Procedure At A Glance
Rh typing is a serologic test that determines whether red blood cells carry the RhD antigen, and in extended panels, the C, c, E, and e antigens. It is essential for safe transfusion and for preventing hemolytic disease of the fetus and newborn (HDFN).
- Label tubes.
- Add a drop of a 3-5% patient red cell suspension to the appropriately labeled tubes.
- Add one drop of Anti-D antiserum to the Anti-D labeled tube and one drop of control reagent to the control tube.
- Gently mix the contents of each tube.
- Incubate the tubes at the recommended temperature.
- Centrifuge the tubes.
- Gently resuspend the red cell buttons and observe for agglutination (clumping of red cells).
Introduction
The Rh system is the next most clinically important blood group after ABO blood group, and Rh typing is part of every pre-transfusion workup and every prenatal panel. The reason is anti-D. Antibodies against the RhD antigen are highly immunogenic, almost always IgG, and able to cross the placenta. That combination causes two serious problems: hemolytic transfusion reactions in sensitized recipients and HDFN in babies of sensitized mothers [6]. A simple, accurate Rh typing protocol is what stands between those problems and the patient.
This article walks through the tube method for Rh typing. The tube method is still taught because it makes the underlying immunology visible. You can see the antibody find its antigen. Once you understand the tube test, gel cards and solid-phase systems become much easier to interpret.
A Brief History
The first anti-D-like antibody was described by Levine and Stetson in 1939, in a postpartum patient who had a hemolytic transfusion reaction from her husband's blood [6]. The name "Rh" came a year later, when Landsteiner and Wiener (1940) raised an antibody in animals immunized with rhesus monkey red cells. The two antibodies turned out to recognize different antigens, but the name stuck.
What Is the Rh Blood Group System?
The Rh system is built on two genes on chromosome 1: RHD and RHCE. Each codes for a transmembrane protein that crosses the red cell membrane 12 times and transport gases such as ammonia [6,7]. These two proteins are highly homologous, differing by only 32 to 35 amino acids, which explains why distinguishing them historically required complex serological and genetic analysis [6].
- RHD is either present or absent. Present gives the Rh D+ phenotype; absent gives Rh D−.
- RHCE is always present, and alternative splicing produces proteins carrying the C or c, and E or e antigens.
For routine clinical work, "Rh typing" usually means RhD typing alone. Anti-D causes most of the clinical trouble. Anti-C, anti-c, anti-E, and anti-e occur less often but can still cause transfusion reactions and HDFN, so extended typing (full C, c, E, e panel) is performed when those antibodies are detected, in chronic transfusion patients, and in selected prenatal cases. Note that anti-d does not exist — there is no "d" antigen, only the absence of D.
Principle of Rh Typing
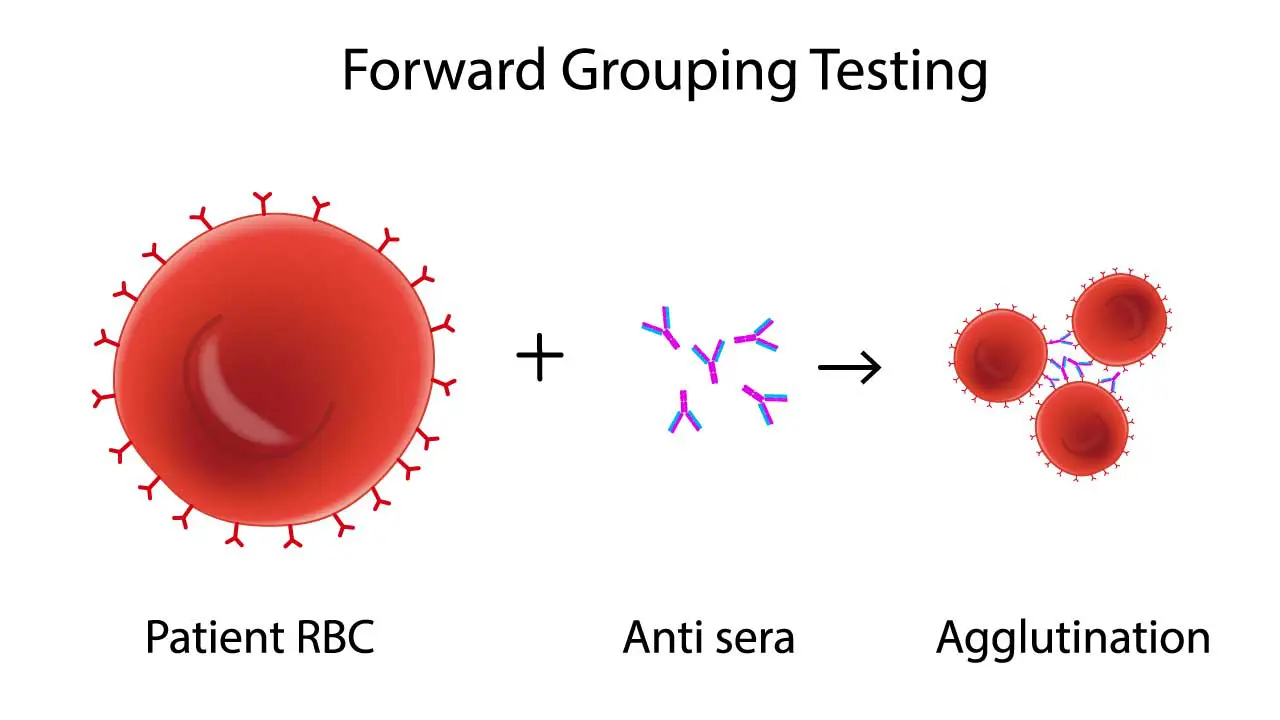
Rh typing is an antigen-antibody reaction read by eye. The patient's red cells are mixed with reagent antibody of known specificity. If the matching antigen is on the cell, the antibody binds, the cells bridge to each other, and visible agglutination forms. No agglutination means no antigen.
