Procedure-at-a-Glance
The platelet aggregation test is a laboratory study that measures how well platelets clump together in response to chemical triggers, helping clinicians diagnose inherited and acquired platelet function disorders.
- Processing:
- Spin 1 (Slow): Centrifuge whole blood at ~200g for 10-15 mins to obtain Platelet Rich Plasma (PRP).
- Spin 2 (Fast): Centrifuge remaining blood at ~2000g for 15-20 mins to obtain Platelet Poor Plasma (PPP) (used as the "blank" or 100% transmission baseline).
- Testing:
- Calibrate aggregometer (0% transmission = PRP; 100% transmission = PPP).
- Add specific Agonist (ADP, Collagen, Ristocetin, etc.) to the PRP cuvette.
- Monitor the curve for 6–10 minutes.
- Interpretation:
- Primary Wave: Direct response to agonist.
- Secondary Wave: Response to platelet granule release (secretion).
Introduction
Platelets are tiny cell fragments, but when a blood vessel tears, they are the first responders. The platelet aggregation test asks a simple question: can this patient's platelets do their job? A complete blood count tells you how many platelets there are. The platelet aggregation test tells you whether they actually work.
This matters in the real world. A patient with a normal platelet count can still bleed heavily after a tooth extraction, a tonsillectomy, or childbirth if their platelets cannot clump properly. The platelet aggregation test bridges the gap between quantity and quality, and for many inherited disorders it is the single most informative laboratory study available [1,3].
In the lab, we mimic vessel injury by adding chemical triggers (agonists) to the patient's platelet-rich plasma. By watching how the platelets respond, we can pin down whether the problem lies in adhesion, activation, granule release, or aggregation itself. Diagnoses range from rare inherited disorders such as Glanzmann's thrombasthenia and Bernard-Soulier syndrome to the everyday effects of aspirin.
Why the platelet aggregation test matters
The platelet aggregation test is most useful for:
- Diagnosing qualitative platelet defects in patients with bleeding and a normal platelet count.
- Distinguishing between disorders of adhesion, aggregation, and secretion, which look similar at the bedside but require different management.
- Monitoring antiplatelet therapy or confirming washout before high-risk surgery.
When the test is ordered
Doctors typically order a platelet aggregation test when a patient has:
- Easy or unexplained bruising.
- Prolonged bleeding after surgery, dental work, or minor injury.
- Heavy menstrual bleeding that started at menarche.
- A personal or family history of a bleeding disorder.
Before the lab work, clinicians often score the bleeding history with the ISTH Bleeding Assessment Tool (ISTH-BAT), then run a CBC, peripheral smear, PT, aPTT, and von Willebrand screen. The platelet aggregation test comes next when those tests are normal but bleeding is real [5].
Principle of the Platelet Aggregation Test
The most common method is Light Transmission Aggregometry, or LTA. Gustav Born and John O'Brien developed it independently in 1962, and despite many newer technologies, the principle has not changed [1].
The turbidimetric concept
Platelet-rich plasma (PRP) looks cloudy because suspended platelets scatter light. Add an agonist, and the platelets change shape and stick together. As they form clumps, they fall out of suspension and the plasma clears. The aggregometer detects this change: more light reaches the photodetector as the sample becomes less cloudy.
In short: cloudy plasma = scattered platelets, clear plasma = aggregated platelets.
Setting the baseline
The instrument needs two reference points before the test begins:
- 0% light transmission — the patient's own PRP, which is the cloudiest the sample gets.
- 100% light transmission — the patient's platelet-poor plasma (PPP), which is the clearest.
Calibrating against the patient's own plasma cancels out small differences in plasma color or turbidity between people.
