Procedure At a Glance
The sickle cell disease test (dithionite solubility test) is a fast, low-cost screening method that detects hemoglobin S (HbS) by turning cloudy when deoxygenated HbS forms polymers.
- Prepare fresh dithionite reagent (or reconstitute a commercial kit).
- Mix 2.0 mL reagent with 20 µL anticoagulated blood in a labeled tube.
- Stand for 5–10 minutes at room temperature.
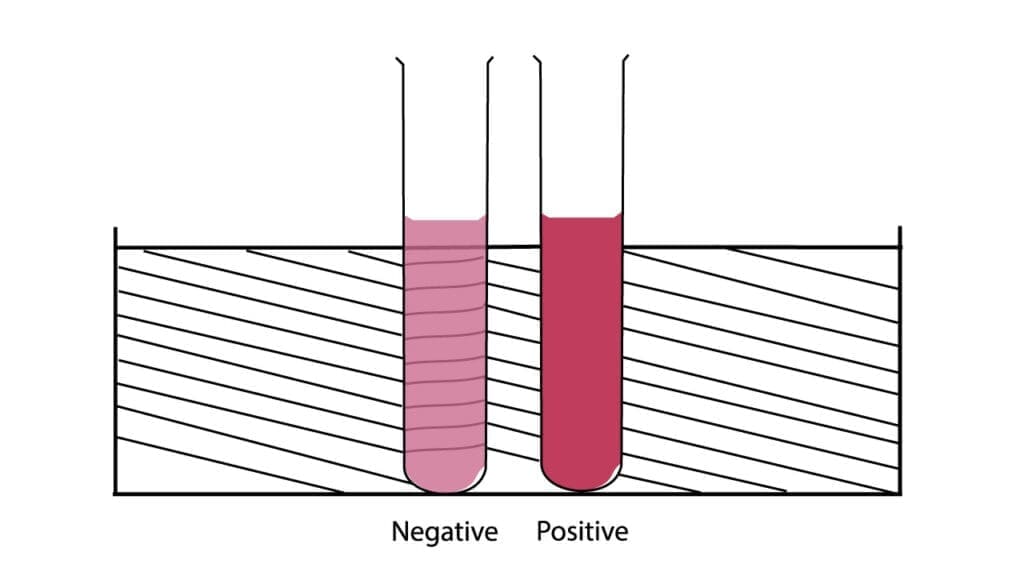
- Read macroscopically (visually): clear = negative, cloudy = positive. Note: Do not view under a microscope, as the red blood cells are destroyed during this specific test [11].
- Confirm any positive or unclear result with HPLC or hemoglobin electrophoresis.
What is the Sickle Cell Disease Test?
The sickle cell disease test, also known as the dithionite solubility test or Hb S sickling test, is a screening method used to detect hemoglobin S (HbS) in blood. It is fast, cheap, and well-suited to laboratories that don't have access to high-end equipment. It is, however, only a screening test. Any positive result needs confirmation [10].
Understanding Sickle Cell Disease
Sickle cell disease (SCD) is an inherited disorder of red blood cells. It is passed on recessively, meaning a child develops SCD only when they inherit one mutated β-globin gene from each parent. SCD is not contagious [8].
