Key Takeaways
Cell surface markers are proteins, sugars, or lipids on the outside of a cell that act as identifiers, allowing scientists and clinicians to tell one cell type from another. CD34 is the most widely used marker of hematopoietic stem and progenitor cells, central to bone marrow transplantation, CAR-T manufacturing, and newly approved gene therapies for sickle cell disease and β-thalassemia [2,9].
- Each blood lineage has a signature combination of markers. T cells carry CD3 with CD4 or CD8; B cells carry CD19 and CD20; red cells carry CD235a (glycophorin A); platelets carry CD41 and CD61.
- The most primitive hematopoietic stem cells are usually CD34-positive and CD38-negative, but recent work shows a rare CD34-negative HSC population also exists in cord blood [6].
- Surface markers guide diagnosis (acute leukemia subtyping), prognosis, treatment selection, and tracking of measurable residual disease (MRD) after therapy [5,10].
Introduction to Hematopoiesis
Before talking about markers, it helps to know the cells they label.
Hematopoiesis is how the body makes blood. It starts with a single hematopoietic stem cell (HSC) in the bone marrow and ends with the red cells, white cells, and platelets that circulate in your blood.
HSCs have two superpowers. They can self-renew, meaning they divide to make more stem cells, and they can differentiate, meaning they can mature into specialized cell types. Because they can become several blood lineages but not unrelated tissues, they are called multipotent.
From the HSC, partially committed progenitor cells appear. The common lymphoid progenitor (CLP) gives rise to T cells, B cells, and natural killer cells. The common myeloid progenitor (CMP) splits into the granulocyte-macrophage progenitor (GMP), which makes neutrophils, eosinophils, basophils, monocytes, and dendritic cells, and the megakaryocyte-erythroid progenitor (MEP), which makes platelets and red cells.
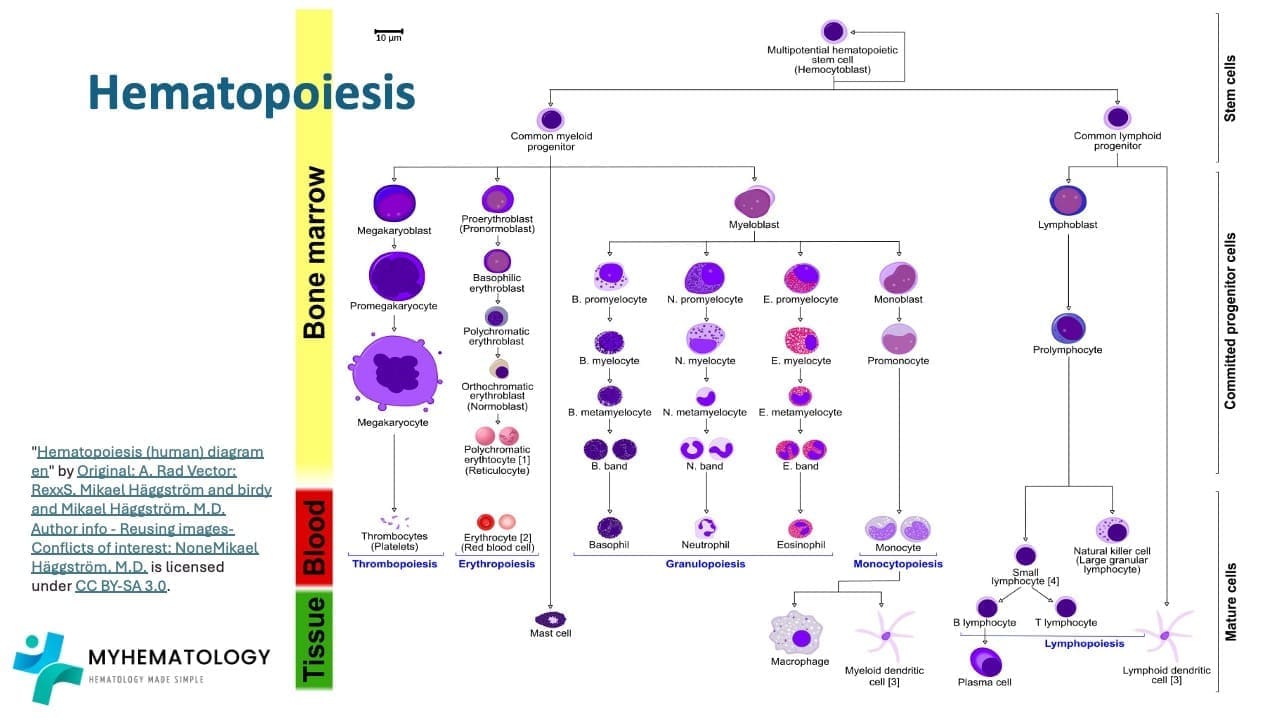
Each step of this journey is marked by a different combination of surface molecules. That is what makes surface markers so useful: they let us read where a cell is in its life story.