The tube format adds two practical steps that make the reaction easier to read:
- Centrifugation brings cells together, increasing the chance that antibody bridges can form.
- Gentle resuspension then tests whether those bridges hold. True agglutinates stay clumped; non-specific cell pellets fall apart.
The control tube uses the same red cells with no anti-D (just diluent or 6% albumin, depending on the reagent system). It must show no agglutination. If it does, the test is invalid until the cause is identified.
Modern reagents are mostly FDA-licensed monoclonal IgM/IgG blend anti-D reagents. The IgM component allows for immediate spin detection, while the IgG component allows the same reagent to be carried through to the 37°C and anti-human globulin (AHG) phases for weak D testing [8]. They are sensitive enough to detect most clinically relevant D antigen expression at immediate spin and they correctly type the partial D variant DVI as D-negative for recipient testing, which is what we want [4].
Materials
For routine RhD typing, plus extended Rh phenotyping when ordered:
- 10 mm × 75 mm glass or polypropylene test tubes
- Calibrated serofuge (or standard centrifuge with manufacturer's calibration)
- Pasteur pipettes
- Patient's EDTA whole blood
- Normal saline (0.9%) for washing red cells
- Commercially prepared monoclonal anti-D, and for extended phenotyping, anti-C, anti-c, anti-E, and anti-e
- Manufacturer-supplied diluent or 6% bovine albumin for the control tube
Specimen and Cell Suspension Preparation
- Centrifuge the EDTA tube to pack cells.
- Wash the cells three times with normal saline to remove plasma proteins (this prevents rouleaux and false positives).
- Prepare a 3–5% red cell suspension in saline. A practical guide is one drop of packed cells in roughly 20 drops of saline.
Protocol (Immediate Spin)
The instructions below assume monoclonal IgM/IgG blend anti-D, the standard reagent in most modern labs. Always follow your reagent manufacturer's package insert if it differs.
- Label two tubes: "Anti-D" and "Control."
- Add one drop of 3–5% washed patient red cell suspension to each tube.
- Add one drop of monoclonal anti-D reagent to the Anti-D tube. Add one drop of saline or 6% albumin (per manufacturer) to the Control tube.
- Mix gently by tapping the tube.
- Centrifuge at the manufacturer's calibrated immediate-spin setting (typically about 15 seconds at ~3,400 RPM, or the RCF specified in the package insert).
- Resuspend the cell button gently by tapping. Read against a well-lit white background or using an agglutination viewer.
- Grade agglutination from 0 to 4+ (see table below).
- Record results. If the Anti-D tube is negative in a recipient where weak D testing is indicated (donors, neonates of RhD-negative mothers, or unexplained discrepancies), proceed to the weak D / RHD genotyping pathway described later [1, 3].
For Extended Rh Phenotyping
Repeat steps 1–7 using anti-C, anti-c, anti-E, and anti-e in their own labeled tubes alongside an additional control.
Interpretation
Read the Control tube first. It must be 0 (no agglutination). Note that when using modern low-protein reagents, a dedicated Rh control is strictly required only for patients who type as AB Positive; for other blood types, the negative reverse typing tubes serve as an internal negative control [8]. If the control reacts, do not interpret the rest of the panel. Move to troubleshooting.
- Agglutination in the Anti-D tube → RhD antigen present → Rh D-positive.
- No agglutination in the Anti-D tube → RhD antigen not detected at immediate spin. For most adult recipients, report as Rh D-negative. For donors, neonates of RhD-negative mothers, and other indicated cases, reflex to weak D testing or RHD genotyping [1].
