TL;DR
Classic Hodgkin Lymphoma is primarily treated with systemic therapy (chemotherapy, targeted therapy, immunotherapy) and sometimes radiation therapy.
- Early-stage (Stage 1-2) treatment is tailored based on whether the disease is favorable (fewer risk factors) or unfavorable (more risk factors).
- Favorable disease often involves shorter chemotherapy followed by radiation.
- Unfavorable disease may require longer or more intensive chemotherapy, and treatment decisions are guided by PET/CT scans and the Deauville Score.
- Advanced-stage (Stage 3-4) treatment typically involves combination chemotherapy.
- Preferred regimens include Nivolumab + AVD or BrECADD + growth factors.
- Treatment decisions and prognosis are influenced by factors like the International Prognostic Score (IPS) and PET/CT response.
Response Assessment: PET/CT scans and the Deauville Score are crucial for evaluating treatment response and guiding subsequent treatment decisions.
Special Considerations ▾: Treatment approaches may need to be adjusted for specific situations, including pregnancy and older adults. Fertility preservation and management of long-term side effects are also important considerations.
*Click ▾ for more information
Introduction
Hodgkin lymphoma is a type of cancer that starts in white blood cells called lymphocytes and usually begins in the lymph nodes in the upper body. It is a highly curable disease, but effective treatment is crucial. This blog post will explain classic Hodgkin lymphoma and its treatment strategies.
The information provided here is based on the latest recommendations from the National Comprehensive Cancer Network (NCCN). The NCCN is an alliance of top cancer centers in the United States that develops evidence-based guidelines for cancer care. These guidelines are used by healthcare providers worldwide to ensure patients receive the best possible treatment.
This post aims to simplify the NCCN guidelines to help patients and their caregivers better understand Hodgkin lymphoma treatment options.
What is Hodgkin Lymphoma?
Lymphoma is a type of cancer of the lymphocytes. There are two main types of lymphoma: Hodgkin lymphoma and non-Hodgkin lymphoma.
Types of Hodgkin Lymphoma
There are two main types of Hodgkin lymphoma.
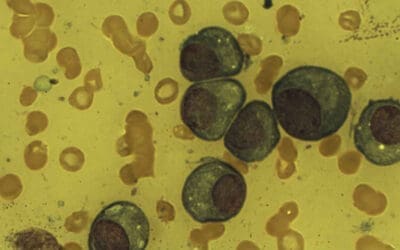
- Classic Hodgkin Lymphoma (CHL): This is the most common type of Hodgkin lymphoma. It is characterized by the presence of large, abnormal lymphocytes called Reed-Sternberg cells. There are several subtypes of classic Hodgkin lymphoma, but the treatment approach is generally the same for all of them.
- Nodular Lymphocyte-Predominant Hodgkin Lymphoma (NLPHL): This is a rare form of Hodgkin lymphoma, characterized by the presence of “popcorn-shaped” cells. It typically grows slowly but can sometimes behave aggressively.
Signs and Symptoms of Hodgkin Lymphoma
- Lymphadenopathy (Swollen Lymph Nodes): This is often the most common symptom. The swelling is usually painless and may occur in the neck, armpits, or groin.
- Unexplained fevers (above 100.4°F or 38°C )
- Drenching night sweats
- Unexplained weight loss
- Itchy skin (pruritus)
- Extreme tiredness despite sleep (fatigue)
- A bad reaction to alcohol (pain in lymph nodes after drinking alcohol)
Laboratory Investigations for Hodgkin Lymphoma Diagnosis
While a lymph node biopsy is the definitive test for diagnosing Hodgkin lymphoma, other laboratory tests play a crucial role in evaluating a patient’s overall health, staging the disease, and monitoring treatment.
