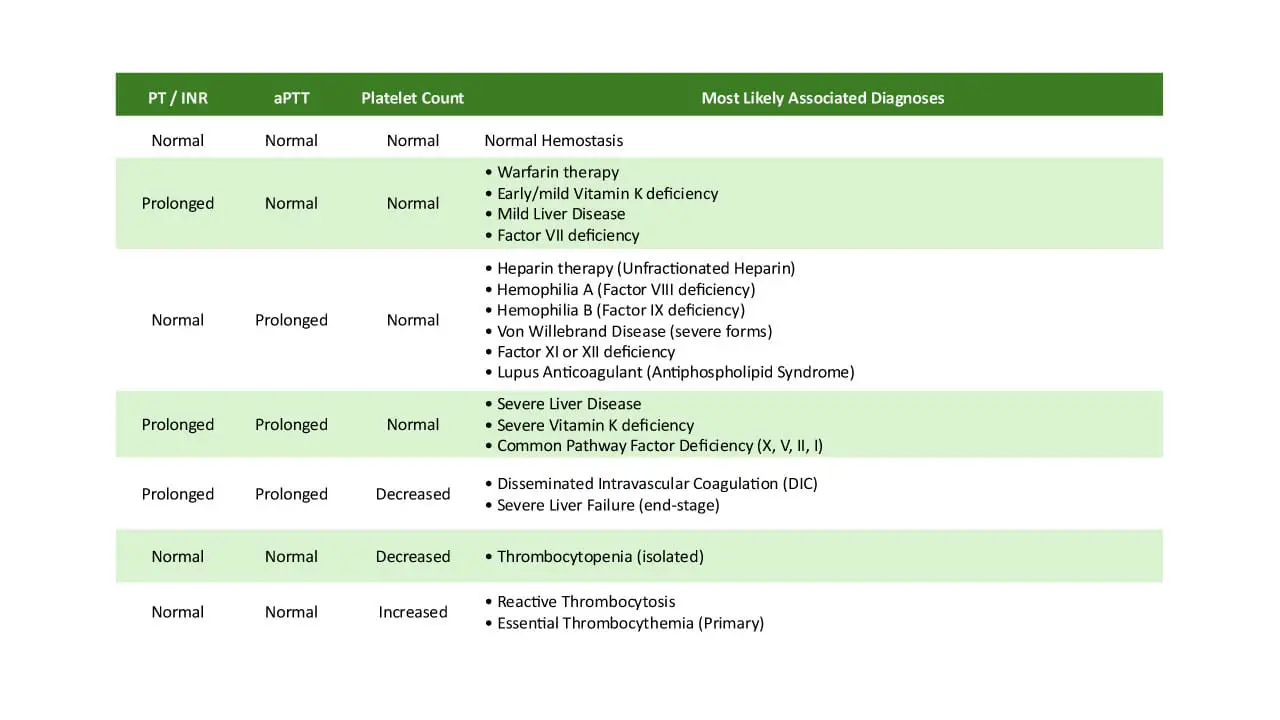
Diagnosis is clinical, supported by coagulation tests, and often confirmed by the dramatic response to vitamin K. The classic laboratory pattern is:
- Prothrombin time (PT) and INR: Severely prolonged. Factor VII has the shortest half-life of the vitamin K-dependent factors and falls first, which is why PT/INR rise so sharply.
- Activated partial thromboplastin time (aPTT): Prolonged or normal. Factor IX is also vitamin K-dependent, but the PT/INR change dominates.
- Platelet count, fibrinogen, and D-dimer: Normal. This pattern is critical for ruling out disseminated intravascular coagulation (DIC), which causes low platelets, low fibrinogen, and high D-dimer.
- PIVKA-II: While highly sensitive and specific for vitamin K deficiency, PIVKA-II assays are not universally available in acute settings and may take days to result. In an emergency, acute diagnosis relies almost entirely on the triad of clinical bleeding, severely prolonged PT/INR, and a normal platelet count [10].