What are Cell Surface Markers?
A cell surface marker is a protein, carbohydrate, or lipid embedded in the outer membrane of a cell. Every cell type carries its own set, almost like an ID badge.
Antibodies that recognize the same surface molecule are grouped together and assigned a number. That number is called a cluster of differentiation, or CD. So when you see CD34, CD19, or CD45, the "CD" tells you which standardized group the antibodies belong to, and the number identifies the specific molecule.
Function of Cell Surface Markers
Markers are not just labels. They have real jobs.
They help with cell-to-cell communication. When a T cell recognizes an infected cell, it does so by reading surface markers. Receptors and ligands on neighboring cells dock together and trigger signals inside.
They help with adhesion and migration. Markers anchor cells to extracellular matrix and to neighboring cells, holding tissues together and guiding immune cells to the right destination.
They help regulate cell fate. Signaling through certain markers can push a stem cell to divide, mature, or stay quiet.
And in disease, they are often diagnostic clues. Tumor cells frequently express marker patterns that healthy cells do not, which is why immunophenotyping is central to cancer diagnosis.
CD34: The Stem Cell Marker
CD34 is a transmembrane sialomucin protein. It was identified in 1984 and quickly became the standard marker for hematopoietic stem and progenitor cells (HSPCs) [2].
CD34 is not exclusive to blood. It is also expressed on vascular endothelial progenitors, muscle satellite cells, corneal keratocytes, interstitial dendritic cells, and several cancer stem cell populations [1,9]. This broad distribution explains why "CD34-positive" is a useful but not stand-alone description.
What CD34 actually does
The function of CD34 is mainly adhesion. Its cytoplasmic tail helps stem cells stick to bone marrow stromal cells and to extracellular matrix [2]. It does not appear to drive proliferation directly.
A more interesting twist comes from lineage priming. CD34-positive HSCs can express low levels of myeloid genes, including CD13, CD33, and CD123, before they have actually committed to a lineage [1]. This finding overturned the older idea that primitive HSCs are completely "blank" and has implications for how acute myeloid leukemia (AML) is targeted therapeutically.
Are all stem cells CD34-positive?
Mostly, but not entirely. Research has identified a rare CD34-negative HSC population in human cord blood that sits at the very top of the stem cell hierarchy. Historically, these cells were ignored for transplantation because their limited homing capacity relative to CD34-positive HSCs made intravenous injection ineffective. However, recent breakthroughs have shown that treating these CD34-negative cells with an enzyme process called α1,3-fucosylation adds a crucial navigation carbohydrate (Sialyl Lewis X) to their surface [11]. This allows them to successfully migrate to the bone marrow, increasing their engraftment potential by roughly 7-fold and opening new doors for umbilical cord blood transplants [11].
Refining the CD34+ pool
Within CD34+CD38− cells, additional markers narrow down the most potent stem cells:
- CD90 (Thy-1) is positive on long-term HSCs.
- CD45RA is negative on HSCs and turns positive in lymphoid progenitors.
- CD49f is currently considered the most discriminating marker for single long-term repopulating HSCs [4].
The classical research panel is therefore Lin−CD34+CD38−CD45RA−CD90+CD49f+ [3,4].
CD34 in modern cell therapy
CD34 has moved well beyond bone marrow transplantation.