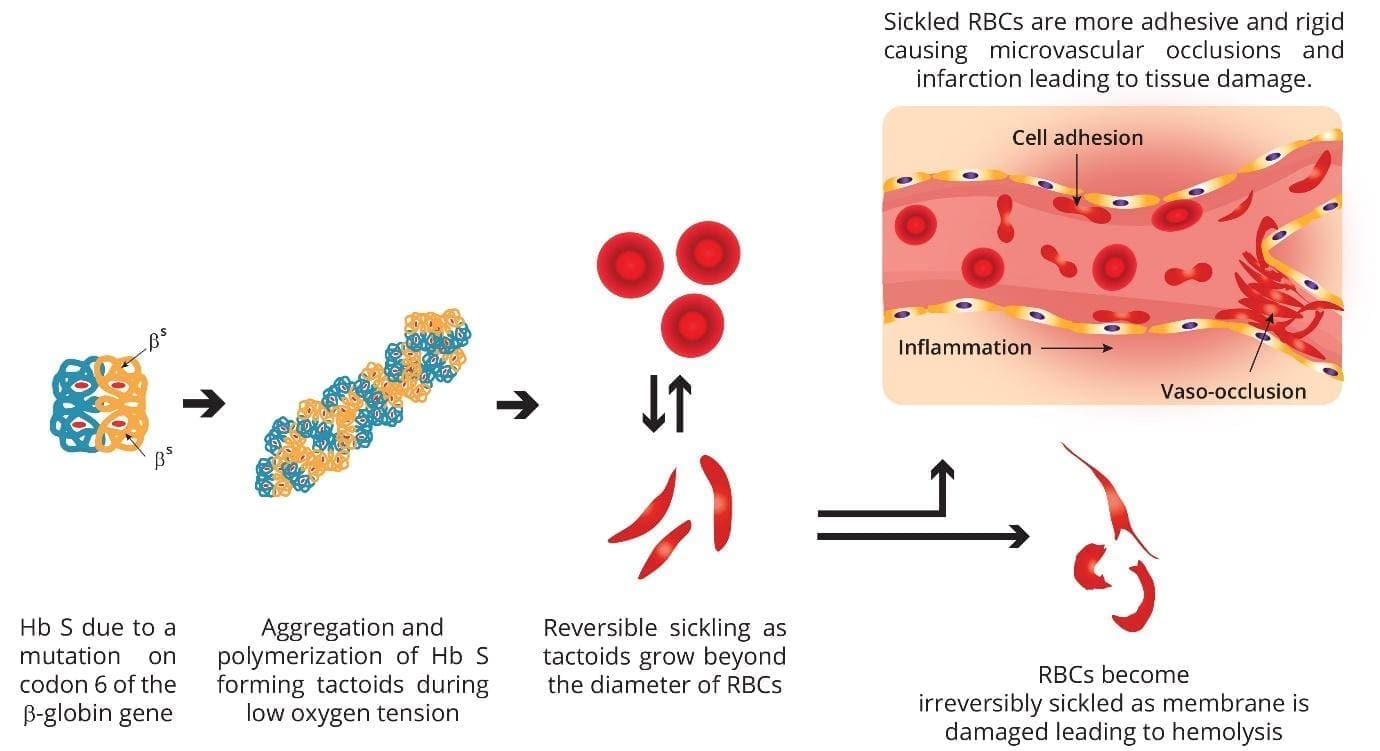
The disease starts with a single change at codon 6 of the β-globin gene: the amino acid glutamic acid is replaced by valine. This swap produces an abnormal hemoglobin called HbS. When HbS gives up its oxygen, its molecules clump together (polymerize) into long, rigid fibers. The red blood cell loses its smooth, doughnut-like shape and becomes a stiff crescent — the "sickle."
Why Sickled Cells Cause Problems
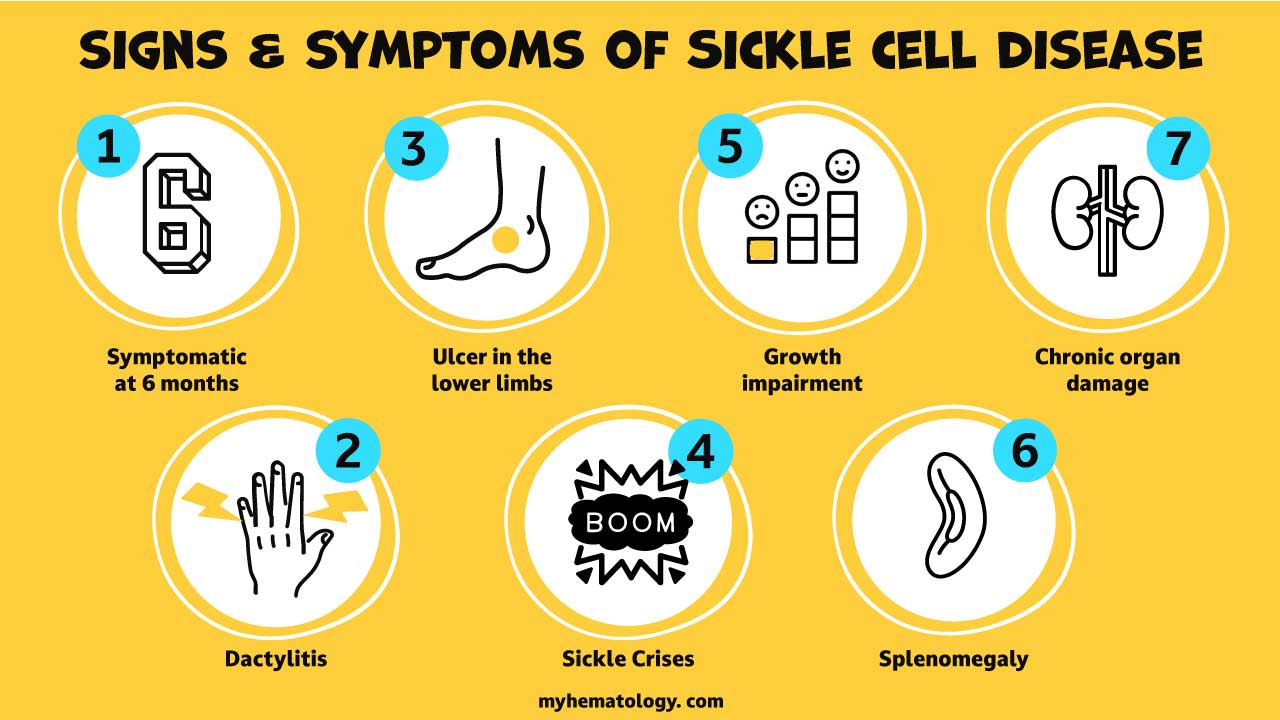
- Short lifespan: Sickled red cells last 10–20 days, compared with 120 days for normal cells. The result is chronic anemia (low red cell count).
- Vessel blockage: Their stiff, sticky surface lets them lodge in small blood vessels. This blockage, called vaso-occlusion, starves tissues of oxygen.
- Complications: Pain crises, stroke, organ damage (spleen, kidneys, lungs, brain), acute chest syndrome, increased infection risk, and delayed growth in children [8,9].
Sickle Cell Trait vs. Sickle Cell Disease
- Sickle cell trait (HbAS): one normal gene, one HbS gene. Usually symptom-free, but can pass HbS to children.
- Sickle cell disease (HbSS, HbSC, HbSβ-thalassemia): two abnormal genes, with the symptoms described above.
Knowing which version someone has is essential, and that's why a positive screening test always needs confirmation.
Principle of the Test
The principle is simple but elegant. Normal hemoglobin (HbA) stays dissolved whether oxygenated or not. HbS is different: when deoxygenated, it loses solubility and polymerizes [1].
The test exploits this. Sodium dithionite is a strong reducing agent that strips oxygen off hemoglobin. Saponin is a detergent that breaks open the red blood cells, releasing their hemoglobin. Once HbS molecules are deoxygenated and free in solution, they form long fibers that scatter light. The solution looks cloudy. HbA, treated the same way, stays clear. That contrast is the readout [1,10].