Agglutination Grading
Advanced reference laboratories may use the numeric Marsh scoring system (e.g., 12, 10, 8) alongside these grades for antibody titration studies, but routine typing requires only the 0 to 4+ visual grading scale.
| Symbol | Score | Description |
|---|---|---|
| 4+ (C, complete) | 12 | One solid cell button, clear supernatant. |
| 3+ | 10 | Several large clumps, clear supernatant. |
| 2+ | 8 | Many medium clumps, clear supernatant. |
| 1+ | 5 | Fine granular clumps, turbid reddish supernatant. |
| w (weak) | 3 | Visible only under microscope, turbid supernatant. |
| 0 | 0 | No clumps, clear reddish supernatant. |
| MF | — | Mixed field: agglutinated and free cells together. |
| H | — | Hemolysis: red supernatant, few or no intact cells. |

Mixed-Field
A mixed-field picture is a clue, not a result. It often means recent transfusion, fetomaternal hemorrhage, or a chimeric individual, and it always deserves follow-up.
Weak D and Partial D
Some red cells carry a quantitatively reduced or qualitatively altered D antigen. These cells may type negative or weakly positive at immediate spin. Two categories matter:
- Weak D — fewer copies of an otherwise normal D antigen. Most weak D types (specifically types 1, 2, 3, and 4.0) are safe to manage as D-positive for both transfusion and RhIg purposes [1,3].
- Partial D — parts of the D antigen are altered or missing. Partial D carriers can make anti-D against the parts they lack, so they are managed as D-negative for transfusion and RhIg.
Serologic tests cannot reliably tell weak D from partial D. The 2015 AABB/CAP Joint Statement and subsequent updates recommend RHD genotyping when a weak or discrepant D type is found, with priority for females of childbearing potential [1,3]. This is a meaningful change from older protocols that stopped at the weak D (formerly "Du") IAT and is the direction the field is moving [4,5].
Troubleshooting
Even careful technique runs into discrepant results. Read the control tube, then work through the most likely cause for what you see.
Weak or Questionable Agglutination (Weak Positive / Grade 1+)
Possible causes include a true weak D phenotype, deteriorated reagent, an over-dilute cell suspension, under-centrifugation, or vigorous resuspension that broke a fragile agglutinate.
What to do: prepare a fresh 3–5% suspension, check reagent expiry and storage, verify centrifuge calibration, and resuspend more gently. If the result is still weak in a context where it matters (donor, neonate, prenatal patient), reflex to RHD genotyping rather than relying on the older IAT-based weak D test alone [1,3].
False Positive (Reactive Control or Unexpected D Positive)
Most often this is autoagglutinin/cold antibody coating, rouleaux from abnormal plasma proteins (think multiple myeloma), bacterial contamination, an over-concentrated cell suspension, dirty glassware, or an old high-protein reagent system.
What to do: wash the red cells three to four more times in warm saline, examine microscopically (rouleaux looks like coin stacks; true agglutinates are irregular), add a drop of saline to disperse rouleaux, and if your reagent is a high-protein anti-D, switch to a monoclonal low-protein system that comes with its own diluent control.
False Negative (Missing Expected D Positive)
Causes include omission of reagent, a true weak D missed because no reflex testing was done, deteriorated anti-D, over-centrifugation that packed the cells too tightly, or in vivo antibody coating of the patient's red cells (as in autoimmune hemolytic anemia, where a positive direct antiglobulin test would point you to the explanation).
What to do: re-check every step, repeat with fresh reagent, perform the weak D test or RHD genotyping for any D-negative result that needs it, and run a DAT if in vivo antibody coating is suspected.
Discrepancies Between Current and Previous Results
Recent transfusion (mixed field), bone marrow or hematopoietic stem cell transplant (donor type takes over), clerical error, or rare antigen loss in some leukemias can all cause this.
What to do: verify identification first, review the patient's transfusion and transplant history, draw a fresh sample, and consider RHD genotyping when serology cannot resolve the discrepancy.
Tube Method in Context: How It Compares
| Method | Strengths | Limitations |
|---|---|---|
| Tube | Inexpensive, flexible, useful for teaching, easy to add washes | Subjective reading, low throughput, technique-dependent |
| Gel / column agglutination | Standardized, stable endpoints, easy to photograph | Higher reagent cost, less flexible for unusual workups |
| Solid phase | High throughput, automation-friendly | Capital cost, less suited for low-volume labs |
| RHD genotyping | Resolves weak D and partial D definitively | Slower turnaround, requires molecular lab, higher cost |
Quality Control and Good Practice
Daily QC, manufacturer-specified incubation and centrifugation, clean glassware, documented results, and trained staff are the basics that prevent most of the errors above. When the result is unclear, the best decisions come from a second method and a conversation with the supervisor or reference lab — not from a borderline read on a single tube.