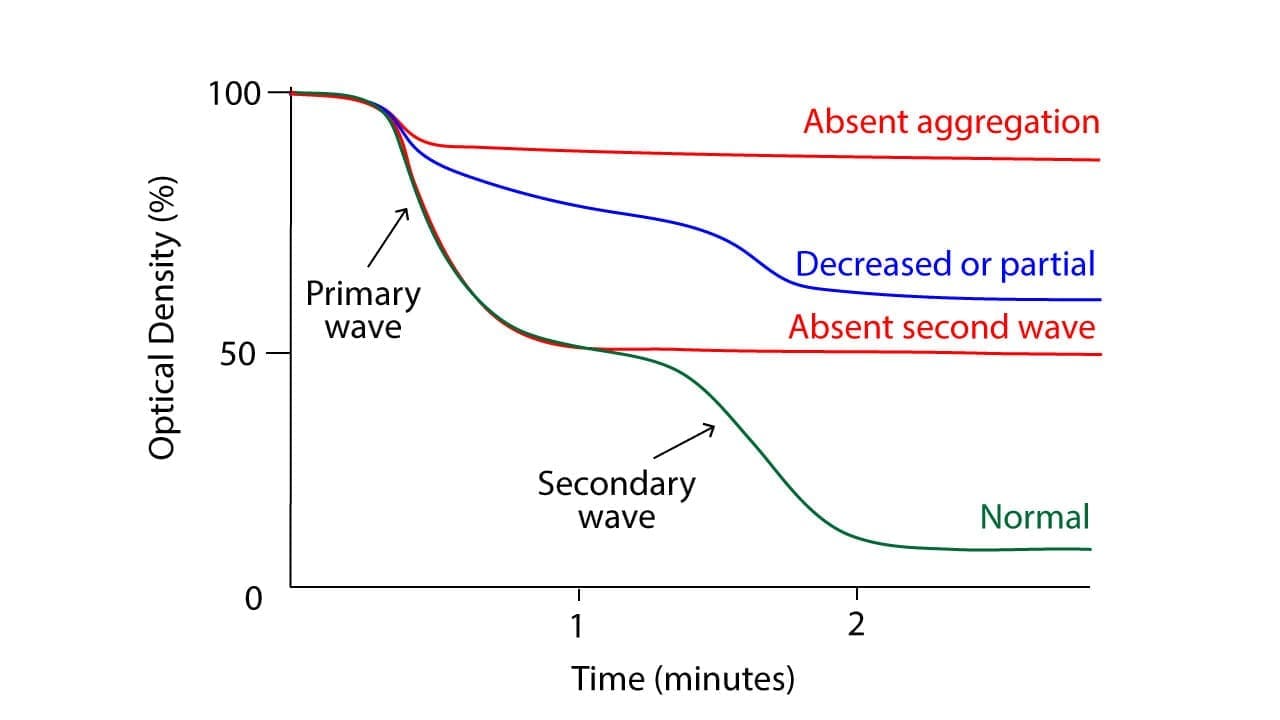
Reading the aggregogram
The aggregogram is a graph of light transmission against time. A normal response to a strong agonist often shows a biphasic curve:
- Primary wave — platelets start to stick together as soon as the agonist binds its receptor.
- Release reaction — activated platelets degranulate, dumping their stored ADP, serotonin, and thromboxane into the surrounding plasma.
- Secondary wave — the released chemicals recruit more platelets, producing a second, larger rise.
Some agonists behave differently. Collagen typically gives a single robust wave because it triggers a massive release reaction immediately. Low-dose ADP may show a primary wave followed by disaggregation if the platelets cannot sustain activation.
Materials
- Platelet-rich plasma (PRP) and platelet-poor plasma (PPP) prepared from the patient and a control.
- Agonists: ADP (2.5 µmol/L), collagen (1.25 µg/mL), epinephrine (5.00 µmol/L), arachidonic acid (1.0 mmol/L), ristocetin sulfate (1.2 mg/mL).
- Aggregometer with 37 °C heating block and stirring function.
- Glass cuvettes with magnetic stir bars.
- Disposable pipettes, test tubes, timer.
- Centrifuge.
- 3.2% (109 mmol/L) trisodium citrate vacutainer tubes (light blue top) [1].
- 37 °C water bath.
Pre-analytical Checklist
This is where most errors happen. Get the pre-analytical phase right and the rest of the test usually follows [1,8].
- Aspirin and NSAIDs: stop for 7–10 days. Aspirin permanently blocks the cyclooxygenase enzyme inside platelets, so the effect lasts the full platelet lifespan.
- Clopidogrel, prasugrel, and ticagrelor: stop for 5–7 days. Note that while ticagrelor is reversible and its effects may wane in 3–5 days, a full 5-to-7-day week is standard practice to ensure complete washout for irreversible P2Y12 inhibitors [9].
- Caffeine and fatty meals: avoid for 12 hours before the draw. Lipemic plasma scatters light and can mimic an abnormal trace.
- Fasting: overnight fast is recommended.
