Procedure-at-a-Glance
- Processing:
- Spin 1 (Slow): Centrifuge whole blood at ~200g for 10-15 mins to obtain Platelet Rich Plasma (PRP).
- Spin 2 (Fast): Centrifuge remaining blood at ~2000g for 15-20 mins to obtain Platelet Poor Plasma (PPP) (used as the “blank” or 100% transmission baseline).
- Testing:
- Calibrate aggregometer (0% transmission = PRP; 100% transmission = PPP).
- Add specific Agonist (ADP, Collagen, Ristocetin, etc.) to the PRP cuvette.
- Monitor the curve for 6–10 minutes.
- Interpretation:
- Primary Wave: Direct response to agonist.
- Secondary Wave: Response to platelet granule release (secretion).
Introduction
Platelet Aggregation Testing (PAT), specifically Light Transmission Aggregometry (LTA), remains the “Gold Standard” for evaluating platelet function in the clinical laboratory. While a complete blood count (CBC) provides the platelet quantity, it reveals nothing about their quality. The platelet aggregation test (PAT) bridges this gap, providing a dynamic assessment of how well platelets can activate, adhere, and clump together to form a primary hemostatic plug.
In a healthy system, vascular injury exposes subendothelial collagen, triggering a cascade of platelet activation. In the laboratory, we replicate this environment by introducing specific chemical “agonists” to a patient’s Platelet-Rich Plasma (PRP) in the Platelet Aggregation Testing (PAT). By measuring the change in light turbidity as platelets form aggregates in the platelet aggregation test (PAT), clinicians can pinpoint specific biochemical deficiencies, ranging from rare genetic disorders like Glanzmann’s Thrombasthenia to the effects of common antiplatelet medications like Aspirin.
Key Objectives of the Platelet Aggregation Test (PAT)
- Monitor Therapy: Assessing the efficacy of antiplatelet drugs or ensuring their effects have worn off prior to high-risk surgery.
- Identify Qualitative Defects: Diagnosing patients who have normal platelet counts but suffer from unexplained bleeding.
- Differentiate Platelet Disorders: Distinguishing between defects in adhesion (e.g., Bernard-Soulier) versus defects in aggregation or secretion.
Why is the Platelet Aggregation Test (PAT) Important?
The Platelet Aggregation Test (PAT) provides valuable insights into various bleeding disorders like:
- Thrombocytopenia: A low platelet count, leading to excessive bleeding.
- Von Willebrand disease: A genetic disorder impacting the protein that helps platelets adhere to each other and the blood vessel wall.
- Bernard-Soulier syndrome: Another genetic disorder affecting the platelet surface proteins needed for aggregation.
- Antiplatelet medication: Assessing the effectiveness of medications used to prevent blood clots.
When Might the Platelet Aggregation Test (PAT) be Indicated?
The Platelet Aggregation Test (PAT) is often ordered when someone experiences:
- Unexplained or excessive bruising or bleeding.
- Prolonged bleeding after an injury or surgery.
- Recurrent miscarriages.
- A personal or family history of bleeding disorders.
The Platelet Aggregation Test (PAT) is often used in conjunction with other tests and a comprehensive clinical evaluation to form a conclusive diagnosis.
Principle of Platelet Aggregation Test (PAT)
The most common method for performing a Platelet Aggregation Test is Light Transmission Aggregometry (LTA), often referred to as the Born method. This technique is based on turbidimetry by measuring the cloudiness of a sample as light passes through it.
The Turbidimetric Concept
Platelet-Rich Plasma (PRP) is naturally turbid because the suspended platelets scatter light. When a chemical agonist (such as ADP, Collagen, or Epinephrine) is added to the PRP, it triggers the platelets to change shape and stick together.
As these platelets form large clumps (aggregates), they settle out of the suspension, making the plasma increasingly clear. The aggregometer detects this change: as the sample clears, more light passes through the cuvette to the photodetector.
Establishing the Baseline (0% to 100%)
To provide a measurable scale, the instrument must be calibrated using two standards:
- 0% Light Transmission: Set using the patient’s PRP. Since this sample is full of individual platelets, it is the most “cloudy” or opaque state.
- 100% Light Transmission: Set using the patient’s Platelet-Poor Plasma (PPP). Because the platelets have been removed, this represents the “clearest” the sample can possibly become (total aggregation).