Because the saponin completely lyses (destroys) the red blood cells to release the hemoglobin, no intact cells remain to be viewed. Therefore, the dithionite test is strictly a macroscopic, visual test [11].
Materials
- Anticoagulated peripheral blood (EDTA)
- Sodium dithionite (Na₂S₂O₄) in concentrated phosphate buffer, pH 6.8
- Saponin or another red-cell lysing agent
- Pasteur pipette, test tubes, microscope slides, coverslips
- Petroleum jelly–paraffin wax or DePeX for sealing
- A reading stand or card with printed lines (helps judge turbidity)
Practical tips
Commercial kits are widely available and come with pre-measured reagents that just need mixing before use. They also include a reference card so you can compare turbidity reliably.
Protocol
- Prepare or reconstitute the dithionite reagent immediately before use. Sodium dithionite is unstable in solution.
- Label a clean, dry test tube.
- Pipette 2.0 mL of reagent into the tube.
- Add 20 µL of anticoagulated blood. Avoid air bubbles.
- Mix thoroughly by inverting or vortexing.
- Let the mixture stand at room temperature for 5–10 minutes. Note that for borderline samples, laboratories may incubate the tube for up to 15–20 minutes to allow for slower polymerization, depending on the manufacturer's specific instructions [12].
- Read the tube against the reference card.
Microscopic Sickling Test
If microscopic confirmation of sickled cells is desired, a separate procedure known as the sodium metabisulfite slide test must be used. This test utilizes a reducing agent without a lysing agent like saponin. Because the cells are not lysed, they remain intact, allowing the technician to observe their physical deformation into sickle shapes under a microscope [1,11].
Interpretation
The test has a macroscopic and a microscopic readout, and you should always check both.
