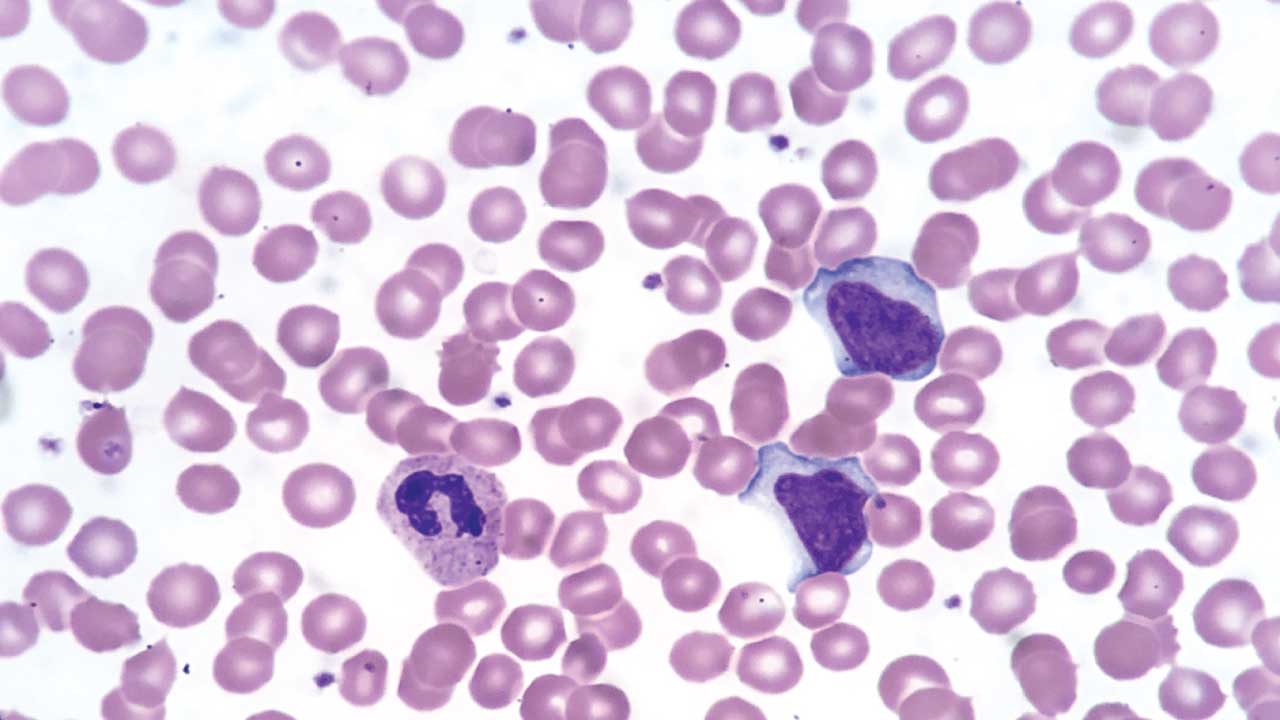
The absolute neutrophil count, or ANC, is one of the most practical numbers in hematology. It tells clinicians exactly how many infection-fighting neutrophils are circulating in a patient's blood at any given moment, rather than relying on the total white blood cell count alone. An ANC calculator takes two values from a complete blood count, the total white blood cell count and the percentage of neutrophils (segmented neutrophils plus bands) from the differential, and converts them into a single, actionable number.
This tool is used daily by oncologists, hematologists, infectious disease specialists, nurses, and pharmacists, particularly when managing patients on chemotherapy, those with bone marrow disorders, or anyone being monitored for neutropenia.
The Formula
The ANC calculator works from this equation:
ANC = Total WBC × (% neutrophils + % bands) ÷ 100
The total WBC comes directly from the complete blood count. The percentage of neutrophils and bands comes from the differential, which breaks the white cell population down by type. Bands are immature neutrophils and are counted alongside mature (segmented) neutrophils because both contribute to infection defense. However, many modern automated hematology analyzers no longer count bands separately, instead grouping all neutrophils together. If a lab report does not list a specific band percentage, clinicians simply use the total neutrophil percentage for the calculation [1].