- Blood draw: use a 21-gauge needle with minimal stasis. Discard the first 2–3 mL to avoid tissue factor contamination. Fill the citrate tube to its mark — the 9:1 blood-to-citrate ratio depends on it.
- Time to test: complete all aggregations within 4 hours of collection. PRP rests at room temperature, not on ice.
Protocol
Preparing platelet-rich and platelet-poor plasma
- Collect whole blood into a 3.2% trisodium citrate tube at a 9:1 blood-to-anticoagulant ratio. Two or three tubes (around 4.5 mL each) usually give enough plasma.
- Let the tubes rest undisturbed for 15–30 minutes at room temperature.
- Centrifuge at approximately 200 × g for 10 minutes at room temperature to obtain PRP. This is a soft spin — it leaves platelets suspended in plasma [1].
- Carefully aspirate the upper PRP layer with a plastic pipette. Do not disturb the buffy coat or red cell layer.
- Centrifuge a separate aliquot at 2000 × g for 15 minutes to obtain PPP.
- Place both PRP and PPP in capped tubes and rest them at room temperature. Do not warm PRP for prolonged periods before testing.
- Current ISTH-SSC consensus is to test native, non-adjusted PRP rather than diluting to a fixed platelet count [1]. If your local protocol still adjusts to 200–400 × 10⁹/L, follow it consistently. However, if the patient has severe thrombocytosis (>500 × 10⁹/L), dilution may be required to prevent artifactual trace flattening, whereas testing is generally considered unreliable if the native platelet count falls below 150 × 10⁹/L [1].
Running the aggregation test
- Pre-warm the aggregometer block to 37 °C for at least 30 minutes.
- Place a magnetic stir bar in each cuvette.
- Calibrate: pipette 500 µL of PPP into one cuvette to set 100% transmission, then 500 µL of PRP into another to set 0% transmission. Remove both.
- Pipette 450 µL of PRP (patient and control) into the test channels.
- Set stirring speed to 1000–1200 rpm. Allow the cuvette to warm for 1–3 minutes.
- Add the agonist (e.g., 50 µL of ADP). Start the recording at the moment of addition.
- Run for at least 6 minutes — longer (up to 8–10 minutes) if testing for disaggregation or late secondary waves.
- Repeat with each agonist. Test patient and control in parallel for every agonist.
- Record maximum aggregation, slope, and shape of the curve. Compare against laboratory reference values.
Optional add-on tests
- Lumi-aggregometry measures ATP released from dense granules simultaneously with aggregation. Adding ATP-release measurement to LTA substantially increases diagnostic yield in patients with bleeding of unknown cause by detecting subtle storage pool defects that standard LTA alone misses [4,10].
- Low-dose ristocetin can be used when type 2B von Willebrand disease is suspected.
Interpretation
Normal patterns by agonist
The normal platelet aggregation test response varies by agonist:
- ADP — biphasic. Small primary wave, larger secondary wave driven by released thromboxane A₂ and granule contents.
- Collagen — single, sustained wave after a brief lag phase, because collagen triggers an immediate strong release reaction.
- Ristocetin — rapid agglutination, mediated by von Willebrand factor binding to GPIb. Note: this is agglutination, not true aggregation, which is why Glanzmann's thrombasthenia (a GPIIb/IIIa defect) shows a normal ristocetin response.
- Arachidonic acid — slow rise via the thromboxane A₂ pathway. Aspirin abolishes this.
- Epinephrine — variable, often weak. A poor epinephrine response in isolation is rarely diagnostic on its own.
Abnormal patterns
- Hypersensitivity — increased amplitude or faster onset, suggesting platelet hyperactivity.
- Hyposensitivity — weak or absent response, suggesting impaired function.
- Delayed aggregation — points to a problem in a specific signaling pathway.
- Absent secondary wave — defective thromboxane production or granule release.
Diagnostic Patterns of Abnormal Platelet Aggregation Test
| Disorder | ADP | Collagen | Epinephrine | Arachidonic acid | Ristocetin |
|---|---|---|---|---|---|
| Glanzmann's thrombasthenia | Absent | Absent | Absent | Absent | Normal |
| Bernard-Soulier syndrome | Normal | Normal | Normal | Normal | Absent |
| Von Willebrand disease | Normal | Normal | Normal | Normal | Absent / reduced |
| Aspirin or NSAID effect | No 2nd wave | Reduced | No 2nd wave | Absent | Normal |
| Storage pool disease | No 2nd wave | Reduced | Absent | Reduced | Normal |
Glanzmann's vs. Bernard-Soulier
Glanzmann's gives a flat trace to almost everything but a normal ristocetin response, because ristocetin works through GPIb-vWF and does not need the missing GPIIb/IIIa receptor. Bernard-Soulier is the mirror image: ristocetin fails because GPIb is missing or defective, but everything else aggregates normally. To distinguish between these two clinically similar ristocetin defects, the lab can perform a mixing study: adding normal plasma (which contains functional von Willebrand factor) will correct the aggregation response in von Willebrand disease, but it will not correct the response in Bernard-Soulier syndrome [5].