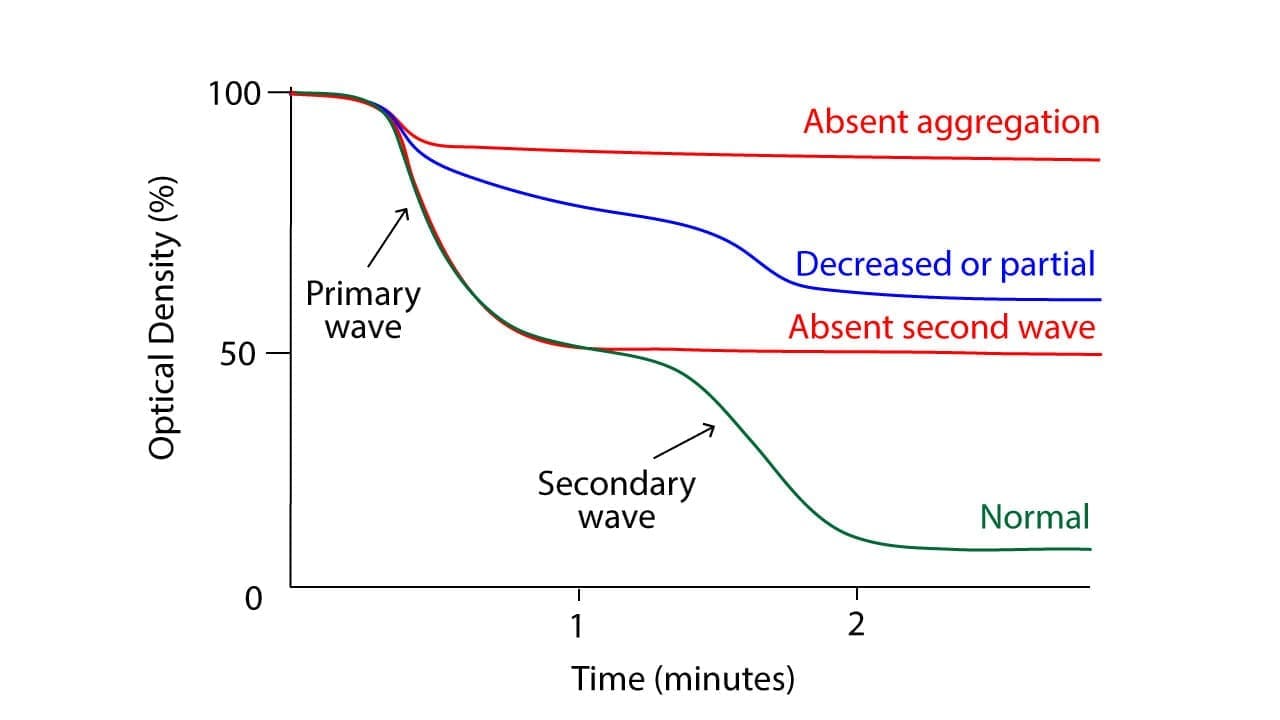
The Aggregogram: Understanding the Curve
The Platelet Aggregation Test (PAT) results are plotted on a graph called an aggregogram, which tracks light transmission over time. A typical normal response often displays a biphasic curve:
- The Primary Wave: Occurs immediately after the agonist is added. This represents the initial response of the platelets as they begin to adhere to one another.
- The Release Reaction: If the stimulus is strong enough, the platelets undergo “degranulation,” releasing their own internal stores of ADP and serotonin.
- The Secondary Wave: The platelets’ own released chemicals recruit even more platelets into the clump, creating a second, larger rise in the curve.
Some agonists, like Collagen, only produce a single, robust wave because they trigger a massive release reaction immediately. Conversely, low doses of ADP might only show a primary wave followed by disaggregation (the clumps falling apart) if the platelets fail to secrete their own granules.
Materials
- Platelet-rich plasma (PRP)
- Agonists: Adenosine disphosphate (ADP) (2.5 µmol/L), Collagen (1.25 µg/mL), Epinephrine (5.00 µmol/L), Arachidonic Acid (AA) (1.0 mmol/L), Ristocetin sulfate (1.2 mg/mL) (optional)
- Aggregation analyzer (aggregometer)
- Calibrator plasma (Control)
- Disposable pipettes
- Test tubes
- Timer
- Centrifuge
- Trisodium citrate vacutainer
- Water bath (37°C)
Protocol
Platelet-Rich Plasma (PRP) Preparation
To ensure accurate results for the platelet aggregation test, patient and control subjects should avoid food, beverages, and medications that could affect platelet function for 10 days before the test and fast overnight prior to sample collection.
