Key Takeaways
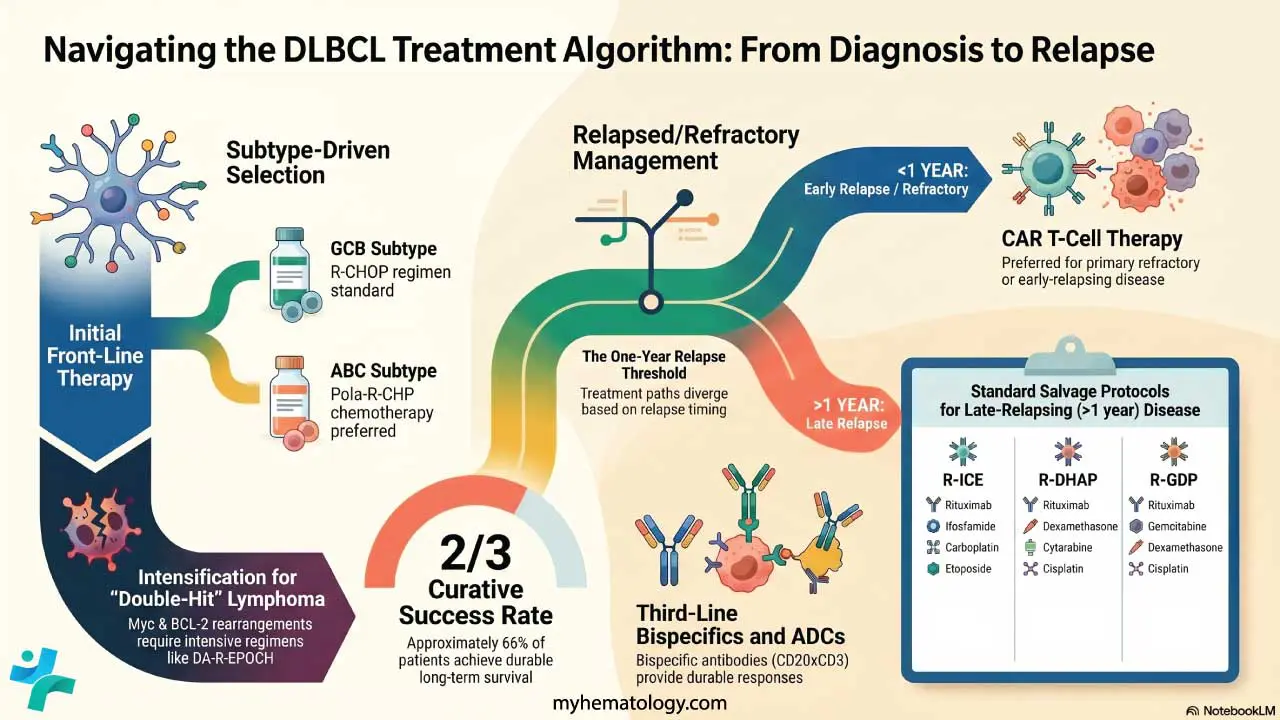
- DLBCL is treatable with curative intent. Approximately two thirds of patients achieve long-term remission with first-line therapy. R-CHOP remains the backbone of initial treatment for most patients.
- Subtype matters. Molecular classification into ABC versus GCB subtypes now directly influences treatment selection. Patients with the ABC subtype benefit from the addition of polatuzumab vedotin (Pola-R-CHP), while double-hit lymphomas require more intensive regimens.
- CAR T-cell therapy has changed the relapse story. For patients whose disease returns early or never responded to initial treatment, CAR T-cell therapy now offers four-year event-free survival rates around 40%, significantly better than previous standard approaches.
- New options exist even for the hardest-to-treat cases. Bispecific antibodies like glofitamab and epcoritamab offer meaningful response rates in patients who have failed multiple prior therapies, though they are not curative for most in this setting.
What Is DLBCL?