Technical Artefacts
Several factors can muddy the trace and be mistaken for true platelet dysfunction:
- Poor PRP preparation — aggressive pipetting or contamination with red cells activates platelets before the test starts.
- Temperature drift — outside 37 °C, platelets respond unpredictably.
- Wrong stirring speed — too slow and platelets do not meet; too fast and they shear.
- Lipemic, icteric, or hemolyzed plasma — interferes with light transmission.
- Wrong agonist concentration — high concentrations mask mild defects; low concentrations exaggerate them.
- Calibration error — invalidates the entire run.
- Drug interference — undisclosed aspirin, NSAIDs, or even some herbal supplements (fish oil, garlic, ginkgo) can flatten the curve.
This is why interpretation always combines the aggregogram, the clinical history, and a check for technical artifacts. Pattern across multiple agonists matters more than any single trace.
Where the Platelet Aggregation Test Sits Among Other Methods
LTA is the reference standard, but it is not the only tool. Knowing the alternatives helps explain why LTA is still preferred for diagnosis [6,7].
- PFA-100 / PFA-200 — a screening test that simulates high-shear vessel injury. Quick and useful as an initial screen, but poor at pinpointing specific defects.
- Whole-blood impedance aggregometry (Multiplate) — uses whole blood instead of PRP, faster, often used for antiplatelet drug monitoring.
- VerifyNow — point-of-care, mainly for monitoring aspirin and P2Y12 inhibitors before cardiac procedures.
- 96-well Optimul aggregometry — high-throughput LTA variant with pre-coated agonist plates [7].
- Flow cytometry — measures surface receptors directly; useful for confirming Glanzmann's or Bernard-Soulier.
- Platelet genetic panels — increasingly used when LTA is abnormal but the specific diagnosis is unclear.
Frequently Asked Questions (FAQs)
Why do I need to stop aspirin before the test?
Aspirin permanently disables an enzyme inside platelets for the platelet's whole 7–10-day lifespan. Even a single dose can flatten the secondary wave on the platelet aggregation test, producing a result that looks like a storage pool defect when the platelets are actually fine.
What is the difference between a platelet aggregation test and PT/aPTT?
PT and aPTT measure clotting factors in plasma. A platelet aggregation test measures the platelets themselves as in how well they activate and stick together. A patient can have completely normal PT and aPTT and still have a serious platelet function disorder.
Does a normal platelet count mean my platelets work normally?
No. The count tells you the quantity. The platelet aggregation test tells you the quality. The two are independent.
Which diseases is this test used to diagnose?
Most commonly Glanzmann's thrombasthenia, Bernard-Soulier syndrome, von Willebrand disease, and storage pool disorders. It also helps confirm the effect of antiplatelet drugs.
Is the platelet aggregation test painful?
The blood draw is the same as any other. Because platelets must be tested fresh, the draw is usually done at the specialist laboratory rather than a general collection center.
Can the test be normal in someone who still bleeds?
Yes. LTA can miss subtle granule release defects and mild von Willebrand disease. Add-on tests such as ATP-release lumi-aggregometry, flow cytometry, or genetic panels can pick up some of these missed cases.
Glossary of Related Medical Terms
- Aggregometer — instrument that measures light passing through plasma as platelets clump.
- Aggregogram — the graph of percent transmission over time produced by the aggregometer.
- Agonist — chemical added to the sample to activate platelets, mimicking a vessel injury.
- Biphasic response — aggregation pattern with two waves: primary from the agonist, secondary from internal granule release.
- GPIIb/IIIa (αIIbβ3) — the platelet surface receptor for fibrinogen; missing in Glanzmann's thrombasthenia.
- GPIb-IX-V — the platelet receptor for von Willebrand factor; defective in Bernard-Soulier syndrome.