Lymph Node Biopsy
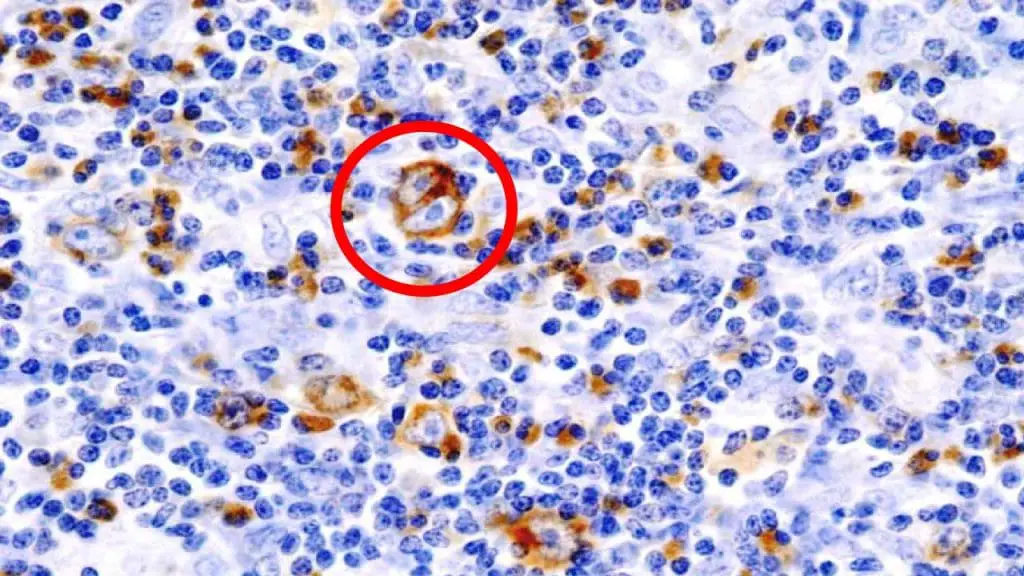
Surgical removal of a lymph node (excisional biopsy) is preferred, but sometimes a needle biopsy (core needle biopsy) is used. Presence of Reed-Sternberg cells is necessary for classic Hodgkin Lymphoma diagnosis. Specific cellular morphology will help indicate the classic Hodgkin Lymphoma subtype (nodular sclerosis, mixed cellularity, lymphocyte-rich, lymphocyte-depleted).
Blood Tests
- Complete Blood Count (CBC): Anemia (low red blood cell count) may be present in some cases.
- Erythrocyte Sedimentation Rate (ESR): Often elevated, indicating inflammation, but this is a non-specific finding (can be elevated in other conditions as well). ESR can be used to monitor treatment response in some cases.
- Comprehensive Metabolic Panel (CMP): Usually normal, but abnormalities may indicate involvement of organs outside the lymphatic system. For example, elevated liver enzymes may suggest liver involvement.
- Serum Lactate Dehydrogenase (LDH): May be elevated, indicating a higher tumor burden or more aggressive disease. Like ESR, LDH is a non-specific marker.
- Testing for HIV: To determine HIV status, as HIV infection can affect Hodgkin lymphoma presentation and treatment.
- Testing for Hepatitis B and C: To determine Hepatitis B and C status, as these infections can impact treatment options (especially chemotherapy)/
Imaging Studies for Hodgkin Lymphoma Staging
Imaging tests are a crucial part of diagnosing and staging Hodgkin lymphoma, as well as monitoring how well treatment is working. These tests allow doctors to visualize the lymph nodes and other organs in the body to identify areas affected by lymphoma.
| Imaging Study | Purpose | Procedure | Expected Findings |
| PET/CT Scan | – Determines stage – Evaluates treatment response | – Injection of radioactive glucose (FDG)- PET scan detects FDG uptake – CT scan provides anatomical images | -“Hot spots” of increased FDG uptake indicate lymphoma – Deauville Score assesses treatment response (1-3 = good, 4-5 = residual lymphoma/progression) |
| CT Scan | – Detailed anatomical images – Staging and tumor size assessment | – X-rays from multiple angles – Computer creates cross-sectional images – May use contrast | – Enlarged lymph nodes – Tumor masses – Organ involvement (spleen, liver) |
| MRI Scan | – Detailed soft tissue images – Evaluation of brain, spinal cord, bones | – Radio waves and magnetic field – No radiation – May use contrast | – Similar to CT findings (enlarged lymph nodes, tumors, organ involvement) – Greater soft tissue detail |
| Chest X-ray | – Detects enlarged lymph nodes in the chest | – Quick X-ray of the chest | – Widening of the mediastinum (suggestive of enlarged lymph nodes) |
What is the Deauville Score?