Stem cell mobilization. Granulocyte colony-stimulating factor (G-CSF) is the standard agent that pushes CD34+ cells from bone marrow into the blood for collection. In poor mobilizers, plerixafor (a CXCR4 antagonist) is added. Motixafortide, approved by the FDA in 2023, is a newer CXCR4 antagonist used in multiple myeloma.
Graft engineering. Devices like CliniMACS use immunomagnetic beads coated in anti-CD34 antibodies to isolate CD34+ cells from a graft, allowing T-cell depletion or selection of stem cells before infusion.
Gene therapy. This is arguably the most exciting frontier for CD34. Therapies for sickle cell disease (Casgevy and Lyfgenia) and β-thalassemia (Zynteglo) start by collecting a patient's own CD34+ HSPCs, editing them in the lab, and infusing them back [2]. As of July 2026, the FDA has expanded the use of Casgevy (the world's first ex vivo CRISPR/Cas9 therapy) to children as young as 2 years old [12]. This label expansion allows clinicians to intervene and correct the patient's stem cells before years of cumulative, irreversible organ damage take hold [12].
Therapeutic angiogenesis. CD34+ cells from bone marrow can promote new blood vessel formation in ischemic tissues, with applications under investigation for peripheral artery disease, cardiac ischemia, and stroke [9].
Flow Cytometry: How We Read Markers
Flow cytometry is the workhorse technique for analyzing cell surface markers.
How it works
Cells are tagged with antibodies that each carry a different fluorescent dye. The cells are then suspended in fluid and pushed through a narrow channel, one cell at a time, past one or more lasers. When a tagged cell crosses the laser, each dye lights up at a specific wavelength. Detectors record which dyes are present and how strongly they shine, giving a multi-color readout for every cell.
Multiparametric immunophenotyping
Modern instruments can measure a dozen markers or more on the same cell. This is called multiparametric immunophenotyping, and it is far more powerful than checking one marker at a time. Many surface molecules are shared across cell types. CD34 alone does not tell you whether you are looking at a leukemic blast or a healthy stem cell. CD34 combined with CD38, CD45, HLA-DR, MPO, and lineage markers does.
FACS
Fluorescence-Activated Cell Sorting (FACS) goes one step further by physically separating cells based on their marker profile. Researchers use FACS to purify rare populations, like single CD34+CD38−CD90+CD49f+ HSCs, for transplantation studies or single-cell sequencing.
Beyond flow cytometry
Immunohistochemistry uses antibodies on tissue sections, which lets pathologists see where a marker sits within the architecture of a lymph node or bone marrow trephine. Fluorescence microscopy offers high-resolution images of marker distribution on individual cells. The two complement flow cytometry rather than replacing it.
Clinical Applications of Cell Surface Markers

Surface markers do real work in clinical hematology every day.
Diagnosing and classifying leukemias and lymphomas
In acute leukemia, the marker profile decides treatment. B-cell ALL typically expresses CD19, cytoplasmic CD79a, CD10, CD22, TdT, and often CD34. T-cell ALL expresses cytoplasmic CD3, CD7, TdT, and is often CD34-negative. AML expresses MPO, CD13, CD33, CD117, with CD34 and HLA-DR usually positive (acute promyelocytic leukemia, the old M3, is the classic exception, being HLA-DR negative) [10].
The WHO 5th edition (2022) and the International Consensus Classification (2022) now define acute leukemias by integrating morphology, immunophenotype, and genetics rather than the older FAB system alone [7,8]. The FAB subtypes (M1 to M7) still appear in textbooks but increasingly take a back seat to genetic categories.
Monitoring measurable residual disease (MRD)
After chemotherapy, many patients still harbor a small number of leukemic cells that drive relapse. The field now prefers measurable residual disease to "minimal residual disease" because newer methods detect cells at levels of 10⁻⁵ to 10⁻⁶ (one leukemic cell among 100,000 to a million normal ones). Standardized panels such as the EuroFlow MRD panel use the leukemia-associated immunophenotype (LAIP) strategy and the different-from-normal (DfN) strategy to spot these rare cells [5].
Stem cell transplantation
CD34 enumeration on flow cytometry is the standard way to dose a stem cell graft. A typical adult autologous transplant aims for at least 2 to 5 × 10⁶ CD34+ cells per kilogram.