- Cranial imaging: While a CT or MRI is ultimately mandatory to definitively map suspected Late VKDB, a Point-of-Care Cranial Ultrasound (CUS) is often the first-line imaging modality. Because infants have an open anterior fontanelle, CUS can rapidly detect major intracranial bleeds at the bedside, sparing the unstable infant from immediate radiation exposure and transport [11].
| Condition | PT / INR | aPTT | Platelets | Fibrinogen | PIVKA-II | Key Distinguishing Feature | |
|---|---|---|---|---|---|---|---|
|
VKDB
PRIMARY DX
|
↑↑ | ↑ or Normal | Normal | Normal | ↑↑↑ | Rapid and complete correction of PT/INR after Vitamin K administration. | |
|
DIC
CRITICAL
|
↑↑ | ↑↑ | ↓ | ↓ | Normal | High D-dimer, factor consumption. | |
|
Severe Hepatic Failure
MODERATE
|
↑ | ↑ | Normal or ↓ | ↓ | ↑ | High AST/ALT; poor response to vitamin K. | |
|
ISOLATED
|
Normal | ↑↑ | Normal | Normal | Normal | Isolated aPTT prolongation. | |
|
PLATELET
|
Normal | Normal | ↓↓ | Normal | Normal | Bleeding from low platelets only. |
Treatment: Stopping the Bleed
Acute management of vitamin K deficiency in a bleeding infant is a two-step strategy: replace the vitamin and, if needed, replace the factors.
Step 1: Give vitamin K1 immediately. A 1.0 mg dose is given intravenously in actively bleeding or critically ill infants. Higher doses (up to 5–10 mg) may be used in severe hemorrhage.
Important Note
Intravenous vitamin K must be administered slowly; rapid IV push carries a black-box warning for a rare but severe risk of anaphylactoid reactions, including shock or cardiac arrest [12].
Step 2: Replace clotting factors if bleeding is severe. Vitamin K alone cannot stop active bleeding fast enough. Current pediatric hematology guidelines recommend 4-factor Prothrombin Complex Concentrate (PCC) as the first-line therapy for life-threatening hemorrhage, such as intracranial bleeding. PCC provides a concentrated, active mix of factors II, VII, IX, and X, which can correct the INR within minutes without the high volume-overload risk of fresh frozen plasma (FFP). FFP is now generally considered a second-line option if PCC is unavailable or if the time required for thawing is prohibitive [13].
Step 3: Supportive care. Intracranial hemorrhage requires urgent neurosurgical input, neurological monitoring, and management of raised intracranial pressure. Volume resuscitation may be needed if blood loss is heavy.
Prevention: The Vitamin K Shot at Birth
Prophylactic vitamin K1 at birth is the global standard of care and is endorsed by the American Academy of Pediatrics, the Canadian Paediatric Society, and the World Health Organization [3,4,7].
The standard regimen is a single intramuscular injection of 0.5–1.0 mg of vitamin K1, given within six hours of birth. Preterm infants under 1500 g typically receive a smaller dose (0.3–0.5 mg). The IM dose creates a slow-release reservoir that protects the infant through the entire vulnerable window of up to six months [3].
- 2 mg at birth, 2 mg at 4–6 days, and 2 mg at 4–6 weeks
- Weekly 1 mg doses while breastfeeding [14]
Managing Vitamin K Injection Refusal
Oral vitamin K is generally reserved for families who decline the injection. Major guidelines emphasize that parents who choose the oral route should be clearly informed of the higher residual risk of Late VKDB.
Special Case: Preventing Early VKDB
When mothers take medications that interfere with vitamin K metabolism, oral vitamin K1 has historically been considered for the mother in the weeks before delivery. However, major pediatric and obstetric organizations currently state there is insufficient evidence to recommend routine maternal supplementation to prevent early VKDB. Focus must remain on ensuring the infant receives standard IM prophylaxis immediately at birth [4,15].
Warning Signs Caregivers Should Know
Most cases of VKDB give no warning before bleeding becomes serious. When signs do appear, they may include:
- Unexplained bruising, especially around the head or face
- Bleeding from the umbilical stump, nose, or gums
- Blood in stool, dark tarry stools, or vomit containing blood
- Pale skin or unusual sleepiness
- Poor feeding, irritability, seizures, or a bulging soft spot (signs of brain bleeding)
Any of these in a baby under six months requires urgent medical assessment [7].