The Deauville Score is a 5-point scale used to assess the response to treatment in Hodgkin lymphoma, particularly on PET scans. It measures the amount of FDG (a radioactive glucose tracer) uptake in areas where lymphoma was present before treatment, compared to the FDG uptake in healthy tissues.
So it provides a standardized way to determine if the lymphoma is responding to the treatment. Based on the Deauville Score, doctors may decide to continue the current treatment, switch to a different treatment, or consider additional therapies like stem cell transplantation. The Deauville Score can also help predict the likelihood of long-term remission.
| Score | FDG Uptake | Interpretation |
| 1 | No uptake or uptake ≤ mediastinum | Complete response |
| 2 | Uptake ≤ liver | Good response |
| 3 | Uptake > liver, but < new lesions | Intermediate response |
| 4 | Uptake moderately > liver | Less favorable response/residual disease |
| 5 | Uptake markedly > liver or new lesions | Treatment failure/progressive disease |
The Four Stages of Hodgkin Lymphoma

Determining the stage of Hodgkin lymphoma is essential for planning the right treatment and understanding the outlook. This involves carefully assessing how far the lymphoma has spread, mainly using imaging tests along with information from physical exams and lab work. Doctors use the Lugano classification to stage Hodgkin lymphoma, which relies heavily on PET-CT scans, though the older Ann Arbor system is still sometimes used in the NCCN guideline.
There are four stages of Hodgkin lymphoma.
- Stage 1: The cancer is in only one group of lymph nodes and possibly in one small area or organ outside the lymphatic system.
- Stage 2: The cancer has spread to two or more groups of lymph nodes on the same side of the diaphragm. It may also have spread to one area or organ and its nearby lymph nodes outside the lymphatic system.
- Stage 3: The Hodgkin lymphoma is found in lymph nodes both above and below the diaphragm. It might also be in one area or organ outside the lymphatic system, in the spleen, or both.
- Stage 4: The cancer has spread to multiple areas in one or more organs outside the lymphatic system. It may also be in lymph nodes near those organs. Or, it may be in one organ outside the lymphatic system and also in distant lymph nodes.
A and B Symptoms
- A “B” after the stage means the cancer is causing B symptoms: unexplained fevers, drenching night sweats, and significant weight loss.
- An “A” after the stage means the cancer is not causing B symptoms.
Early vs. Advanced Classic Hodgkin Lymphoma
- Stages 1 and 2 are considered early classic Hodgkin lymphoma.
- Stages 3 and 4 are considered advanced classic Hodgkin lymphoma.
Types of Treatment for Classic Hodgkin Lymphoma
Classic Hodgkin lymphoma is primarily treated with chemotherapy, and sometimes radiation therapy is added to the treatment plan.
Systemic Therapy
Systemic therapy involves using medications to target and kill cancer cells throughout the body. The main types of systemic therapy for Hodgkin lymphoma are:
- Chemotherapy: Chemotherapy drugs are the foundation of classic Hodgkin lymphoma treatment. They work by attacking rapidly dividing cells, including lymphoma cells. Chemotherapy is typically given intravenously (through a vein) in cycles, with rest periods in between to allow the body to recover.
- Targeted Therapy: These drugs are designed to target specific molecules or pathways involved in cancer cell growth and survival. Brentuximab vedotin is an example of a targeted therapy called an antibody-drug conjugate. It combines an antibody that recognizes a specific protein on Hodgkin lymphoma cells (CD30) with a chemotherapy drug, delivering the drug directly to the cancer cells.