CAR-T therapy
Chimeric Antigen Receptor T-cell (CAR-T) therapy engineers a patient's T cells to recognize a tumor surface marker. As of 2026, the FDA has approved 7 autologous CAR-T products targeting CD19 for B-cell malignancies and BCMA for multiple myeloma. Because cancers can sometimes "hide" by downregulating these markers (antigen escape), recent clinical trials have focused heavily on dual-targeting CAR-Ts (e.g., hitting both CD19 and CD22 simultaneously), which have demonstrated high complete response rates in relapsed leukemia and lymphoma [13]. Furthermore, the field is actively researching allogeneic ("off-the-shelf") CAR-T therapies to bypass the 2- to 4-week manufacturing wait time required for current autologous products.
Targeted antibody therapies
Monoclonal antibodies use surface markers as docking stations for cytotoxic payloads or immune effector function. Examples include rituximab (anti-CD20) for B-cell lymphomas, daratumumab (anti-CD38) for myeloma, and gemtuzumab ozogamicin (anti-CD33) for AML.
Marker Profiles of Hematopoietic Cells
The table below summarizes the classical surface marker profiles students are expected to recognize. Marker combinations differ slightly between research papers and clinical labs; the panels here represent widely accepted consensus sets.
Differential Cell Surface Markers of Leukemias
| Cell Type | Classical Marker Profile |
|---|---|
| Stem & Progenitor Cells | |
| Hematopoietic Stem Cell (HSC) | Lin−CD34+CD38−CD45RA−CD90+CD49f+ [3, 4] |
| Common Lymphoid Progenitor (CLP) | Lin−CD34+CD38−/lo CD45RA+ CD90− |
| Common Myeloid Progenitor (CMP) | CD34+CD38+CD123med CD135+ CD45RA− |
| Granulocyte-Macrophage Progenitor (GMP) | CD34+CD38+CD123+CD135+CD45RA+ |
| Megakaryocyte-Erythroid Progenitor (MEP) | CD34+CD38+CD123−CD135−CD45RA− |
| Mature & Peripheral Cells | |
| Erythroid (red cell lineage) | CD71+ glycophorin A (CD235a)+ |
| T cell | CD3+ with CD4 or CD8 |
| B cell (mature) | CD19+ CD20+ |
| Natural killer cell | CD56+ CD16+ (peripheral blood) |
| Monocyte (classical) | CD14+ CD16− |
| Neutrophil | CD11b+ CD16+ |
| Platelet | CD41+ CD61+ CD42b+ |
Marker Profiles in Acute Leukemia
The table below highlights the high-yield panels for distinguishing AML, B-ALL, and T-ALL. Adapted from Li (2022) [10].
| Leukemia | Lineage-Defining Markers | Maturation Markers | Immaturity Markers |
|---|---|---|---|
| AML | MPO, CD117 | CD13, CD33, CD15, CD14/CD64 (monocytic) | CD34, HLA-DR (APL/M3 is HLA-DR negative) |
| B-ALL | cytoplasmic CD79a, strong CD19 | CD10, CD22, CD24, CD20 (later) | TdT, CD34, HLA-DR |
| T-ALL | cytoplasmic CD3, CD7 | CD5, CD2, CD4, CD8, CD1a (cortical) | TdT (CD34 often negative) |
A few rules to remember:
- MPO defines myeloid; TdT defines immature lymphoid. Surface CD3 is often absent in immature T cells, so cytoplasmic CD3 (cCD3) is the lineage-defining marker for T-ALL.
- Aberrant marker expression is common. B-ALL blasts can express CD13 or CD33, and AML blasts can occasionally express lymphoid markers. This does not automatically mean mixed-phenotype acute leukemia (MPAL) as a strict diagnostic criteria must be met.
- CD10 (CALLA) marks the common B-ALL subtype, which carries a more favorable pediatric prognosis than CD10-negative pro-B ALL.
Frequently Asked Questions (FAQs)
What is CD34 and why is it important?