Negative Result
No significant HbS detected. Solution is clear and transparent. You can read fine print or lines through it.
Positive Result
HbS is present — either trait or disease. Solution is turbid (cloudy or opaque). Lines behind the tube are obscured. Stronger turbidity often suggests more HbS [10].
A positive result does not distinguish HbAS from HbSS or HbSC. That's the job of confirmatory testing.
Indeterminate or Weak Positive Result
Sometimes the tube is faintly hazy and only a few sickled cells appear. Don't call this negative. Common reasons include low HbS concentration, severe anemia, recent transfusion, high HbF, or aged reagent. Repeat the test with fresh reagent, then refer for confirmatory testing regardless.
Factors Affecting SCD Test Results
Like any laboratory test, this one is fallible. Knowing why helps you interpret tricky cases.
Causes of False Negatives
- High fetal hemoglobin (HbF): The main reason newborns and infants under 6 months can't be reliably tested with this method. HbF blocks HbS polymerization [3].
- Recent blood transfusion: Transfused HbA dilutes HbS below the test's detection threshold.
- Severe anemia: If the patient's hemoglobin is very low (typically <8 g/dL), there may not be enough HbS to produce visible turbidity. To prevent a false negative, laboratories standardize the hemoglobin concentration by removing a portion of the patient's plasma before adding the red blood cells to the testing reagent [1,12].
- Low HbS concentration: The solubility test generally requires a minimum concentration of 10% to 20% HbS to precipitate and show visible turbidity. Extreme dilution, such as following a recent mass transfusion, can easily drop HbS levels below this threshold, causing the test to fail [12].
- Aged sample or aged reagent: Both reduce reactivity. Sodium dithionite is notoriously unstable; some newer paper-based kits use sodium metabisulfite instead for longer shelf life [6].
- Technical errors: wrong volumes, poor mixing, inadequate incubation.
Causes of False Positives
- Very high red cell counts (polycythemia) or extreme leukocytosis or thrombocytosis — too many particles in the tube create non-specific cloudiness.
- High plasma proteins or lipids (e.g., paraproteins in multiple myeloma, severe hyperlipidemia).
- Other rare sickling hemoglobin variants (HbC-Harlem, HbC-Georgetown).
- Numerous Heinz bodies in the red cells.
- Technical errors: too much blood, contaminated reagent or glassware.
This is why every positive or ambiguous result must go to a confirmatory test [3,10].
Limitations of the Dithionite Solubility Test
- It is a screening test, not a diagnostic one. A positive result only flags HbS; it cannot diagnose SCD on its own.
- It cannot tell trait from disease. HbAS and HbSS both turn the tube cloudy.
- It is qualitative. It does not measure the percentage of HbS in the sample.
- Interpretation is subjective. Reading turbidity and microscopic morphology depends on the technician's experience.
- It is unreliable in newborns and recently transfused patients.
Confirmatory and Alternative Tests
When the sickle cell disease test is positive, indeterminate, or clinically suspicious, the next step is a method that can identify and quantify hemoglobin variants.
- Hemoglobin electrophoresis separates hemoglobins by electrical charge on a gel.
- High-Performance Liquid Chromatography (HPLC) automates separation by chemical properties and quantifies each variant. It is the workhorse of confirmatory and newborn screening labs [3].
- Isoelectric focusing (IEF) is the other main newborn-screening method in many countries [3].
- Genetic (DNA) testing identifies the HBB gene mutation directly. Useful for ambiguous compound heterozygotes and prenatal diagnosis.
- Point-of-care immunoassays such as HemoTypeSC and SickleSCAN use monoclonal antibodies on a lateral-flow strip and can give a result in minutes for under $2 per test. In multi-center field studies, HemoTypeSC has shown sensitivity of 93–100% and specificity above 99%, including in newborns [5,7]. These are increasingly used where HPLC and electrophoresis aren't available.
A simple comparison helps put the methods in context:
| Method | Speed | Cost | Quantifies HbS? | Use in Newborns? |
|---|---|---|---|---|
| Dithionite Solubility | 10 min | Low | No | No HbF interferes |
| Hb Electrophoresis | Hours | Moderate | Semi-quantitative | Yes |
| HPLCPreferred | ~10 min/sample | Higher | Yes | Yes |
| IEFPreferred | Hours (batch) | Moderate | Semi-quantitative | Yes |
| POC Immunoassay | Minutes | Very low | No | Yes |
| DNA Testing | Days | Highest | N/A | Yes |
Clinical Significance
SCD affects an estimated 100,000 people in the United States and around 300,000 babies are born with SCD globally each year, the majority in sub-Saharan Africa [8]. Catching it early changes lives.