The ANC Calculator
Absolute Neutrophil Count (ANC)
Interpreting the Result
Once the ANC is calculated, it is matched against standard severity thresholds:
| ANC (cells/µL) | Category | Clinical significance |
|---|---|---|
| ≥ 1,500 | Normal | No increased infection risk from neutrophil count |
| 1,000–1,500 | Mild neutropenia | Usually low clinical concern |
| 500–1,000 | Moderate neutropenia | Increased infection risk; closer monitoring needed |
| < 500 | Severe neutropenia | High infection risk; fever in this range is a medical emergency |
A few interpretation points matter as much as the number itself:
- Trend matters more than a single value. A rising ANC after chemotherapy is reassuring even if the absolute number is still low. A falling ANC needs attention even if it is technically still "normal."
- Context changes the meaning. An ANC of 1,200 in a healthy person and an ANC of 1,200 in a patient three days post-chemotherapy carry very different implications, because the second patient may still be heading toward their nadir.
- Ethnic variation exists. Some individuals, particularly those with the Duffy-null genotype common in African, Middle Eastern, and West Indian ancestry, have a baseline ANC below 1,500 with no increased infection risk. This is a normal variant, not a disease state, and should not automatically trigger the same concern as a treatment-induced drop.
- Fever changes everything. Regardless of the exact ANC value, a single oral temperature of 38.3°C (101°F) or a sustained temperature of 38.0°C (100.4°F) for more than one hour in a patient with an ANC under 500 (or expected to fall below 500) is treated as a medical emergency until proven otherwise [2].
Case Scenarios
Scenario 1: Post-chemotherapy monitoring
A 54-year-old patient on cycle two of chemotherapy for breast cancer has a CBC showing a total WBC of 1,800/µL with 25% neutrophils and 5% bands.
ANC = 540/µL
This falls just above the severe threshold but still in the high-risk range. The patient is afebrile, so no emergency antibiotics are needed, but the care team schedules a repeat CBC in 48 hours and reinforces infection-prevention precautions, since this patient is likely approaching their nadir.
Scenario 2: Febrile neutropenia
A 67-year-old patient with acute myeloid leukemia develops a temperature of 38.4°C. The CBC shows a WBC of 900/µL with 15% neutrophils and 2% bands.
ANC = 153/µL
This is severe neutropenia with fever, meeting the definition of febrile neutropenia. This triggers immediate blood cultures and empiric broad-spectrum antibiotics within the hour, per standard protocol, regardless of how well the patient appears clinically.
Scenario 3: Routine result in a healthy adult
A 29-year-old donor of West African descent has a routine CBC for an unrelated reason. WBC is 3,600/µL with 35% neutrophils and 3% bands.
ANC = 1,368/µL
This sits in the mild neutropenia range by standard cutoffs. However, given the patient's ancestry, baseline health, and lack of infection history, this is most likely a Duffy-null associated neutrophil count rather than a pathological finding. No further workup is needed unless the patient has a history of recurrent or unusual infections.
Scenario 4: Drug-induced neutropenia
A 41-year-old patient recently started on clozapine reports flu-like symptoms. CBC shows WBC of 2,200/µL with 18% neutrophils and 1% bands.
ANC = 418/µL
This is severe neutropenia, and given the timing with clozapine initiation, drug-induced neutropenia is the leading suspect. The medication is held immediately. While the FDA officially eliminated the mandatory Clozapine REMS reporting program in 2025 to improve patient access, the risk of severe neutropenia remains. Therefore, the patient must still be monitored closely with serial CBCs according to the drug's updated prescribing information until the ANC recovers to a safe threshold [3].
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Keohane, E. M., Preston, M. M., Mirza, K. M. & Walenga, J. M. (2024). Rodak's Hematology: Clinical Principles and Applications (7th ed.). Elsevier.
- Freifeld, A. G., Bow, E. J., Sepkowitz, K. A., Boeckh, M. J., Ito, J. I., Mullen, C. A., Raad, I. I., Rolston, K. V., Young, J. A., Wingard, J. R., & Infectious Diseases Society of America (2011). Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 52(4), e56–e93. https://doi.org/10.1093/cid/cir073
- U.S. Food and Drug Administration (FDA). (2025). FDA removes risk evaluation and mitigation strategy (REMS) program for the antipsychotic drug Clozapine. FDA Drug Safety Communication. Retrieved from https://www.fda.gov/drugs/drug-safety-communications/fda-removes-risk-evaluation-and-mitigation-strategy-rems-program-antipsychotic-drug-clozapine