- Immunotherapy: Immunotherapy drugs help the body’s own immune system recognize and attack cancer cells. Checkpoint inhibitors, such as nivolumab and pembrolizumab, are a type of immunotherapy that can be used in Hodgkin lymphoma.
Common Chemotherapy Regimens
Chemotherapy regimens involve combinations of different chemotherapy drugs given together to maximize their effectiveness. Some commonly used regimens for Hodgkin lymphoma are described in the table below.
| Regimen | Components |
| ABVD | Doxorubicin (Adriamycin), Bleomycin, Vinblastine, Dacarbazine |
| BrECADD + G-CSF | Brentuximab vedotin, Epirubicin, Cyclophosphamide, Doxorubicin, Dacarbazine, plus growth factors (G-CSF). G-CSF is a growth factor that helps boost the immune system by stimulating the production of white blood cells, which can be reduced by chemotherapy. |
| BV-AVD + G-CSF | Brentuximab vedotin, Doxorubicin |
| Nivolumab and AVD | This regimen combines the immunotherapy drug nivolumab with the AVD chemotherapy drugs (Doxorubicin, Vinblastine, and Dacarbazine). |
Radiation Therapy
Radiation therapy uses high-energy rays to kill cancer cells in specific areas of the body. It is often used in combination with chemotherapy to treat Hodgkin lymphoma.
Involved-site radiation therapy (ISRT) is a technique that targets the radiation specifically to the lymph nodes where the cancer started, minimizing damage to surrounding healthy tissues.
Alright, let’s break down the treatment approaches for early-stage classic Hodgkin lymphoma (CHL), including the definitions of favorable and unfavorable early-stage disease.
Treatment Approaches for Early-Stage Classic Hodgkin Lymphoma (Stages 1-2)
Early-stage Hodgkin lymphoma refers to stages 1 and 2 of the disease. The treatment approach depends on whether the early-stage disease is considered “favorable” or “unfavorable,” as these categories help predict the risk of relapse.
Favorable Early-Stage Classic Hodgkin Lymphoma
Favorable early-stage classic Hodgkin lymphoma generally means that the lymphoma is limited and the patient has fewer risk factors for relapse.
Favorable early-stage classic Hodgkin lymphoma is defined by the absence of the following risk factors:
- B symptoms (unexplained fevers, drenching night sweats, weight loss)
- Bulky tumors (larger than 10 cm)
- Elevated erythrocyte sedimentation rate (ESR)
- Involvement of more than 2 areas
- Involvement of areas other than lymph nodes, such as a lung
Treatment approach typically involves a shorter course of chemotherapy (e.g., 2 cycles of ABVD) followed by radiation therapy to the involved field (ISRT). The goal is to achieve a high cure rate while minimizing long-term side effects from treatment.
PET scans are used to assess response after chemotherapy. Treatment decisions are guided by the PET scan results. The Deauville Score is used to interpret the PET scan results.
| Deauville Score | Interpretation | Treatment Response | Action |
| 1-3 | Good response | Favorable | – If initial treatment was 2 cycles ABVD, consider radiation therapy. – Some treatment plans may involve 2 more cycles of ABVD instead of radiation |
| 4 | Intermediate response | Less favorable | – Typically, 2 additional cycles of ABVD are given. – Response is reassessed after these additional cycles. |
| 5 | Poor response | Treatment failure / Progressive disease | – A biopsy is performed to confirm the presence of active lymphoma. – If lymphoma is confirmed, treatment strategies for refractory (resistant) Hodgkin lymphoma are considered. |
Unfavorable Early-Stage Classic Hodgkin Lymphoma
Unfavorable early-stage classic Hodgkin lymphoma indicates a higher risk of relapse due to the presence of certain risk factors.