Preventing infection. Young children with SCD are highly vulnerable to bacterial infections such as pneumococcal disease. Daily prophylactic penicillin and a full vaccination schedule (pneumococcal, meningococcal, Hib, influenza) dramatically lower this risk [9].
Preventing stroke. Children with SCD undergo regular transcranial Doppler ultrasound screening. Those at high risk benefit from chronic transfusion or hydroxyurea.
Disease-modifying therapy. Standard-of-care medications include hydroxyurea (boosts HbF), L-glutamine, and crizanlizumab (reduces vaso-occlusive crises). Note that voxelotor was withdrawn from the market in September 2024 after post-marketing data raised safety concerns.
Curative options. Allogeneic stem cell transplantation has long been the only cure. Since December 2023, two gene therapies are FDA-approved for patients aged 12 and older with recurrent pain crises [4]:
- Casgevy (exagamglogene autotemcel) — the first CRISPR/Cas9 gene-editing therapy approved for any disease, working by reactivating fetal hemoglobin.
- Lyfgenia (lovotibeglogene autotemcel) — uses a lentiviral vector to add an anti-sickling β-globin gene to the patient's own stem cells.
Access remains limited and the therapies are expensive, but they represent a genuine shift in what's possible.
Family planning and genetic counseling. A confirmed result lets families be screened, understand inheritance, and make informed reproductive decisions.
Frequently Asked Questions (FAQs)
What is the sickle cell disease test, in plain terms?
The sickle cell disease test (also called the dithionite solubility test or Hb S sickling test) is a quick, inexpensive screening test that checks whether your blood contains an abnormal form of hemoglobin called HbS. It works by removing oxygen from the hemoglobin and watching whether the solution turns cloudy. Cloudy means HbS is likely present.
Does a positive sickle cell disease test mean I have sickle cell disease?
Not necessarily. A positive result simply means HbS is present. It does not tell you whether you have sickle cell trait (one mutated gene, usually no symptoms) or sickle cell disease (two mutated genes, with symptoms). A confirmatory test such as hemoglobin electrophoresis or HPLC is needed to know which.
Why isn't the dithionite test used on newborns?
Newborns have high levels of fetal hemoglobin (HbF), which blocks HbS from polymerizing. The test can therefore look falsely negative in babies under about 6 months old. Newborn screening programs use isoelectric focusing (IEF) or HPLC on a dried blood spot instead.
What treatments are available for sickle cell disease today?
Standard treatments include hydroxyurea, vaccinations, daily prophylactic penicillin in young children, blood transfusions, and pain management. Newer options include L-glutamine and crizanlizumab. In December 2023, the FDA approved two gene therapies (Casgevy (a CRISPR-based therapy) and Lyfgenia) for patients aged 12 and older with recurrent pain crises [4].
Is sickle cell disease contagious?
No. Sickle cell disease is inherited. A child develops SCD only when they inherit a mutated gene from each parent. You cannot catch it from someone.
Glossary of Related Medical Terms
- Anticoagulant — a substance added to a blood sample tube (commonly EDTA) to stop it from clotting, so it stays liquid for testing.
- β-globin — one of the two protein chains that make up adult hemoglobin. The mutation that causes sickle cell disease is in the gene for this chain.
- Codon 6 — the sixth three-letter "word" in the β-globin gene's instruction sequence. The sickle mutation swaps one letter here.
- Deoxygenated — when hemoglobin has released its oxygen. HbS only sickles in this state.
- Hemoglobin (Hb) — the iron-containing protein in red blood cells that carries oxygen.
- Hemoglobin S (HbS) — the abnormal hemoglobin produced in people who carry the sickle cell mutation.
- Hemoglobin F (HbF) — fetal hemoglobin. Predominant before birth and in early infancy; protective against sickling.
- Heterozygous — having two different versions of a gene (e.g., HbAS = sickle cell trait).
- Homozygous — having two identical versions of a gene (e.g., HbSS = sickle cell anemia).
- Hemolysis — the breaking open of red blood cells, releasing their contents.
- Polymerization — molecules linking up into long chains. Deoxygenated HbS does this, deforming the cell.