Why This Matters Clinically
A misread Rh type does real harm. Transfusing RhD-positive cells to an RhD-negative woman of childbearing age can cause anti-D formation that affects every future RhD-positive pregnancy. Conversely, treating a weak D type 1 patient as RhD-negative needlessly uses scarce RhD-negative blood and exposes them to extra RhIg they do not need [1,3]. Accurate Rh typing, with the right reflex pathway, is straightforward immunology that protects patients across decades.
Frequently Asked Questions (FAQs)
What is Rh typing and why is it done?
Rh typing checks whether red blood cells carry the RhD antigen, and in extended panels, the C, c, E, and e antigens. It is a routine part of pretransfusion testing and prenatal care. The goal is to prevent transfusion reactions and hemolytic disease of the fetus and newborn.
What does Rh positive or Rh negative mean?
Rh positive means your red cells carry the RhD antigen on their surface. Rh negative means they do not. The distinction matters for transfusion compatibility and for pregnancy management, not for everyday health.
Why use the tube method when gel cards are available?
The tube method is inexpensive, flexible for unusual workups, and excellent for teaching the underlying immunology. Gel and solid-phase methods are now standard in high-throughput labs because they are more sensitive and easier to standardize. Most modern blood banks use a combination [4].
What is weak D, and why does it matter?
Weak D is a phenotype with reduced amounts of the RhD antigen. People with weak D types 1, 2, 3, or 4.0 can usually be managed as RhD-positive, while those with partial D should be managed as RhD-negative. Because serology cannot tell these apart reliably, current AABB/CAP guidance recommends RHD genotyping for any serologic weak D phenotype, especially in females of childbearing potential [1,3].
Can Rh-negative blood always be given to Rh-positive patients?
Yes, for the RhD antigen alone. RhD-negative red cells lack the D antigen and will not stimulate anti-D in the recipient. Full compatibility still requires ABO matching and screening for other clinically significant antibodies.
When is RhIg given to RhD-negative pregnant patients?
Standard practice is a dose at around 28 weeks gestation, within 72 hours after delivery if the baby is RhD-positive, and after sensitizing events such as miscarriage, amniocentesis, abdominal trauma, or external cephalic version. RhIg works by clearing fetal RhD-positive red cells before the maternal immune system can mount a response.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Sandler, S. G., Flegel, W. A., Westhoff, C. M., Denomme, G. A., Delaney, M., Keller, M. A., Johnson, S. T., Katz, L., Queenan, J. T., Vassallo, R. R., Simon, C. D., & College of American Pathologists Transfusion Medicine Resource Committee Work Group (2015). It's time to phase in RHD genotyping for patients with a serologic weak D phenotype. College of American Pathologists Transfusion Medicine Resource Committee Work Group. Transfusion, 55(3), 680–689. https://doi.org/10.1111/trf.12941
- Sandler, S. G., Roseff, S. D., Domen, R. E., Shaz, B., & Gottschall, J. L. (2014). Policies and procedures related to testing for weak D phenotypes and administration of Rh immune globulin: results and recommendations related to supplemental questions in the Comprehensive Transfusion Medicine survey of the College of American Pathologists. Archives of pathology & laboratory medicine, 138(5), 620–625. https://doi.org/10.5858/arpa.2013-0141-CP
- Flegel, W. A., Denomme, G. A., Queenan, J. T., Johnson, S. T., Keller, M. A., Westhoff, C. M., Katz, L. M., Delaney, M., Vassallo, R. R., Simon, C. D., & Sandler, S. G. (2020). It's time to phase out "serologic weak D phenotype" and resolve D types with RHD genotyping including weak D type 4. Transfusion, 60(4), 855–859. https://doi.org/10.1111/trf.15741
- Li, H. Y., & Guo, K. (2022). Blood Group Testing. Frontiers in medicine, 9, 827619. https://doi.org/10.3389/fmed.2022.827619
- Westhoff C. M. (2019). Blood group genotyping. Blood, 133(17), 1814–1820. https://doi.org/10.1182/blood-2018-11-833954
- Avent, N. D., & Reid, M. E. (2000). The Rh blood group system: a review. Blood, 95(2), 375–387. https://doi.org/10.1182/blood.V95.2.375
- Daniels G. (2013). Variants of RhD--current testing and clinical consequences. British journal of haematology, 161(4), 461–470. https://doi.org/10.1111/bjh.12275
- Cohn, C. S., Delaney, M., Johnson, S. T., & Katz, L. M. (Eds.). (2023). Technical Manual (21st ed.). Association for the Advancement of Blood & Biotherapies (AABB).