For these agonists to provide valid data, the patient’s platelets must be “clean.”
- Aspirin/NSAIDs: Must be discontinued for 7–10 days. These inhibit the Arachidonic Acid pathway.
- Clopidogrel (Plavix): Must be discontinued for 7–10 days. This blocks the ADP (P2Y12) receptor.
- Dietary Interferents: Patients should avoid caffeine and fatty meals for 12 hours prior to the draw, as lipemic plasma can interfere with light transmission.
The test window for platelet aggregation is 30 minutes after PRP preparation and must be completed within 4 hours of blood collection.
- Collect 20 mL whole blood in an trisodium citrate-anticoagulated tube (light blue top). Blood to trisodium citrate ratio should be 9:1.
- Centrifuge the blood at 1500 – 2000 g (3000 rpm) for 15 minutes at room temperature.
- Carefully aspirate the PRP layer without disturbing the buffy coat or red blood cells.
- Pipette the PRP into a test tube and warm it to 37°C in a water bath.
- Centrifuge the remaining blood at 2000 – 2500 g for 20 minutes at room temperature for platelet poor plasma (PPP).
- Carefully aspirate the PPP layer without disturbing the buffy coat or red blood cells.
- Pipette the PPP into a test tube and warm it to 37°C in a water bath.
- Check the platelet count for PRP and carefully dilute the PRP with PPP until the platelet count is approximately 200 – 400 x 109/L.
Platelet Aggregation
- Pre-heat the aggregometer block to 37°C for 30 minutes prior to starting the test.
- Place a magnetic stir bar into each glass cuvette.
- To establish a baseline of 0% and 100%, pipette 500 μL of PPP and PRP, respectively, into separate cuvettes. Measure and then remove them.
- Pipette 450 μL of patient and control PRP into their designated channels (Channel 1: Control, Channel 2: Patient). For each agonist test, prepare a paired set of cuvettes.
- Set the stirring speed to 900 rpm and incubate at 37°C for 3 minutes.
- Monitor the aggregometer baseline and adjust as needed.
- Add the agonist (e.g., ADP) and record the start time for both test and control PRP. Run the aggregometer for a maximum of 8 minutes before stopping the test.
- Repeat the procedure with each agonist at different concentrations, following the manufacturer’s instructions.
- Record the results for each agonist and compare them to the reference values.
Optional Tests
Perform additional platelet aggregation tests with specific inhibitors to identify the cause of abnormal aggregation.
Interpretation
Normal Platelet Aggregation Test Response
The normal platelet aggregation test response varies slightly depending on the agonist used:
- ADP: Triggers a biphasic response. The first phase is a quick, small aggregation due to ADP-mediated activation of receptors. The second phase, larger and delayed, is caused by released thromboxane A2 and further platelet activation.
- Collagen: Induces a rapid, sustained single phase aggregation due to direct activation of collagen receptors on platelets.
- Ristocetin: Mediates a specific clumping through von Willebrand factor (vWF), resulting in a moderate and rapid aggregation.
- Arachidonic Acid: Induces a slow aggregation via the thromboxane A2 pathway, similar to the second phase of the ADP response.
- Epinephrine: Produces a weak and variable aggregation through alpha-adrenergic receptors, primarily seen in high concentrations in the Platelet Aggregation Testing (PAT).
Abnormalities in the aggregogram (the graph depicting platelet aggregation over time) can indicate various platelet function disorders:
- Hypersensitivity: Increased amplitude or faster onset of aggregation suggests platelet hyperactivity or excessive sensitivity to the agonist.
- Hyposensitivity: Weak or absent aggregation implies impaired platelet function or response to the agonist.
- Delayed aggregation: Can indicate abnormalities in specific activation pathways within the platelets.
- Absence of second phase: Suggests defects in thromboxane A2 production or signaling.
Diagnostic Patterns of Abnormal Platelet Aggregation Test
| Disorder | ADP | Collagen | Epinephrine | Arachidonic Acid | Ristocetin |
| Glanzmann’s Thrombasthenia | Absent | Absent | Absent | Absent | Normal |
| Bernard-Soulier Syndrome | Normal | Normal | Normal | Normal | Absent |
| Von Willebrand Disease (vWD) | Normal | Normal | Normal | Normal | Absent/Reduced |
| Aspirin / NSAID Effect | No 2nd Wave | Reduced | No 2nd Wave | Absent | Normal |
| Storage Pool Disease | No 2nd Wave | Reduced | Absent | Reduced | Normal |
Technical Artefacts
Several factors can influence the platelet aggregation test results and be misinterpreted as abnormalities:
- Improper platelet-rich plasma (PRP) preparation: Can lead to platelet activation or decreased concentration, affecting aggregation.