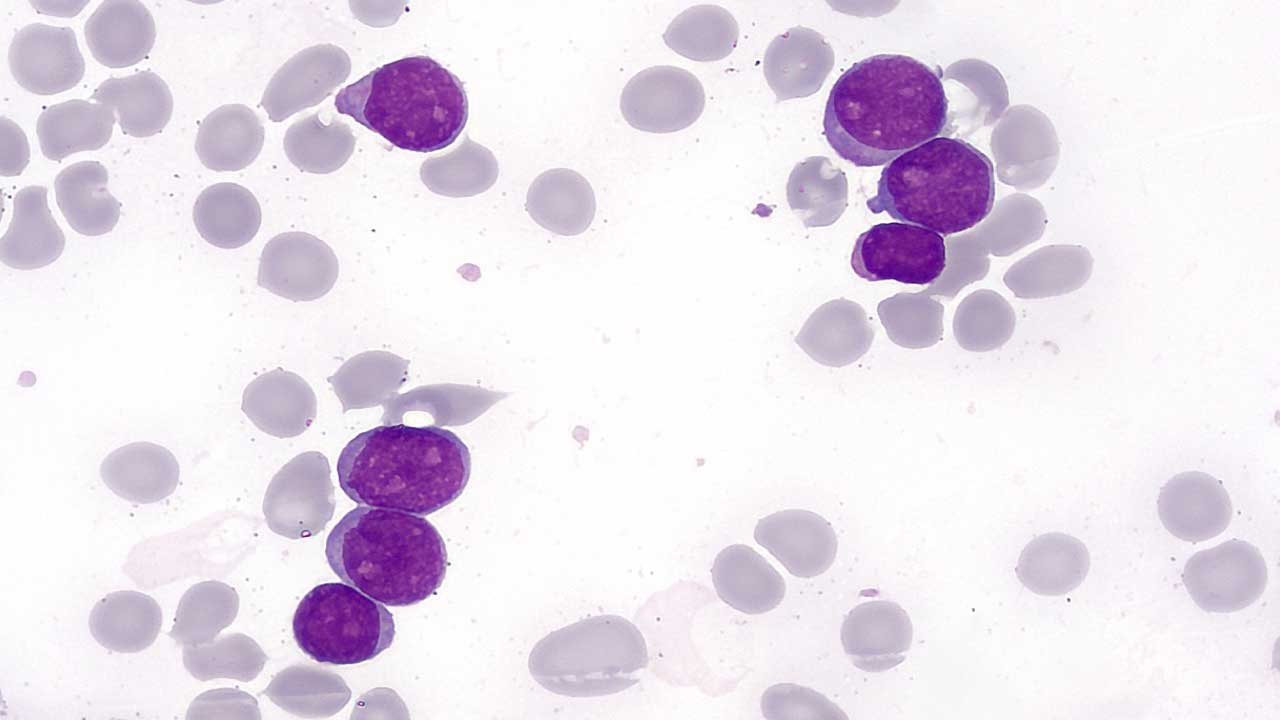
Imagine your immune system's white blood cells suddenly start growing out of control. That is, at its core, what happens in diffuse large B-cell lymphoma, or DLBCL. It is the most common subtype of non-Hodgkin lymphoma, making up roughly 30% of all lymphoma diagnoses worldwide. It is also fast-growing and aggressive.
Two hematologists from the Mayo Clinic, Drs. Stephen Ansell and Grzegorz Nowakowski, published a comprehensive treatment algorithm review in Blood Cancer Journal in March 2026. Their paper synthesises decades of clinical trial data into a clear, practical roadmap for managing this disease. This article unpacks that roadmap in plain language.
The Foundation: A Chemotherapy Regimen That Has Stood the Test of Time
For more than two decades, the standard starting treatment for DLBCL has been a drug combination called R-CHOP. This stands for rituximab (a targeted antibody that marks cancer cells for destruction by the immune system), combined with four chemotherapy agents: cyclophosphamide, doxorubicin, vincristine, and prednisone.
R-CHOP works remarkably well. Approximately 60% of patients treated with it achieve long-term, durable remission. That is not a small number. For a disease that is aggressive and fast-moving, six in ten patients going on to live cancer-free lives is a meaningful achievement.