- ISTH-BAT — bleeding assessment questionnaire used to score a patient's bleeding history.
- LTA (Light Transmission Aggregometry) — gold-standard platelet function test using PRP.
- Lumi-aggregometry — LTA combined with ATP-release measurement.
- PPP (Platelet-Poor Plasma) — plasma with platelets removed; sets the 100% transmission baseline.
- PRP (Platelet-Rich Plasma) — plasma with platelets suspended; the active sample.
- Ristocetin — antibiotic used in the lab to test von Willebrand factor and GPIb function.
- Turbidimetry — measurement of cloudiness by light transmission.
- Von Willebrand factor (vWF) — plasma protein bridging platelets to injured vessel walls.
Disclaimer: This protocol is for educational purposes only. Local laboratory standard operating procedures take precedence. It is not intended to be a substitute for informed professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for clinical decision-making. While the information presented here is derived from credible medical sources and is believed to be accurate and up-to-date, it is not guaranteed to be complete or error-free. See additional information.
References
- Cattaneo, M., Cerletti, C., Harrison, P., Hayward, C. P., Kenny, D., Nugent, D., Nurden, P., Rao, A. K., Schmaier, A. H., Watson, S. P., Lussana, F., Pugliano, M. T., & Michelson, A. D. (2013). Recommendations for the Standardization of Light Transmission Aggregometry: A Consensus of the Working Party from the Platelet Physiology Subcommittee of SSC/ISTH. Journal of thrombosis and haemostasis : JTH, 10.1111/jth.12231. https://doi.org/10.1111/jth.12231
- Hayward, C. P., Moffat, K. A., & Liu, Y. (2012). Laboratory investigations for bleeding disorders. Seminars in thrombosis and hemostasis, 38(7), 742–752. https://doi.org/10.1055/s-0032-1326780
- Koltai, K., Kesmarky, G., Feher, G., Tibold, A., & Toth, K. (2017). Platelet Aggregometry Testing: Molecular Mechanisms, Techniques and Clinical Implications. International journal of molecular sciences, 18(8), 1803. https://doi.org/10.3390/ijms18081803
- Cattaneo M. (2009). Light transmission aggregometry and ATP release for the diagnostic assessment of platelet function. Seminars in thrombosis and hemostasis, 35(2), 158–167. https://doi.org/10.1055/s-0029-1220324
- Gresele, P., & Subcommittee on Platelet Physiology of the International Society on Thrombosis and Hemostasis (2015). Diagnosis of inherited platelet function disorders: guidance from the SSC of the ISTH. Journal of thrombosis and haemostasis : JTH, 13(2), 314–322. https://doi.org/10.1111/jth.12792
- Le Blanc, J., Mullier, F., Vayne, C., & Lordkipanidzé, M. (2020). Advances in Platelet Function Testing-Light Transmission Aggregometry and Beyond. Journal of clinical medicine, 9(8), 2636. https://doi.org/10.3390/jcm9082636
- Chan, M. V., Lordkipanidzé, M., & Warner, T. D. (2023). Assessment of Platelet Function by High-Throughput Screening Light Transmission Aggregometry: Optimul Assay. Methods in molecular biology (Clifton, N.J.), 2663, 627–636. https://doi.org/10.1007/978-1-0716-3175-1_41
- Clinical and Laboratory Standards Institute. (2008). Platelet function testing by aggregometry; Approved guideline (CLSI document H58-A). Wayne, PA: CLSI.
- Valgimigli, M., Bueno, H., Byrne, R. A., Collet, J. P., Costa, F., Jeppsson, A., Jüni, P., Kastrati, A., Kolh, P., Mauri, L., Montalescot, G., Neumann, F. J., Petricevic, M., Roffi, M., Steg, P. G., Windecker, S., Zamorano, J. L., Levine, G. N., ESC Scientific Document Group, ESC Committee for Practice Guidelines (CPG), … ESC National Cardiac Societies (2018). 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). European heart journal, 39(3), 213–260. https://doi.org/10.1093/eurheartj/ehx419
- Dawood, B. B., Lowe, G. C., Lordkipanidzé, M., Bem, D., Daly, M. E., Makris, M., Mumford, A., Wilde, J. T., & Watson, S. P. (2012). Evaluation of participants with suspected heritable platelet function disorders including recommendation and validation of a streamlined agonist panel. Blood, 120(25), 5041–5049. https://doi.org/10.1182/blood-2012-07-444281