CD34 is a protein on the surface of hematopoietic stem and progenitor cells. It is the standard marker used to identify, count, and isolate stem cells for bone marrow transplantation, gene therapy, and CAR-T cell production. CD34 is also found on endothelial progenitors, muscle satellite cells, and some cancer stem cells, so it is not exclusive to blood.
What is the difference between CD34 and CD38?
CD34 marks early hematopoietic stem and progenitor cells. CD38 turns on as those cells start to mature and commit to a lineage. The most primitive, self-renewing stem cells are therefore typically CD34-positive and CD38-negative (CD34+CD38−).
How is flow cytometry used to diagnose leukemia?
Flow cytometry uses panels of fluorescent antibodies that bind to surface and intracellular markers. The pattern of markers for example MPO with CD13/CD33 for myeloid leukemia, or CD19, CD10, and TdT for B-cell ALL tells the laboratory which lineage the leukemic cells belong to and which subtype is involved. This guides treatment.
Are all hematopoietic stem cells CD34-positive?
Most are, but research published in the last decade shows that a small population of the most primitive cord-blood HSCs is actually CD34-negative and can be identified using markers like CD133 and GPI-80. So CD34 captures the majority of clinically relevant stem cells but not the entire stem cell pool.
What does "Lineage Negative" mean in flow cytometry?
Lineage Negative (Lin−) means a cell does not carry any of the markers that define mature blood cells, such as CD3 (T cells), CD19 (B cells), CD14 (monocytes), or CD235a (red cells). Researchers exclude lineage-positive cells so they can study rare stem and progenitor populations.
How is CD34 used in modern cell therapy beyond transplantation?
Newly approved gene therapies for sickle cell disease and β-thalassemia, such as Casgevy (exagamglogene autotemcel) and Lyfgenia (lovotibeglogene autotemcel), are made by collecting a patient's own CD34+ cells, editing them in the laboratory, and infusing them back. CD34 selection is also used to engineer transplant grafts and to mobilize stem cells with agents like plerixafor and motixafortide.
Glossary of Related Medical Terms
- Antigen — a molecule, usually a protein or sugar on a cell surface, that the immune system can recognize and that an antibody can bind.
- Aberrant expression — when a leukemic cell shows surface markers that are not normally found together in healthy cells of the same lineage.
- Blast cell — an early, immature cell in the bone marrow. Increased blasts in blood are a hallmark of acute leukemia.
- CD34 — a transmembrane protein widely used to identify hematopoietic stem and progenitor cells; also expressed on several non-blood cells.
- Cluster of Differentiation (CD) — a numbered naming system for cell-surface molecules.
- Engraftment — when transplanted stem cells settle in the recipient's bone marrow and begin producing new blood cells.
- FACS (Fluorescence-Activated Cell Sorting) — a flow cytometry technique that physically separates cells based on the fluorescent markers they carry.
- Flow cytometry — a laser-based method that measures the size, shape, and surface molecules of single cells.
- Hematopoiesis — the process by which the body makes blood cells, mostly in the bone marrow.
- Immunophenotyping — using antibodies against surface markers to identify and classify cells.
- Lineage Negative (Lin−) — a cell that lacks the surface markers of mature blood cells.
- Measurable Residual Disease (MRD) — small numbers of cancer cells that remain after treatment, detectable only with sensitive methods.
- MPO (Myeloperoxidase) — an enzyme inside myeloid cells; its presence confirms myeloid lineage in acute leukemia.
- Multipotent — able to develop into several, but not all, cell types within a related family.
- Progenitor cell — a partly committed cell that has lost full self-renewal but can still divide and mature into a limited range of cell types.
- Self-renewal — the ability of a stem cell to divide and produce more stem cells without losing its identity.
- TdT (Terminal deoxynucleotidyl transferase) — a nuclear enzyme found in immature lymphoid cells; a hallmark of lymphoblasts in ALL.