- Temperature variations: Outside the optimal range (usually 37°C) can alter platelet activity.
- Stirring speed: Incorrect stirring can affect platelet interaction and aggregation dynamics.
- Agonist concentration: Improper concentration can lead to over- or under-stimulation of platelets.
- Instrument calibration: Errors in calibration can skew the measured aggregation values.
Therefore, interpreting platelet aggregation test results requires careful consideration of the entire aggregogram, clinical context, and potential technical artefacts. Evaluating the response to different agonists further aids in differentiating specific platelet function disorders.
Note: This is a general overview of the Platelet Aggregation Testing (PAT), and specific interpretation of results depends on the laboratory’s reference values and established practices. Always consult a qualified healthcare professional for diagnosis based on individual results.
Frequently Asked Questions (FAQs)
Why do I need to stop taking Aspirin before the test?
Aspirin permanently disables platelets for their entire lifespan (7-10 days). Even a single dose can block the “secondary wave” of aggregation, leading to false abnormal Platelet Aggregation Testing (PAT) results that look like a storage pool defect.
What is the difference between Platelet Aggregation and PT/PTT?
PT and PTT measure the clotting factors (proteins in the plasma) like Factor VIII or Factor IX. The Platelet Aggregation Test measures the function of the platelets (cells) themselves. You can have a normal PT/PTT but still have a severe platelet function disorder.
Does a normal platelet count mean my platelet function is normal?
No. You can have a normal number of platelets (Quantity) but they may not work properly (Quality). This Platelet Aggregation Testing (PAT) checks the quality of your platelets.
What diseases are diagnosed with this Platelet Aggregation Testing (PAT)?
It is primarily used to diagnose Glanzmann’s Thrombasthenia, Bernard-Soulier Syndrome, Von Willebrand Disease (vWD), and Storage Pool Diseases.
Is the Platelet Aggregation Testing (PAT) painful?
No more than a standard blood draw. However, because the platelets must be fresh, the blood is often drawn at the specialized laboratory rather than a general collection center.
Glossary of Related Medical Terms
- Agonist: A biochemical substance (like ADP or Collagen) added to the blood sample to “trick” platelets into thinking there is an injury, forcing them to activate and clump together.
- Aggregometer: The specialized instrument used to measure the rate and extent of platelet clumping. It typically uses a light source to detect how clear the sample becomes as clots form.
- Biphasic Response: An aggregation pattern with two distinct waves. The Primary Wave is caused by the external agonist added, and the Secondary Wave is caused by the platelets releasing their own internal granules to recruit more platelets.
- Lag Phase: The brief delay between adding the agonist and the start of aggregation (often seen with Collagen).
- LTA (Light Transmission Aggregometry): The “Gold Standard” method for testing platelet function using Platelet Rich Plasma (PRP).
- Platelet Poor Plasma (PPP): Plasma with very few platelets, obtained by high-speed centrifugation. It is used to calibrate the machine to “100% light transmission.”
- Platelet Rich Plasma (PRP): Plasma with a high concentration of platelets, obtained by low-speed centrifugation. This is the active sample used for testing.
- Ristocetin: An antibiotic (no longer used clinically) used in the lab to test if Von Willebrand Factor (vWF) is working correctly. It causes platelets to agglutinate in the presence of vWF.
Disclaimer: This protocol is intended for informational purposes only and may need to be modified depending on the specific laboratory procedures and patient circumstances. Always consult with a qualified healthcare professional for guidance. See additional information.
References
- Koltai K, Kesmarky G, Feher G, Tibold A, Toth K. Platelet Aggregometry Testing: Molecular Mechanisms, Techniques and Clinical Implications. Int J Mol Sci. 2017 Aug 18;18(8):1803. doi: 10.3390/ijms18081803. PMID: 28820484; PMCID: PMC5578190.
- https://practical-haemostasis.com/Platelets/platelet_function_testing_lta.html
- Saba HI, Roberts HR. Hemostasis and Thrombosis: Practical Guidelines in Clinical Management (Wiley Blackwell). 2014.