However, the remaining 40% either do not respond well to initial treatment or relapse after it. That gap has driven enormous research efforts over the past decade, and the results are beginning to show.
Not All DLBCL Is the Same
One of the most important developments in hematology has been the recognition that DLBCL is not a single, uniform disease. It contains distinct subtypes, each with different biology and different behaviour.
Using a technique called gene expression profiling (a test that reads which genes are switched on or off inside cancer cells), researchers identified two major subtypes:
- Germinal centre B-cell (GCB) subtype: tends to respond better to standard treatment
- Activated B-cell (ABC) subtype: tends to have worse outcomes with R-CHOP alone
A simpler laboratory test called the Hans algorithm, using standard tissue staining, is widely used to classify these subtypes. However, it can misclassify approximately 20% of cases, which is an important limitation to keep in mind.
Beyond cell of origin, some patients have a particularly aggressive variant where both the Myc and BCL-2 genes are rearranged. These "double-hit" lymphomas behave more aggressively and require a more intensive treatment approach from the start.
Tailoring Treatment: Pola-R-CHP for the ABC Subtype
For patients with the ABC subtype, a modified regimen called Pola-R-CHP is now commonly used. This replaces vincristine in R-CHOP with polatuzumab vedotin, an antibody-drug conjugate. Think of it as a guided missile: the antibody seeks out cancer cells, and the attached chemotherapy payload is delivered directly into them, minimising harm to healthy tissue.
The landmark POLARIX trial compared Pola-R-CHP to standard R-CHOP in previously untreated DLBCL patients. It found a modest but statistically significant improvement in progression-free survival (the time patients live without the disease getting worse): approximately 6% better at two years with Pola-R-CHP. No significant difference in overall survival was demonstrated, and this remains an area of ongoing follow-up.
When DLBCL Comes Back: The Relapse Roadmap
Despite best efforts, at least one in three patients will see their disease return. What happens next depends heavily on when the relapse occurs.
Early relapse (within 12 months) or primary refractory disease (never responded to initial therapy)
This group has historically had very poor outcomes with traditional salvage chemotherapy followed by a stem cell transplant. The picture changed significantly with the approval of CAR T-cell therapy (chimeric antigen receptor T-cell therapy), which involves collecting a patient's own immune cells, engineering them in a laboratory to specifically recognise and attack DLBCL cells, and infusing them back into the patient.
Two products are now approved in this setting. The ZUMA-7 trial studied axicabtagene ciloleucel and found a four-year event-free survival of approximately 40% in early-relapse patients, far superior to the standard chemotherapy-transplant approach. The TRANSFORM trial found similar benefits for lisocabtagene maraleucel, showing a complete response rate of around 74%. These are not small improvements. For patients who previously had very few options, CAR T-cell therapy represents a genuine shift in what is achievable.
Late relapse (more than 12 months after initial treatment)
Patients in this group generally have a more favourable biology. Standard practice remains salvage chemotherapy followed by autologous stem cell transplant (ASCT), where the patient's own stem cells are collected, stored, and reinfused after high-dose chemotherapy destroys remaining cancer cells. This approach results in long-term remission in a meaningful proportion of patients who respond to salvage therapy.
After CAR T-Cell Therapy: What Next?
CAR T-cell therapy is not the end of the road for everyone. Some patients are ineligible due to age, fitness, or lack of access. Others respond initially but then relapse again. For this group, management shifts toward controlling the disease rather than curing it, using newer targeted agents.
Bispecific antibodies are among the most promising of these. They are engineered proteins designed to simultaneously bind to cancer cells and recruit immune cells to destroy them. Two approved agents are:
- Glofitamab: achieved a complete response rate of approximately 35% in heavily pre-treated patients in clinical trials
- Epcoritamab: similarly showed complete response rates of around 39% in patients who had failed multiple prior therapies
These are not cures for most patients in this late-stage setting, but they offer meaningful disease control where few alternatives previously existed.