Frequently Asked Questions (FAQs)
Why do all newborns need a vitamin K shot, even healthy ones?
Every newborn is born with very low vitamin K stores. Vitamin K does not cross the placenta well, the newborn liver stores only small amounts, and the gut bacteria that make vitamin K2 have not yet established. Without a shot at birth, any infant can develop vitamin K deficiency bleeding, which can cause life-threatening bleeding inside the skull. The intramuscular shot provides a slow-release reservoir that protects the baby for the first six months of life.
Is the vitamin K injection safe?
Yes. The intramuscular vitamin K injection has been used since the 1960s. A single 1992 study suggested a possible link with childhood cancer, but multiple larger studies done since then have found no such link. The medical consensus is that the injection is safe and that the benefit of preventing fatal bleeding far outweighs the brief discomfort of a single injection.
Can vitamin K be given by mouth instead of by injection?
Oral vitamin K is offered in some countries, but it is less reliable than the injection. It requires multiple doses over several weeks, can be vomited up, and may not be absorbed if the baby has an undiagnosed liver or gut problem. Major guidelines, including those from the American Academy of Pediatrics, recommend intramuscular injection as the preferred route. Oral dosing is reserved for families who decline the injection.
What are the warning signs of vitamin K deficiency bleeding in a baby?
Bleeding may have no warning at all, which is why prevention matters so much. When signs do appear, they include unusual bruising (especially around the head or face), bleeding from the umbilical stump or the nose, blood in the stool, pale skin, or vomit that contains blood. Signs of bleeding in the brain include unusual sleepiness, poor feeding, seizures, a bulging soft spot, or sudden vomiting. Any of these signs in a young infant warrants immediate medical attention.
Why is vitamin K deficiency bleeding so dangerous in breastfed babies?
Breast milk contains very low levels of vitamin K compared with infant formula. A breastfed baby who has not received vitamin K prophylaxis at birth is at higher risk of Late VKDB, which often presents with bleeding inside the skull between 2 weeks and 6 months of age. Breastfeeding remains highly recommended, but it does not replace the need for a vitamin K shot at birth.
How do doctors diagnose VKDB in the laboratory?
The classic pattern is a markedly prolonged PT and INR, a normal or mildly raised aPTT, and normal platelet count, fibrinogen, and D-dimer. Elevated PIVKA-II confirms the diagnosis. A rapid normalization of PT and INR within hours of giving vitamin K is itself a strong diagnostic sign and is sometimes called the "therapeutic diagnosis."
Glossary of Related Medical Terms
- Coagulopathy: A condition in which blood does not clot properly, leading to abnormal bleeding.
- Phylloquinone (Vitamin K1): The form of vitamin K found in plants such as leafy greens. This is the form given as prophylaxis at birth.
- Menaquinones (Vitamin K2): Forms of vitamin K made by bacteria living in the human gut.
- Gamma-carboxylation: A chemical step in the liver that switches certain clotting factor proteins from inactive to active. It needs vitamin K to work.
- PIVKA-II (Des-gamma-carboxy prothrombin): The inactive precursor of factor II that builds up when vitamin K is missing. High levels confirm vitamin K deficiency.
- Prothrombin time (PT) and INR: A blood test that measures how long it takes for a clot to form through the extrinsic and common clotting pathways. PT and INR rise sharply in vitamin K deficiency.
- Activated partial thromboplastin time (aPTT): A blood test measuring the intrinsic and common clotting pathways. It may be normal or mildly raised in VKDB.
- Intracranial hemorrhage (ICH): Bleeding inside the skull. The most dangerous complication of Late VKDB.
- Cholestasis: Reduced bile flow from the liver. It interferes with absorption of fat-soluble vitamins, including vitamin K.
- Fresh frozen plasma (FFP): Plasma frozen soon after donation that contains all clotting factors. Used to replace factors quickly during severe bleeding.
- Prothrombin complex concentrate (PCC): A concentrated mix of factors II, VII, IX, and X used for rapid factor replacement.