Disclaimer: This article is intended for educational and informational purposes only. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Sidney, L. E., Branch, M. J., Dunphy, S. E., Dua, H. S., & Hopkinson, A. (2014). Concise review: evidence for CD34 as a common marker for diverse progenitors. Stem cells (Dayton, Ohio), 32(6), 1380–1389. https://doi.org/10.1002/stem.1661
- Radu, P., Zurzu, M., Paic, V., Bratucu, M., Garofil, D., Tigora, A., Georgescu, V., Prunoiu, V., Pasnicu, C., Popa, F., Surlin, P., Surlin, V., & Strambu, V. (2023). CD34-Structure, Functions and Relationship with Cancer Stem Cells. Medicina (Kaunas, Lithuania), 59(5), 938. https://doi.org/10.3390/medicina59050938
- Majeti, R., Park, C. Y., & Weissman, I. L. (2007). Identification of a hierarchy of multipotent hematopoietic progenitors in human cord blood. Cell stem cell, 1(6), 635–645. https://doi.org/10.1016/j.stem.2007.10.001
- Notta, F., Doulatov, S., Laurenti, E., Poeppl, A., Jurisica, I., & Dick, J. E. (2011). Isolation of single human hematopoietic stem cells capable of long-term multilineage engraftment. Science (New York, N.Y.), 333(6039), 218–221. https://doi.org/10.1126/science.1201219
- Weeda, V., Mestrum, S. G. C., & Leers, M. P. G. (2022). Flow Cytometric Identification of Hematopoietic and Leukemic Blast Cells for Tailored Clinical Follow-Up of Acute Myeloid Leukemia. International journal of molecular sciences, 23(18), 10529. https://doi.org/10.3390/ijms231810529
- Rix, B., Maduro, A. H., Bridge, K. S., & Grey, W. (2022). Markers for human haematopoietic stem cells: The disconnect between an identification marker and its function. Frontiers in physiology, 13, 1009160. https://doi.org/10.3389/fphys.2022.1009160
- Khoury, J. D., Solary, E., Abla, O., Akkari, Y., Alaggio, R., Apperley, J. F., Bejar, R., Berti, E., Busque, L., Chan, J. K. C., Chen, W., Chen, X., Chng, W. J., Choi, J. K., Colmenero, I., Coupland, S. E., Cross, N. C. P., De Jong, D., Elghetany, M. T., Takahashi, E., … Hochhaus, A. (2022). The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia, 36(7), 1703–1719. https://doi.org/10.1038/s41375-022-01613-1
- Arber, D. A., Orazi, A., Hasserjian, R. P., Borowitz, M. J., Calvo, K. R., Kvasnicka, H. M., Wang, S. A., Bagg, A., Barbui, T., Branford, S., Bueso-Ramos, C. E., Cortes, J. E., Dal Cin, P., DiNardo, C. D., Dombret, H., Duncavage, E. J., Ebert, B. L., Estey, E. H., Facchetti, F., Foucar, K., … Tefferi, A. (2022). International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: integrating morphologic, clinical, and genomic data. Blood, 140(11), 1200–1228. https://doi.org/10.1182/blood.2022015850
- Fujita, Y., & Kawamoto, A. (2022). Therapeutic Angiogenesis Using Autologous CD34-Positive Cells for Vascular Diseases. Annals of vascular diseases, 15(4), 241–252. https://doi.org/10.3400/avd.ra.22-00086
- Li, W. (2022). Flow Cytometry in the Diagnosis of Leukemias. In W. Li (Ed.), Leukemia. Exon Publications. https://doi.org/10.36255/exon-publications-leukemia-flow-cytometry
- Al-Amoodi, A. S., Kai, J., Li, Y., Malki, J. S., Alghamdi, A., Al-Ghuneim, A., Saera-Vila, A., Habuchi, S., & Merzaban, J. S. (2024). α1,3-fucosylation treatment improves cord blood CD34 negative hematopoietic stem cell navigation. iScience, 27(2), 108882. https://doi.org/10.1016/j.isci.2024.108882
- Vertex Pharmaceuticals. (2026). FDA Expands Casgevy Approval to Children as Young as 2 Years With Sickle Cell Disease or Transfusion-Dependent β-Thalassemia. Pharmacy Times / BioPharm International.
- Feng, S., Kong, R., Xiao, L., & Zhou, X. (2026). Dual-target CAR-T cell therapy: latest updates from the 2025 ASH annual meeting. Experimental hematology & oncology, 15(1), 50. https://doi.org/10.1186/s40164-026-00790-4