Special Populations: Elderly and Frail Patients
DLBCL is not only a disease of younger adults. Many patients are elderly or have significant other health conditions that make standard R-CHOP too toxic. For patients over 80, a reduced-intensity regimen called R-miniCHOP has been studied. A phase 2 trial reported a two-year progression-free survival of approximately 50% with this gentler approach, offering a real treatment option where previously many patients were deemed unfit for any therapy.
For patients with central nervous system (CNS) involvement, meaning the lymphoma has spread to the brain or spinal fluid, outcomes remain substantially worse. Even with intensive treatment including high-dose methotrexate, long-term event-free survival ranges from approximately 39% to 67% depending on disease characteristics.
What the Future Looks Like
The field is now actively testing whether newer agents can be moved earlier. Several clinical trials are exploring the use of CAR T-cell therapy and bispecific antibodies in the front-line setting, in combination with or as a replacement for standard chemotherapy. If successful, this could raise the proportion of patients achieving long-term remission from the current two-thirds to something higher.
Limitations to Keep in Mind
This paper is a narrative review and treatment algorithm, not a new clinical trial. It synthesises evidence from multiple existing studies and reflects the practice of a major academic centre in the United States. Several important caveats apply:
- The recommendations assume access to advanced diagnostics, CAR T-cell manufacturing facilities, and specialist haematology units, which are not universally available.
- Treatment algorithms from high-income settings may not be directly applicable in resource-limited environments.
- The Hans algorithm used to classify subtypes can misclassify roughly 20% of patients.
- Many of the trials cited excluded elderly or frail patients, so applicability to real-world populations with multiple comorbidities requires clinical judgement.
Based on: Ansell, S. M., & Nowakowski, G. S. (2026). Current treatment algorithm: diffuse large B-cell lymphoma. Blood Cancer Journal, 16, Article 32. https://doi.org/10.1038/s41408-026-01458-2
References
- Ansell, S. M., & Nowakowski, G. S. (2026). Current treatment algorithm: diffuse large B-cell lymphoma. Blood Cancer Journal, 16, Article 32. https://doi.org/10.1038/s41408-026-01458-2
- Coiffier, B., Lepage, E., Briere, J., Herbrecht, R., Tilly, H., Bouabdallah, R., Morel, P., Van Den Neste, E., Salles, G., Gaulard, P., Reyes, F., Lederlin, P., & Gisselbrecht, C. (2002). CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. The New England journal of medicine, 346(4), 235–242. https://doi.org/10.1056/NEJMoa011795
- Tilly, H., Morschhauser, F., Sehn, L. H., Friedberg, J. W., Trněný, M., Sharman, J. P., Herbaux, C., Burke, J. M., Matasar, M., Rai, S., Izutsu, K., Mehta-Shah, N., Oberic, L., Chauchet, A., Jurczak, W., Song, Y., Greil, R., Mykhalska, L., Bergua-Burgués, J. M., Cheung, M. C., … Salles, G. (2022). Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. The New England journal of medicine, 386(4), 351–363. https://doi.org/10.1056/NEJMoa2115304
- Locke, F. L., Miklos, D. B., Jacobson, C. A., Perales, M. A., Kersten, M. J., Oluwole, O. O., Ghobadi, A., Rapoport, A. P., McGuirk, J., Pagel, J. M., Muñoz, J., Farooq, U., van Meerten, T., Reagan, P. M., Sureda, A., Flinn, I. W., Vandenberghe, P., Song, K. W., Dickinson, M., Minnema, M. C., … All ZUMA-7 Investigators and Contributing Kite Members (2022). Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. The New England journal of medicine, 386(7), 640–654. https://doi.org/10.1056/NEJMoa2116133
- Dickinson, M. J., Carlo-Stella, C., Morschhauser, F., Bachy, E., Corradini, P., Iacoboni, G., Khan, C., Wróbel, T., Offner, F., Trněný, M., Wu, S. J., Cartron, G., Hertzberg, M., Sureda, A., Perez-Callejo, D., Lundberg, L., Relf, J., Dixon, M., Clark, E., Humphrey, K., … Hutchings, M. (2022). Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. The New England journal of medicine, 387(24), 2220–2231. https://doi.org/10.1056/NEJMoa2206913