- Saponin — a plant-derived detergent that punctures red blood cell membranes.
- Sodium dithionite (Na₂S₂O₄) — a strong reducing agent. Pulls oxygen off hemoglobin in the test.
- Turbidity — visible cloudiness of a solution caused by suspended particles scattering light.
- Vaso-occlusion — blockage of small blood vessels. The main cause of pain crises in SCD.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Bain BJ, Bates I, Laffan MA. Dacie and Lewis Practical Haematology: Expert Consult: Online and Print (Elsevier) 12th Edition. 2016.
- Nalbandian, R. M., Henry, R. L., Lusher, J. M., Camp, F. R., Jr., & Conte, N. F. (1971). Dithionite tube test — A rapid, inexpensive technique for the detection of hemoglobin S and non-S sickling hemoglobin. Clinical Chemistry, 17(10), 1028–1032.
- Frömmel C. (2018). Newborn Screening for Sickle Cell Disease and Other Hemoglobinopathies: A Short Review on Classical Laboratory Methods-Isoelectric Focusing, HPLC, and Capillary Electrophoresis. International journal of neonatal screening, 4(4), 39. https://doi.org/10.3390/ijns4040039
- Frangoul, H., Locatelli, F., Sharma, A., Bhatia, M., Mapara, M., Molinari, L., Wall, D., Liem, R. I., Telfer, P., Shah, A. J., Cavazzana, M., Corbacioglu, S., Rondelli, D., Meisel, R., Dedeken, L., Lobitz, S., de Montalembert, M., Steinberg, M. H., Walters, M. C., Eckrich, M. J., … CLIMB SCD-121 Study Group (2024). Exagamglogene Autotemcel for Severe Sickle Cell Disease. The New England journal of medicine, 390(18), 1649–1662. https://doi.org/10.1056/NEJMoa2309676
- Steele, C., Sinski, A., Asibey, J., Hardy-Dessources, M. D., Elana, G., Brennan, C., Odame, I., Hoppe, C., Geisberg, M., Serrao, E., & Quinn, C. T. (2019). Point-of-care screening for sickle cell disease in low-resource settings: A multi-center evaluation of HemoTypeSC, a novel rapid test. American journal of hematology, 94(1), 39–45. https://doi.org/10.1002/ajh.25305
- Torabian, K., Lezzar, D., Piety, N. Z., George, A., & Shevkoplyas, S. S. (2017). Substituting Sodium Hydrosulfite with Sodium Metabisulfite Improves Long-Term Stability of a Distributable Paper-Based Test Kit for Point-of-Care Screening for Sickle Cell Anemia. Biosensors, 7(3), 39. https://doi.org/10.3390/bios7030039
- Nnodu, O., Isa, H., Nwegbu, M., Ohiaeri, C., Adegoke, S., Chianumba, R., Ugwu, N., Brown, B., Olaniyi, J., Okocha, E., Lawson, J., Hassan, A. A., Diaku-Akinwumi, I., Madu, A., Ezenwosu, O., Tanko, Y., Kangiwa, U., Girei, A., Israel-Aina, Y., Ladu, A., … Adekile, A. (2019). HemoTypeSC, a low-cost point-of-care testing device for sickle cell disease: Promises and challenges. Blood cells, molecules & diseases, 78, 22–28. https://doi.org/10.1016/j.bcmd.2019.01.007
- Williams, T. N., & Thein, S. L. (2018). Sickle Cell Anemia and Its Phenotypes. Annual review of genomics and human genetics, 19, 113–147. https://doi.org/10.1146/annurev-genom-083117-021320
- Kavanagh, P. L., Fasipe, T. A., & Wun, T. (2022). Sickle Cell Disease: A Review. JAMA, 328(1), 57–68. https://doi.org/10.1001/jama.2022.10233
- Arishi, W. A., Alhadrami, H. A., & Zourob, M. (2021). Techniques for the Detection of Sickle Cell Disease: A Review. Micromachines, 12(5), 519. https://doi.org/10.3390/mi12050519
- McPherson, R. A., & Pincus, M. R. (2021). Henry's Clinical Diagnosis and Management by Laboratory Methods (24th ed.). Elsevier.
- Keohane, E. M., Preston, M. M., Mirza, K. M., & Walenga, J. M. (2024). Rodak's Hematology: Clinical Principles and Applications (7th ed.). Elsevier.