Unfavorable early-stage classic Hodgkin lymphoma is defined by the presence of any of the following risk factors:
- B symptoms (unexplained fevers, drenching night sweats, weight loss)
- Bulky tumors (larger than 10 cm)
- Elevated erythrocyte sedimentation rate (ESR)
- Involvement of more than 2 areas
- Involvement of areas other than lymph nodes, such as a lung
Treatment approach usually involves a longer course of chemotherapy (e.g., 4 cycles of ABVD) and may or may not include radiation therapy. More intensive chemotherapy regimens may be considered in some cases. The goal is to reduce the risk of relapse, even if it means more treatment.
PET scans are crucial for assessing response.
Treatment Pathways for Unfavorable Stage 1-2 Classic Hodgkin Lymphoma
| Pathway | Initial Treatment | Subsequent Treatment |
| ABVD Pathway | 2 cycles of ABVD chemotherapy | – Deauville Score 1-3: 4 cycles of AVD chemotherapy or 2 cycles of ABVD + radiation therapy. – Deauville Score 4-5: 2 more cycles of ABVD or 2 cycles of BrECADD + G-CSF. |
| Immunotherapy Pathway | 4 cycles of nivolumab + AVD chemotherapy; Radiation therapy | – Deauville Score 1-3: Begin follow-up care. – Deauville Score 4-5: Biopsy. If biopsy is negative, begin follow-up care. If biopsy is positive, treatment for refractory CHL. |
| Brentuximab Vedotin Pathway | 4 cycles of brentuximab vedotin + AVD chemotherapy + growth factors; Radiation therapy | – Deauville Score 1-3: Begin follow-up care. – Deauville Score 4-5: Biopsy. If biopsy is negative, begin follow-up care. If biopsy is positive, treatment for refractory CHL. |
| BrECADD Pathway | 2 cycles of BrECADD chemotherapy + growth factors | – Deauville Score 1-3: 2 more cycles of BrECADD chemotherapy + growth factors, then restaging. – If interim Deauville Score 1-3, begin follow-up care. – If interim Deauville Score 4-5, biopsy. If biopsy is negative, 4 cycles BrECADD + growth factors. – If results are good, follow-up care. – If biopsy is positive, treatment for refractory CHL. |
Treatment Approaches for Advanced-Stage Classic Hodgkin Lymphoma (Stage 3-4)
Advanced-stage classic Hodgkin lymphoma (CHL) means the lymphoma has spread below the diaphragm and may involve areas outside the lymphatic system. Treatment for advanced-stage classic Hodgkin lymphoma aims to achieve a cure while managing potential side effects.
Preferred Chemotherapy Regimens
The NCCN guidelines emphasize that certain chemotherapy regimens are preferred for advanced classic Hodgkin lymphoma due to evidence of better efficacy and safety.
- Nivolumab + AVD: This regimen combines the immunotherapy drug nivolumab with AVD chemotherapy (doxorubicin, vinblastine, and dacarbazine). Treatment typically involves 6 cycles of nivolumab and AVD. Response to treatment is assessed using the Deauville score on PET/CT scans. If the Deauville score is 1, 2, or 3, no further treatment is needed after completing the planned cycles. If the Deauville score is 4 or 5, a biopsy may be recommended to guide further management.
- BrECADD + Growth Factors: This regimen is a more intensive chemotherapy combination that includes brentuximab vedotin, etoposide, cyclophosphamide, doxorubicin, dacarbazine, and dexamethasone, along with growth factors (G-CSF). Treatment starts with 2 cycles of BrECADD plus growth factors. Response is assessed with PET/CT scans and the Deauville score. If the Deauville score is 1, 2, or 3 after the initial 2 cycles, 2 more cycles of BrECADD are typically given. If the response is good, no further treatment is needed. If the Deauville score is 4 or 5 after the initial cycles, a biopsy is recommended to determine the next steps.
Regimens Used in Certain Cases
If the preferred regimens are not suitable or available, other chemotherapy options may be considered.