- Parenteral: Given by injection, usually intramuscular or intravenous, rather than by mouth.
- Prophylaxis: A treatment given to prevent disease before it develops.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Araki, S., & Shirahata, A. (2020). Vitamin K Deficiency Bleeding in Infancy. Nutrients, 12(3), 780. https://doi.org/10.3390/nu12030780
- Sankar, M. J., Chandrasekaran, A., Kumar, P., Thukral, A., Agarwal, R., & Paul, V. K. (2016). Vitamin K prophylaxis for prevention of vitamin K deficiency bleeding: a systematic review. Journal of perinatology : official journal of the California Perinatal Association, 36 Suppl 1(Suppl 1), S29–S35. https://doi.org/10.1038/jp.2016.30
- Ng, E., & Loewy, A. D. (2018). Guidelines for vitamin K prophylaxis in newborns. Paediatrics & child health, 23(6), 394–402. https://doi.org/10.1093/pch/pxy082
- Hand, I., Noble, L., & Abrams, S. A. (2022). Vitamin K and the Newborn Infant. Pediatrics, 149(3), e2021056036. https://doi.org/10.1542/peds.2021-056036
- Loyal, J., & Shapiro, E. D. (2020). Refusal of Intramuscular Vitamin K by Parents of Newborns: A Review. Hospital pediatrics, 10(3), 286–294. https://doi.org/10.1542/hpeds.2019-0228
- Schulte, R., Jordan, L. C., Morad, A., Naftel, R. P., Wellons, J. C., 3rd, & Sidonio, R. (2014). Rise in late onset vitamin K deficiency bleeding in young infants because of omission or refusal of prophylaxis at birth. Pediatric neurology, 50(6), 564–568. https://doi.org/10.1016/j.pediatrneurol.2014.02.013
- Centers for Disease Control and Prevention. (2024, May 15). About vitamin K deficiency bleeding. https://www.cdc.gov/vitamin-k-deficiency/about/index.html
- Centers for Disease Control and Prevention (CDC) (2013). Notes from the field: late vitamin K deficiency bleeding in infants whose parents declined vitamin K prophylaxis--Tennessee, 2013. MMWR. Morbidity and mortality weekly report, 62(45), 901–902.
- Shearer M. J. (2009). Vitamin K deficiency bleeding (VKDB) in early infancy. Blood reviews, 23(2), 49–59. https://doi.org/10.1016/j.blre.2008.06.001
- Orkin, S. H., Fisher, D. E., Look, A. T., Lux, S. E., Ginsburg, D., & Nathan, D. G. (2014). Nathan and Oski's Hematology and Oncology of Infancy and Childhood (8th ed.). Saunders.
- Leijser, L. M., de Vries, L. S., & Cowan, F. M. (2006). Using cerebral ultrasound effectively in the newborn infant. Early human development, 82(12), 827–835. https://doi.org/10.1016/j.earlhumdev.2006.09.018
- U.S. Food and Drug Administration (FDA). (2003). Phytonadione (Vitamin K1) Injection Black Box Warning regarding severe reactions during intravenous administration. Retrieved from FDA prescribing information databases.
- Revel-Vilk S. (2016). Neonatal haemostasis. Impact on bleeding and thrombosis. Hamostaseologie, 36(4), 261–264. https://doi.org/10.5482/HAMO-15-11-0032
- Mihatsch, W. A., Braegger, C., Bronsky, J., Campoy, C., Domellöf, M., Fewtrell, M., Mis, N. F., Hojsak, I., Hulst, J., Indrio, F., Lapillonne, A., Mlgaard, C., Embleton, N., van Goudoever, J., & ESPGHAN Committee on Nutrition (2016). Prevention of Vitamin K Deficiency Bleeding in Newborn Infants: A Position Paper by the ESPGHAN Committee on Nutrition. Journal of pediatric gastroenterology and nutrition, 63(1), 123–129. https://doi.org/10.1097/MPG.0000000000001232
- Kellie F. J. (2017). Vitamin K supplementation during pregnancy for improving outcomes. The Cochrane Database of Systematic Reviews, 2017(6), CD010920. https://doi.org/10.1002/14651858.CD010920.pub2