- BV-AVD with Growth Factors: This regimen combines brentuximab vedotin with AVD chemotherapy and growth factors. Treatment usually involves 6 cycles. Further treatment decisions are based on the Deauville score after restaging.
International Prognostic Score (IPS)
The International Prognostic Score (IPS) is a scoring system that helps predict the likelihood of treatment success in advanced-stage CHL. It considers several factors:
- Age 45 or older
- Male sex
- Stage 4 disease
- Albumin level below 4 g/dL
- Low hemoglobin level
- High white blood cell count
- Low lymphocyte count
Each risk factor present contributes one point to the IPS. A higher IPS indicates a less favorable prognosis.
Special Considerations for Classic Hodgkin Lymphoma
Several unique factors can influence treatment decisions and management of Hodgkin lymphoma.
Pregnancy
Treatment of Hodgkin lymphoma during pregnancy requires careful consideration to balance the health of the mother and the developing fetus. Some chemotherapy drugs can harm the fetus, so treatment plans may need to be modified or delayed if possible.
Radiation therapy is generally avoided during pregnancy, especially to the abdomen and pelvis. A multidisciplinary team, including experts in hematology, oncology, and maternal-fetal medicine, is essential to develop an individualized treatment strategy.
Older Adults
Older adults (≥ 60 years old) with Hodgkin lymphoma may have other health conditions that can affect their ability to tolerate treatment. Treatment approaches may need to be adjusted to minimize toxicity and maintain quality of life.
Factors such as frailty, organ function, and comorbidities are carefully considered when making treatment decisions. Clinical trials are ongoing to evaluate the safety and effectiveness of less toxic regimens for older adults with Hodgkin lymphoma.
Fertility Preservation
Some Hodgkin lymphoma treatments can affect fertility in both men and women. It is important to discuss fertility preservation options before starting treatment, especially for patients who wish to have children in the future. Fertility preservation methods are available, including sperm banking for men and egg or ovarian tissue freezing for women.
Long-Term Side Effects
While Hodgkin lymphoma is often curable, treatment can increase the risk of developing long-term side effects, such as:
- Heart problems
- Lung damage
- Secondary cancers
Patients should receive regular follow-up care to monitor for and manage any potential long-term complications.
Supportive Care
Supportive care is an essential part of Hodgkin lymphoma treatment, focusing on managing symptoms and side effects, and improving overall quality of life.
This may include:
- Pain management
- Nutritional support
- Emotional and psychological support
- Social support
Disclaimer: This article is intended for informational purposes only and is specifically targeted towards medical students. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Hoppe RT, Advani RH, Ai WZ, Ambinder RF, Armand P, Bello CM, Benitez CM, Chen W, Dabaja B, Daly ME, Gordon LI, Hansen N, Herrera AF, Hochberg EP, Johnston PB, Kaminski MS, Kelsey CR, Kenkre VP, Khan N, Lynch RC, Maddocks K, McConathy J, Metzger M, Morgan D, Mulroney C, Pullarkat ST, Rabinovitch R, Rosenspire KC, Seropian S, Tao R, Torka P, Winter JN, Yahalom J, Yang JC, Burns JL, Campbell M, Sundar H. NCCN Guidelines® Insights: Hodgkin Lymphoma, Version 2.2022. J Natl Compr Canc Netw. 2022 Apr;20(4):322-334. doi: 10.6004/jnccn.2022.0021. PMID: 35390768.
- Engert A, Younes A. Hodgkin Lymphoma: A Comprehensive Overview (Hematologic Malignancies) 3rd Edition (Springer). 2020.
- Hoppe, RT, Mauch PM, Armitage JO, Volker D, Weiss LM. Hodgkin Lymphoma 2nd Edition (Lippincott Williams & Wilkins). 2007.
- https://www.nccn.org/patients/guidelines/content/PDF/hodgkin-patient.pdf
- https://www.nccn.org/professionals/physician_gls/pdf/hodgkins.pdf